

Preprocedure
Most hepatic arteriovenous shunts (HAVS) associated with hepatocellular carcinoma (HCC) occur with advanced stage liver cancer, and these patients typically have a dismal prognosis. Transcatheter arterial embolization (TAE) in this population carries significant risk. Therefore, proper patient selection is critical to determine which patients may benefit from TAE. The Child-Pugh score should be calculated because TAE is poorly tolerated in HCC patients with Child-Pugh class C. We choose transcatheter arterial infusion instead of TAE for those patients. In patients with elevated liver enzymes in addition to increased serum bilirubin levels, there is a propensity for hepatic failure and thus TAE may be contraindicated.
Cross-sectional imaging with computed tomography scanning or magnetic resonance imaging should be performed. Cross-sectional imaging demonstrates the size of tumor, portal venous or hepatic venous invasion, tumor thrombus, and it allows for accurate preprocedural planning. In patients with a tumor burden >70% of total liver volume, TAE is relatively contraindicated. If massive tumors compress bile ducts and cause bile duct obstruction, biliary decompression should occur prior to TAE. Portal venous thrombosis is also a relative contraindication. Finally, in patients with significant HAVS, it is desirable to occlude the shunts by TAE, especially if there is good collateral flow or superselective embolization is performed.
HCC invades portal veins and/or hepatic veins that lead to HAVS and simultaneously leads to venous tumor thrombus. Hepatic angiography demonstrates abnormally early opacification of portal vein and/or hepatic vein branches, with linear opacification showing typical “thread and streak” signs as well as filling defects in the portal/hepatic venous systems.
Procedure
Hepatic Arterial Angiography
Under local anesthesia, the femoral artery is accessed using the Seldinger technique. The celiac trunk and the superior mesenteric artery are respectively selected, and arteriography is performed to evaluate the liver arterial vasculature and portal vein patency. The common hepatic artery is catheterized, and a selective angiogram is performed to identify arterioportal venous shunts (APVS) or arteriohepatic venous shunts (AHVS); if present, the artery supplying and the vein draining the shunt are identified. APVS can be categorized into central, peripheral, and mixed HAVS. Although anatomically useful, the classification does not reflect the hemodynamics of the HAVS. Consequently, it has little value for shunt embolization. In our experience, HAVS is classified into three types according to the timing of visualization of the venous structures on arteriogram images. For high-flow HAVS, the time of appearance of the vein is between 0.5 and 1.5 seconds (Fig. 1). For intermediate-flow HAVS, the time of appearance of the vein is between 1.5 and 3 seconds. Finally, for low-flow HAVS, the time of appearance of the vein is >3 seconds following arterial injection (Fig. 2). This classification is important because the size of the embolic agent used is determined largely by this scheme.
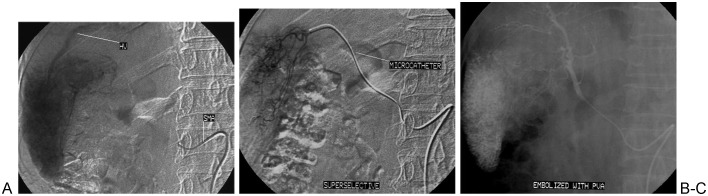
Figure 1.

High-flow arterioportal venous shunts (APVS) associated with hepatocellular carcinoma. (A) The proper hepatic artery angiogram demonstrates opacification of the main portal vein (PV) during the early arterial phase. (B) The entire portal vein (PV) is patent. (C) Preembolization superselective angiography of feeding artery to shunts. (D) Following embolization with 750 to 1000 μm polyvinyl alcohol particles, common hepatic artery angiography demonstrates complete obliteration of APVS.
Figure 2.
Low-flow arteriohepatic venous shunts (AHVS) associated with hepatocellular carcinoma. (A) Right hepatic artery originates from the superior mesenteric artery (SMA); angiography demonstrates opacification of the right hepatic vein in the late arterial phase. (B) Superselective angiography of feeding artery to shunts. (C) Chemoembolization was performed, after which the feeding artery was embolized with 250 to 350 μm polyvinyl alcohol (PVA).
Choice of Embolic Agents
In the past, we used gelatin sponges, coils, absolute ethanol, and polyvinyl alcohol (PVA) particles for shunt embolization in patients with HCC. Since 2002, we prefer to use PVA particles for HAVS. According to the timing of visualization of HAVS, we choose different size PVA particles to occlude the shunt (Table 1).
Table 1. Relationship between Classification of Hepatic Arteriovenous Shunts and Polyvinyl Alcohol Particle Size.
| Timing of Venous Opacification | HAVS Type | PVA Particle |
|---|---|---|
| >3 seconds | Slow flow | 250–350 μm |
| 1.5–3 seconds | Intermediate flow | 350–510 μm |
| 0.5–1.5 seconds | High flow | 750–1000 μm |
PVA, polyvinyl alcohol; HAVS, hepatic arteriovenous shunt.
Shunt Embolization
Superselective catheterization of supplying arteries to the arteriovenous shunts is key to success for HAVS embolization. It may be difficult, however, to identify the feeding arteries for some high-flow HAVS. In such a situation, each suspicious hepatic artery is selected in sequence, and angiography is performed for each one. A microcatheter often must be used to catheterize superselectively each target artery. PVA particles are injected into each feeding artery until flow via the shunts is significantly decreased. Following shunt embolization, 1 mL of chemotherapy lipiodol suspension (lipiodol mixed with epirubicin, oxaliplatin, and mitomycin) is carefully administered in the supplying artery. If fluoroscopy demonstrates significant lipiodol retention in the tumor tissue, more lipiodol suspension is subsequently administered in the target artery until stasis is achieved. After chemoembolization, additional PVA is injected into the supplying artery if shunts are again visualized until all shunts have resolved. A postembolization angiogram via the common hepatic artery is performed to confirm the occlusion of all shunts.
Many types of embolic agents have been used to occlude HCC-associated HAVS. Common agents include gelatin sponges and coils or a combination of both agents. Although immediate complete occlusion can be achieved with a gelatin sponge, the recanalization rate of shunts is appreciable within 3 to 4 weeks after TAE. Coiling causes occlusion proximal to shunts that may lead to recanalization of the HAVS collaterals. In our experience, PVA is a relatively effective embolic agent for HCC-associated HAVS; moreover, the appropriate size PVA can be used in occluding shunts according to the degree of HAVS shunting.
HAVS in the setting of main portal vein tumor thrombosis is not a contraindication for shunt embolization (Fig. 3). Under these circumstances, the following therapeutic strategies are often considered. If there is adequate collateral flow to the portal venous system, shunt embolization can be performed as previously described. If there is poor collateral flow to the portal venous system, however, staged procedures are usually performed at 1-month intervals to allow patients time to recover. In some settings it may be desirable to recanalize the main portal vein by stenting before TAE is performed.
Figure 3.

Hepatocellular carcinoma with arteriohepatic venous shunts (APVS) complicated by main portal vein tumor thrombus. (A) Proper hepatic angiography demonstrates early opacification of the portal vein with thread and streak signs. (B) Superselective angiography of the middle hepatic artery. (C) Spot fluoroscopic embolization with chemotherapy lipiodol suspension and 350 to 510 μm polyvinyl alcohol particles. (D) APVS were completely occluded.
In patients with HAVS complicated by hepatic vein or inferior vena cava (IVC) tumor thrombus, shunt embolization and tumor thrombus chemoembolization may cause tumor thrombus necrosis and subsequent thrombus migration, leading to an acute pulmonary embolism. Therefore, in these settings it is judicious to compress the hepatic vein or IVC tumor thrombus with a stent prior to the embolization of the HAVS.
Postprocedure
In the postprocedure period, impaired liver function caused by HAVS embolization may be seen for 5 to 7 days. Liver and kidney function is monitored every 3 to 5 days until recovery. Prophylactic antibiotics are typically not used before or after the HAVS procedure, although antiemetics are routinely administrated. Transdermal fentanyl is placed 3 hours before the procedure for pain control and continued for 7 days. Regular follow-up including imaging, α-fetoprotein levels, and liver and kidney function is necessary to evaluate for tumor response, to find recurrent or metastatic lesions, and to plan for future therapy. Cross-sectional imaging is obtained 4 weeks after the procedure. If there are residual HAVS and/or tumor thrombus, the patient will return for repeat treatment.
Discussion
Vascular invasion leading to portal or hepatic vein tumor thrombus is one of the pathological mechanisms leading to the development of HAVS. Effective treatment for tumor thrombus is one measure used to completely eliminate HCC-associated HAVS. Thus for HCC patients with HAVS, shunts should be completely occluded while chemical lipiodol suspension is used to treat tumor thrombus as much as possible. However, it is difficult to determine when chemoembolization should be performed; for instance, if chemotherapy lipiodol suspension is given after inadequate shunt embolization, only embolization distal to the level of the shunt may occur. Special attention must be given to AHVS due to the possibility of causing a pulmonary embolism or, more rarely, systemic embolism via a right-to-left shunt. In our experience, small aliquots of lipiodol suspension can be carefully injected into the supplying artery under fluoroscopy after shunt flow becomes very slow. Once most of the injected lipiodol travels distal to the shunt vessels, chemoembolization should terminate immediately. However, if most of the lipiodol retention is noted in tumor tissue, more lipiodol suspension may be administered into the target artery.
Acute liver failure is a severe complication of shunt embolization. It usually occurs in HCC patients with complete main portal vein occlusion without adequate collateral flow. Superselective catheterization of supplying arteries can maximally decrease the likelihood of normal liver tissue damage and effectively avoid liver function failure. Staged procedures are also one method used to prevent hepatic failure.