

Abstract
Purpose
To determine whether three aspects of the word learning process—fast mapping, retention, and extension—are problematic for children with cochlear implants (CIs).
Method
We compared responses of 24 children with CIs, 24 age-matched hearing children and 23 vocabulary-matched hearing children to a novel object noun training episode. Comprehension and production were measured immediately following training (fast mapping) as well as one day later (retention). Extension was measured in terms of the ability of the participants to identify new (untrained) exemplars.
Results
Compared to their hearing age-mates, children with CIs performed marginally more poorly on fast mapping as measured by the comprehension probe and more poorly on retention as measured by comprehension and production probes. The age-mates improved over the retention interval but the children with CIs did not. Most of the children with CIs performed similarly to their age-mates on extension but two children underextended and five failed to understand the task. Compared to younger vocabulary-matched peers, children with CIs did not differ at fast mapping, retention, or extension.
Conclusions
Children with CIs demonstrated deficits in word learning, with retention being especially problematic. Their learning did not differ from that of younger children with similarly sized vocabularies.
Children with cochlear implants (CIs) typically have smaller receptive and expressive vocabularies than their same-age hearing peers (Hayes, Geers, Treiman, & Moog 2009; Geers, Moog, Biedenstein, Brenner, & Hayes, 2009; Johnson & Goswami, 2010). In addition, there is evidence that children with CIs show slower rates of vocabulary growth compared to hearing children (Blamey et al., 2001; Connor, Hieber, Arts, & Zwolan, 2000). Unfortunately, these delays in vocabulary may have a cascading effect on academic success in general and reading outcomes in particular as oral vocabulary skill is related to success in learning to read in the general population (NICHD, 2000; Rayner, Foorman, Perfetti, Pesetsky, & Seidenberg, 2001) and is predictive of reading attainment in children with CIs (Connor & Zwolan, 2004; Johnson & Goswami, 2010).
Prior to implantation, children with prelingual deafness experience a period of auditory deprivation which limits their access to spoken words. It is often hypothesized that longer periods of auditory deprivation will result in greater delays in vocabulary size. This hypothesis is supported in studies demonstrating a negative relationship between age at implantation and vocabulary size (e.g., Connor, Craig, Raudenbush, Heavner, & Zwolan, 2006; Connor et al., 2000; James, Rajput, Brinton, & Goswami, 2007). The length of auditory deprivation also appears to affect growth rates in vocabulary. For example, Kirk et al. (2000) examined vocabulary acquisition at post-implant intervals and found a significant age-at-implantation effect: children implanted prior to age 2 showed steeper growth rates than children implanted between 5 and 7 years of age. Currently, the general consensus among CI researchers is that receiving a CI after age two is late implantation, whereas receiving a CI before one year of age is early implantation (Tomblin, Barker, & Hubbs, 2007).
In many cases, children with CIs continue to build their vocabularies more slowly than children with normal hearing even after they receive their CIs. Using gains in age-equivalency scores on standardized vocabulary tests as a dependent variable, Connor et al. (2000) reported that children who are pre-lingually deaf and who wear CIs average .45 years of gain in receptive vocabulary and .67 years of gain in expressive vocabulary per calendar year regardless of educational method (oral or total communication). Just as for static measures, variance around these mean growth rates is related, in part, to age at implantation, with children who were implanted earlier showing faster growth rates than children who were implanted later (Connor et al., 2000). Moreover, growth trajectories for earlier and later-implanted children differ in slope in that those implanted early experienced a burst of vocabulary growth immediately after implantation but later-implanted children did not (Connor et al., 2006).
That said, early implantation does not ensure adequate vocabulary development in all CI users. Even in ideal circumstances, many children with CIs experience vocabulary deficits. For example, among 5- and 6-year olds who were implanted, on average, by 2.5 years of age and received early intervention and consistent audiological management, half did not develop age-appropriate vocabulary skills by school entry (Hayes et al., 2009).
To date, investigations of vocabulary skills among children with CIs are largely of two types: comparisons to hearing age mates at one point in time or comparisons to age mates (or, more precisely, to age-appropriate published norms) at multiple points over time. Both methods typically employ standardized test scores as the dependent variable. Although these types of studies have clearly demonstrated vocabulary deficits among children with CIs, they provide little insight into the process of word learning that may contribute to lexical deficits. These types of studies also tell us little about how to treat lexical deficits. We maintain that treatment must be guided by a more precise understanding of the processes of word learning that are problematic for children with CIs. The current study is a step in that direction.
Word Learning
The learning of a single word unfolds over time as the learner encounters the word in multiple and varied contexts. Via those encounters word forms, word meanings, their receptive linkage (form-to-meaning), and their expressive linkage (meaning-to-form) are stored in lexical memory (Gupta, 2005). In the current study, we explored three processes involved in word learning—fast mapping, extension, and retention—among children with and without CIs.
Fast mapping
The ability to link a word to its referent after only a few exposures is termed fast mapping (Carey, 1978). In Carey’s original conceptualization, fast mapping depended upon the child’s ability to infer that linkage by making use of linguistic and non-linguistic information in the environment. In later work, the term fast mapping has also been applied to the child’s learning of the word-referent link in response to didactic exposures (Swingley, 2010). Therefore, in current parlance, fast mapping is best thought of as the child’s first connection between a word and its referent.
Fast-mapped representations are highly underspecified in meaning (Carey, 1982) and form (Kay-Raining Bird & Chapman, 1998). They are often strong enough to support above-chance-level performance on a forced choice recognition test (e.g., the child can select the correct referent from an array of objects when the examiner requests it by name) but they are rarely strong enough to support less scaffolded performances such as naming (Dollaghan, 1985; Gray, 2003; Gupta, 2005; Horst & Samuelson, 2008). Even when the fast mapping episode involves as many as 12 exposures to each new word form, young children are typically unable to label referents with these new words (Booth, McGregor, & Rohlfing, 2008).
The success of fast mapping varies across individuals. One factor contributing to this variance is the developmental status of the child’s extant lexicon. Familiar words can trigger (Storkel, Armbrüster, & Hogan, 2006) and scaffold (Storkel, 2001) memory for new words and aid integration of these new memories into the existing lexicon (Storkel et al., 2006). Children with larger vocabularies are better fast mappers than children with smaller vocabularies; this is true of both hearing children (McGregor, Sheng, & Smith, 2005; Mervis & Bertrand, 1994) and children who are deaf or hard-of-hearing (Lederberg & Spencer, 2009).
Extension
With the exception of proper names, all words refer to categories of referents. The word dog labels referents as diverse as Schnoodles, Irish Setters, and Great Danes but it cannot refer to Siamese or Calico cats. Therefore, another important process involved in learning a word is determining its correct category extension. Although exact category boundaries likely require multiple exposures to words and their referents (and their non-referents) over time, by approximately 15 months of age, children have a basic understanding that words can refer to categories and, upon hearing a single referent named, they can extend to multiple exemplars of that referent based on that understanding (Hirsh-Pasek, Golinkoff, & Hollich, 1999; Imai & Gentner, 1997; Landau, Smith, & Jones, 1988). By two years of age, they have developed a heuristic by which they tend to extend new object labels to all similarly shaped objects (Behrend, Scofield, & Kleinknecht; 2001; Landau et al., 1988; Imai & Gentner, 1997). The emergence of the shape bias is positively associated with the number of nouns that the child has in his or her vocabulary (Samuelson & Smith, 1999) and it affects extension behavior in tasks that tap comprehension (Samuelson & Smith, 1999) and production (Samuelson & Smith, 2005).
Retention
Successful word learning involves not only fast mapping and extension but also retention. Memories develop over time and fast-mapped memories are notoriously fragile (Horst & Samuelson, 2008; Munro, Baker, McGregor, Dockering, & Arcuili, 2012). Consider the work of Horst and Samuelson (2008) who presented two-year-olds with a fast-mapping paradigm, followed by a 5-minute delay, and then presentation of a retention/extension paradigm. Participants had no difficulty recognizing word-object pairings in the fast-mapping paradigm, but they were unable to name any of the objects after two exposures to the novel label. In addition, they could not retain or extend novel labels at above-chance levels unless the novel objects were manipulated and ostensively named by the experimenter prior to the retention test. In other words, only when the examiners enhanced saliency of the referent via manipulation and the word via repeated naming did the children establish a fast-mapped representation that was strong enough to resist decay over the short retention interval.
Fast mapping, extension, and retention among children with CIs
Our understanding of the word learning process among children with CIs is limited but three recent studies, Tomblin, Barker, and Hubbs (2007), Willstedt-Svensson et al. (2004), and Lederberg and Spencer (2009), offer some insights. In all three, children were presented with an unfamiliar object in the context of familiar objects. There was no direct teaching; rather, the child was asked to select the objects one at a time as each was named (e.g., Hide the fork, Where’s the koob). The child had to infer that the unfamiliar object was named by the novel word form.
Tomblin et al. (2007) measured fast mapping by posttests that involved a measure of comprehension in which the child had to select the newly mapped referent from an array of objects upon hearing its newly mapped name and a measure of production in which the child was asked to name each of the newly mapped referents (if possible) or to select the correct name from among three options (if independent naming was not possible). They found a comprehension and production composite score to differentiate 2-to-5-year olds with CIs from their normal hearing age-mates. The children with CIs earned scores that ranged from 0 to 6 (with 6 being the highest possible score) and that averaged 2.0. Although the range of scores earned by the children with normal hearing was similar at 1 to 6, the average was significantly higher at 3.86. This constitutes evidence of deficiencies in fast mapping among children with CIs.
Willstedt-Svensson et al. (2004) employed the same posttests measures as Tomblin et al. (2007) but they also included a second round of posttests 30 minutes after the first. Over this brief delay, the performance of the participants, all of whom were school-aged children with CIs, declined. Although the significance of this decline was not tested statistically, working from Table 2 (Willstedt-Svensson et al., 2004, p. 509), it can be determined that the effect size of the difference is moderate (d = .76). Because Willstedt-Svensson et al. did not include a comparison group of normal hearing age-mates, we do not know whether this decline would also characterize hearing children.
Table 2.
Demographic information about the participants. Mean scores (and standard deviations) are provided for each measure.
| CI | AM | VM | |
|---|---|---|---|
|
|
|||
| Chronological age | 4.86 (1.04) | 4.88 (1.02) | 3.74 (1.02) |
| PPVT raw score | 52.5 (19.9) | 82.8 (19.2) | 54 (18.3) |
| PPVT standard score | 90.2 (14.8) | 116.0 (10.6) | 106.1 (8.2) |
| KBIT standard score | 99.8 (12.9) | 100.2 (12.4) | 102.9 (8.03) |
| MCDI quotient score | 1.34 (0.24) | 1.28 (0.22) | 1.41 (0.37) |
| Maternal education level | 14.87 (3.25) | 16.35 (2.17) | 16.65 (1.7) |
To be credited with learning in Lederberg and Spencer (2009), children had to demonstrate comprehension of the new word form in reference to the trained exemplar and an untrained exemplar, that is, they had to extend the new word. Their participants were 98 deaf or hard-of-hearing children ranging from two- to seven years of age. Twenty-three of these children wore CIs and 11 of them were able to map and extend in response to the fast mapping episode that required inference of the word-to-referent link. An additional eight could map and extend when the fast mapping episode was modified to be more didactic (i.e., the examiner provided three additional exposures to the word form and she clearly identified the word-to-referent link by using eye gaze, pointing, and object manipulation while labeling). The variability of performance was positively related to size of the extant lexicon. The children who failed to demonstrate fast mapping and extension were reported by their teachers to produce fewer than 100 words (via speech or sign), on average, whereas those who were successful averaged more than 100.
Hypotheses and predictions
In the current study, we exposed children to novel words and their unfamiliar object referents in a didactic fast mapping episode, then immediately probed their comprehension and production of these newly presented words to determine the amount of information they had fast mapped. We also probed their ability to recognize other (untrained) exemplars of the same referent to determine their ability to extend the newly mapped words. Finally, we repeated these probes after a period of 1–3 days to determine retention. We compared children with CIs to children with normal hearing who were either the same chronological age as those with CIs or similar in vocabulary development to those with CIs.
We hypothesized that access to a clear acoustic signal is crucial to optimal fast mapping. Because children with CIs are known to be limited in this regard, we predicted that they will perform more poorly than their age-mates with normal hearing on measures of fast mapping.
We hypothesized that perception of shape and the recognition that object categories are organized by shape are crucial to optimal extension of object labels. Because children with CIs have adequate access to visual information and (at the age we tested) have more than 100 words in their expressive lexicons and adequate experience with object labels, we predicted that they will perform similarly to their age-mates with normal hearing on measures of extension.
We hypothesized that retention over time is determined by multiple factors including the integrity of initial encoding and the integrity of the extant memory network (i.e., the current lexicon). As a result of incomplete access to auditory information and reduced vocabulary size, we predicted that children with CIs will be less likely than their peers to retain the information that they have fast mapped. That said, there is no firm empirical basis for this prediction and we view this aspect of the study as exploratory.
Finally, we hypothesized that multiple processes involved in word learning in the moment are supported by the extant word knowledge the learner brings to that moment. Because we populated the second comparison group with young children with normal hearing who have similar vocabulary sizes as the children with CIs, we predicted that their profiles of learning on the mapping, extension, and retention tasks would also be similar.
Methods
Participants
Twenty-four children with CIs (15 males, 9 females) were recruited from private deaf oral education schools in the Midwest. Twenty participated in two data collection sessions; four children completed only the first session, due to illness or scheduling conflicts. Testing took place at the children’s schools, with the exception of one child who participated at a hospital following CI programming. Prior to participation in the study, teachers or audiologists checked the devices of the children to ensure that they were working correctly.
All children with CIs were between the ages of 3 years, 6 months and 6 years, 9 months at their time of participation (mean age = 4.86 years, SD = 1.04 years). Spoken English was the primary language for all CI participants; however, two children also spoke Spanish, one spoke Russian, one spoke Romanian, and one was exposed to American Sign Language. Table 1 displays demographic information for the CI group, including age at implantation, length of device use, and device type.
Table 1.
CI participant characteristics (N = 24)
| Participant ID | Age at test (years) | Age at CI (years) | Length of CI use (years) | Device Type |
|---|---|---|---|---|
| CI 008 | 3.67 | 1.92 | 1.75 | Nucleus Freedom |
| CI 009 | 4.33 | 0.75 | 3.58 | Nucleus Freedom |
| CI 010 | 4.42 | 1.42 | 3.00 | Auria Harmony |
| CI 011 | 4.42 | 1.42 | 3.00 | Auria Harmony |
| CI 012 | 5.5 | 1.33 | 4.17 | Nucleus Freedom |
| CI 013 | 4.5 | 1.17 | 3.25 | Nucleus Freedom |
| CI 014 | 3.17 | 0.75 | 2.33 | Nucleus Freedom |
| CI 015 | 3.33 | 1.67 | 1.67 | Nucleus Freedom |
| CI 016 | 4.00 | 2.00 | 1.92 | Nucleus Freedom |
| CI 017 | 6.42 | 2.92 | 3.42 | Nucleus Freedom |
| CI 018 | 4.08 | 1.42 | 2.67 | Nucleus Freedom |
| CI 019 | 5.58 | 1.58 | 4.00 | Nucleus Freedom |
| CI 020 | 4.42 | 1.33 | 3.08 | Nucleus Freedom |
| CI 024 | 5.00 | 1.83 | 3.08 | Auria Harmony |
| CI 025 | 5.92 | 1.00 | 5.92 | Nucleus Freedom |
| CI 026 | 6.75 | 1.58 | 5.17 | Nucleus Freedom |
| CI 027 | 3.25 | 1.50 | 2.33 | Auria Harmony |
| CI 028 | 4.58 | 1.92 | 2.58 | Nucleus Freedom |
| CI 029 | 4.83 | 1.50 | 2.42 | Nucleus Freedom |
| CI 030 | 5.33 | 1.92 | 3.42 | Nucleus Freedom |
| CI 031 | 5.42 | 2.25 | 3.08 | Nucleus Freedom |
| CI 032 | 5.00 | 1.75 | 3.25 | Nucleus Freedom |
| CI 033 | 6.42 | 2.83 | 3.42 | Nucleus Freedom |
| CI 034 | 6.33 | 1.33 | 4.92 | Nucleus Freedom |
| Mean | 4.86 | 1.68 | 3.16 | |
| Range | 3.33–6.75 | 0.75–2.92 | 1.67–5.92 | |
| SD | 1.04 | 0.5 | 1.07 |
All children with CIs had prelingual onset of deafness (prior to 12 months of age), bilateral severe-to-profound sensorineural hearing loss, and no diagnosed cognitive or learning disabilities. All participants received a CI prior to 3 years of age, and had a minimum of 1 year of experience with their CIs. The average age at initial stimulation was 1.68 years (SD = 0.50) and the average length of CI use was 3.16 years (SD = 1.07). Thirteen participants had sequential bilateral CIs, 9 had unilateral CIs only, and 3 had bimodal configurations (CI + hearing aid on contralateral ear).
We recruited 47 children with normal hearing from the local community. All completed both visits. Twenty-four children (15 males, 9 females) served as age-matched (AM) control participants (mean age = 4.88 years, SD = 1.02 years). An additional 23 children (12 males, 11 females) served as vocabulary-matched (VM) control participants (mean age = 3.74 years, SD = 1.02 years). The VM group contained one less participant than the CI and AM groups because one CI participant did not complete vocabulary testing due to behavioral issues. One child in the AM group spoke Spanish and one child in the VM group spoke Romanian; all others were exposed only to English. English was the primary language for all NH participants.
Standardized Language and Cognitive Test Measures
Nonverbal cognitive abilities were measured with one of two tests, depending on the age of the participant. The non-verbal matrices of the Kaufman Brief Intelligence Test (KBIT-2; Kaufman & Kaufman, 2004) were administered to participants who were 4;0 and older. The Situation-Comprehension subtest of the Minnesota Child Development Inventory (MCDI; Ireton & Thwing, 1974) was administered to participants who were younger than 4;0. The Peabody Picture Vocabulary Test-III (PPVT-III; Dunn & Dunn, 1997) was used to measure receptive vocabulary skills.
Table 2 displays mean scores and standard deviations for age and nonverbal cognitive and language measures for the three groups. By design, the CI group was well-matched to the AM group on chronological age, t(45) = .285, p = .78, and to the VM group on PPVT-III raw scores, t(44) = .27, p = .79. We also analyzed standard scores on the PPVT-III. The AM group had significantly higher standard scores than the CI group, t(45) = 6.88, p < .000, but it should be noted that the CI group demonstrated mean standard scores within the average range of performance (M = 90.22; range 55–116; SD = 14.8).
The CI group showed no significant difference in KBIT-2 standard scores compared to the AM group, t(37) = .102, p = .92, or the VM group, t(24) = .59, p = .56. We also analyzed quotient scores on the MCDI Situation-Comprehension subtest. The CI group showed no significant difference in MCDI quotient scores with the AM group, t(34) = −.76, p = .46, or the VM group, t(37), .69, p = .50.
Maternal education was calculated as a continuous variable, in which we determined the number of years of education for the mother of each participant. Results of t-tests for independent samples approached significance for the CI and AM groups, t(45) = 2.008, p = .051, and reached significance for the CI and VM groups, t(44) = 2.331, p = .024, with the mothers of children in the CI group having less education than the other mothers. Because maternal education is known to predict children’s vocabulary abilities (Hoff, 2003), we considered this difference when analyzing the word learning scores.
Word Learning Stimuli
The stimuli and experimental protocol followed Horst and Samuelson (2008) and Booth et al. (2008). There were 16 novel objects (Figure 1); eight were targets and eight were foils. Half of the novel objects (both targets and foils) had an extension object that differed in size and the other half had an extension object that differed in color. For the size extensions, half were smaller than the target/foil and half were larger. Prior to testing, parents saw photographs of the novel objects. If the parent indicated that the child would know the name of one of the novel objects, we replaced that object and its extension with back-up objects. In addition, familiar objects were used in warm-up trials and in one control trial. The familiar object in the warm-up included small books, cups, and cookies. The familiar objects in the control trial were small plastic dogs.
Figure 1.

Novel target objects, foils, and extensions.
The novel words followed the phonological constraints of English. They consisted of consonant-vowel-consonant-vowel combinations and including the following tokens: kaetah, foluh, dihbo, modi, haekay, poboo, gahmay, and nehpay. Each novel word was randomly assigned to its target referent. The order in which word-referent targets were trained was varied randomly across participants.
Procedure
The word learning experiment spanned two visits, lasting approximately one hour each. For all CI participants, visits were one day apart. For hearing participants, visits were one to three days apart (m = 1.53, SD = 0.55). Because of this difference, we limited the retention analysis to those participants with a one-day retention interval (AM group n = 11; VM group n = 12). We used the full data sets for analysis of fast mapping and extension.
For all procedures, the child sat across from an experimenter at a table. All of the CI participants relied on auditory-oral communication; therefore, the experimenter used spoken English throughout the experiment. During visit 1, the procedures, in order, were warm up, training of first four words, testing of first four words, control trial, training of second four words, and testing of second four words. During visit 2, the tests for all eight words were repeated.
Warm up
For each of three warm-up trials, the experimenter placed a familiar object (cup, cookie, or book) with extension objects (a different cup, cookie, or book) and a novel object on a tray. The experimenter first asked the child to identify the familiar object (e.g., Is there a cup here?). If the child accurately identified the familiar object, the experimenter asked the child to identify extensions of the familiar object (e.g., Is there another one?). The experimenter continued asking this question until the child indicated that there were no more extension objects or she identified all of the objects on the tray. If the child could not identify the familiar object or identified objects on the tray that were not extensions of the familiar object, the experimenter corrected the child. After the child identified the familiar object and extension object, the experimenter asked the child to identify the novel object on the tray (e.g., Is there a toma?). The experimenter then asked the child to name the familiar object and then the novel object. If the child could not name the novel object, the experimenter prompted the child by producing the first two phonemes of the word (e.g., It’s a to___).
Training Set 1
The experimenter placed the target novel object and the foil novel object 60 mm apart on the table. Position of the objects on the table (i.e., whether the target was to the examiner’s left or right) was randomized across trials. The experimenter labeled the object three times by stating: “There is a [target word]. I see the [target word]. Wow, that’s a [target word]!” Within the novel word training trials, gesture cues were manipulated during labeling. For four trials, eye gaze cues accompanied labeling, in which the experimenter turned her head and looked at the target object. For the other four trials, touch + eye gaze cues accompanied labeling, in which the experimenter turned her head and touched the target object three times with her index finger (once for each label). This variation did not affect word learning in any group and therefore, was not considered further; however, it is useful to note that the training was highly didactic and that the link from word to referent was made obvious by the examiner’s gestures. This procedure was repeated for each of the four target word-referent stimuli in set 1.
Testing Set 1
After training the first four items, the examiner tested for fast mapping and extension. The testing had three to five phases, depending on the child’s performance: uncued production, cued production (not administered if the child accurately named the object), preference, comprehension, and extension (not administered if the child was not accurate on the comprehension phase). Table 3 summarizes the testing protocol.
Table 3.
Sample sequence for testing paradigm using modi as the target word.
| Task | Examiner’s statement | Child’s response |
|---|---|---|
| Uncued production | “What’s this called?” | C names object. |
| If the child does not produce a label, the experimenter provides a scaffolded cue. | ||
| Cued production |
“It’s called a “mo_. What’s this called?” |
C names object. |
| If the child does not produce an accurate labeling after cueing, the experimenter holds up the object and says, “I know, it’s a modi.” | ||
| Preference | “Which one is your favorite?” | C points to favorite |
| Comprehension | “Show me the modi.” | C points to object. |
| If the child does not accurately identify the target object, the experimenter holds up the target and says, “No, that’s not it. Here it is!” and moves on to the next trial. If the child accurately identifies the target object, the experimenter administers the extension phase. | ||
| Extension | “Is there another one?” | C points to object or indicates no. |
| If the child accurately identifies the target extension, the experimenter repeats the extension until the child indicates there are no more extensions or there are no more objects left on the tray. | ||
Uncued and Cued Production Testing
Target objects were presented in the order in which they were trained. The experimenter looked at the child, held up the target object and asked, “What is this called?” If the child correctly named the object, the experimenter said, “Yes, you’re right!” and praised the child. If the child said “I don’t know” or gave an incorrect response, the experimenter moved on to the cued production test. The experimenter said, “Let me give you a clue. It’s a mo__,” providing the first two phonemes of the novel word. If the child provided a correct response for the cued production, the experimenter said, “Yes, you’re right!” Whether or not the child required a cue to produce the word, he or she was credited with a production response. If the child was still unable to provide a response after five seconds or provided an inaccurate response, the experimenter held up the target object and said, “I know, it’s a modi!” This was done to ensure that all children had the same number of exposures to the correct object-label pairing, prior to administering the comprehension and extension tests.
Twenty percent of the children’s productions were independently transcribed by a second coder. Comparison between the primary and second coders revealed a point-by-point agreement level of 80% when agreement was defined as the number of phonemes transcribed identically divided by the total number of phonemes.
Preference Testing
In the preference phase, the experimenter presented three objects to the child on a tray. These objects consisted of a target, its foil from the training trial, and a target from another trial. The examiner asked the child, “Which one is your favorite?” If children selected two objects, the examiner asked, “Which one do you like the best?” In all cases, children eventually indicated preference for one object. The preference phase allowed us to determine if children understood what was being asked during the comprehension/extension testing, or if they were merely choosing their favorite object. Data analysis indicated that none of the children favored the target object over the other objects during testing; therefore, preference testing will not be addressed in the results section.
Comprehension and Extension Testing
In this phase, the experimenter presented six objects in random order on a tray to the child. These objects consisted of a target and its extension object, its foil from the training trial and the foil’s extension object, and another target from a different training trial and its extension object. The order and pairings of objects remained consistent across all participants. In other words, the first comprehension/extension test trial included Target Object #1 (and extension object), Unnamed Foil #1 (and extension object), and Named Foil #2 (and extension object). The unnamed foil was the distracter object during the training trial. The named foil was the target object from the second training trial.
Participants were instructed to identify Target Object #1 from the set (e.g., “Give me the modi”). If the child accurately identified the target, the experimenter then asked, “Is there another one?” The experimenter continued asking this question until the child indicated no or there were no more objects on the tray. If the child did not accurately identify the target object, the experimenter held up the target and said, “Here it is!” and moved on to the next test trial. We did not administer extension trials in situations in which the child was unable to identify the target. We judged performance on the extension task to be accurate if the child correctly identified the extension object after the comprehension task and answered “no” when the examiner asked, “Is there another one?” after that point.
This same procedure continued for the second comprehension/extension test trial, which included Target Object #3 (and extension object), Unnamed Foil #3 (and extension object), and Named Foil #4 (and extension object). In the second trial, the experimenter requested Target Object #3. The third comprehension/extension test trial included Target Object #4 (and extension object), Unnamed Foil #4 (and extension object), and Named Foil #1 (and extension object). In the third trial, the experimenter requested Target Object #4. In the fourth comprehension/extension test trial, the experimenter presented Target Object #2 (and extension object), Unnamed Foil #2 (and extension object), and Named Foil #3 (and extension object). Children had to identify and extend Target Object #2. Figure 2 summarizes the process by which objects were presented during these test trials.
Figure 2.
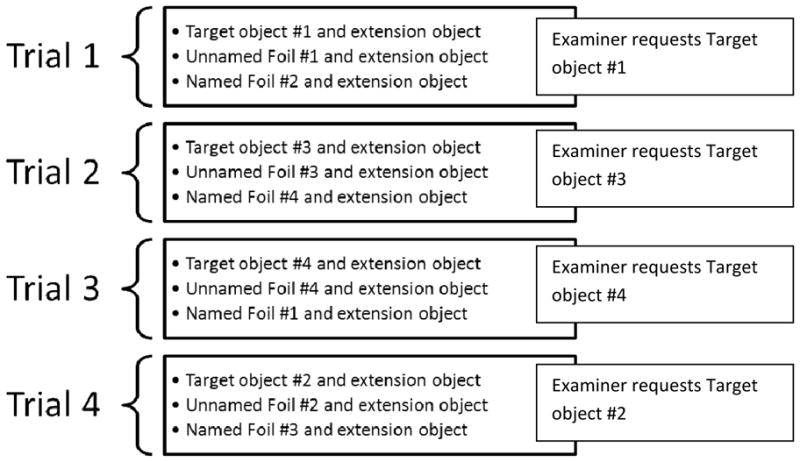
Schematic of object presentation for comprehension/extension testing, Trials 1–4.
Control Trial
After the child had completed production, preference, comprehension, and extension testing for the first four trials, the experimenter administered a control trial. In the control trial, the experimenter presented three toy dogs and four novel objects (two different objects with extension objects) on the tray. The experimenter asked the child, “Are there any dogs here? Give me a dog.” When the child indicated the dog to the experimenter, the experimenter then asked, “Is there another one?” until the child indicated no or there were no more objects on the tray. After the comprehension/extension control trial, the experimenter held up one of the dogs and asked, “What is this called?” The purpose of the control trial was to ensure that the children understood and were attending to the task.
Training and Testing Set 2
Following the control trial, the experimenter trained and tested participants on Target Objects 5 through 8. The presentation order for comprehension/extension testing was identical to Objects 1–4: Trial 1 consisted of Target Object #5, Unnamed Foil #5, and Named Foil #6; Trial 2 consisted of Target Object #7, Unnamed Foil #7, and Named Foil #8; Trial 3 consisted of consisted of Target Object #8, Unnamed Foil #8, and Named Foil #5; and Trial 4 consisted of Target Object #6, Unnamed Foil #6, and Named Foil #7.
Results
Fast Mapping
Comprehension
To determine how children performed on the comprehension task compared to chance, scores were analyzed within each group using a one-sample t-test with the test value set at chance (0.33). Recall that the participants saw six objects (the target and its extension object, the foil and its extension object, and a target from another training trial and its extension object) in the comprehension task. We scored performance as correct if the participant selected the target or its extension; therefore, chance performance was two out of six. The AM, VM, and CI groups all scored significantly higher than chance, t(23) = 9.767, p < .001; t(22) = 2.905, p = .008; t(23) = 5.457, p < .001, respectively.
Next we asked whether comprehension performance varied by group (Table 4). A Mann-Whitney U Test revealed a marginal difference between the CI and AM groups at visit 1, U = 197.5, z = −1.90, p = .057, with the AM group demonstrating higher performance. The CI and VM groups did not differ, U = 210, z = 1.43, p = .15. Years of maternal education did not correlate with performance on the comprehension task, r = .11, p = .36.
Table 4.
Descriptive statistics for comprehension, production, and extension scores (as proportion correct) by Time and Group.
| Time | Comprehension | |
|---|---|---|
| Group | Mean (SD) | |
| Visit 1 | AM (n = 24) | .68 (.18) |
| VM (n = 23) | .47 (.23) | |
| CI (n = 24) | .57 (.21) | |
| Visit 2 | AM (n = 11) | .81 (.26) |
| VM (n = 12) | .56 (.18) | |
| CI (n = 20) | .54 (.22) | |
| Weighted difference | AM (n = 10) | .28 (.93) |
| VM (n = 12) | −.01 (.69) | |
| CI (n = 20) | −.12 (.69) | |
|
| ||
| Production | ||
| Time | Group | Mean (SD) |
|
| ||
| Visit 1 | AM (n = 24) | .12 (.13) |
| VM (n = 23) | .07 (.10) | |
| CI (n = 24) | .07 (.10) | |
| Visit 2 | AM (n = 11) | .32 (.21) |
| VM (n = 12) | .11 (.10) | |
| CI (n = 20) | .06 (.09) | |
| Weighted Difference | AM (n = 11) | .17 (.28) |
| VM (n = 12) | .03 (.14) | |
| CI (n = 20) | −.01 (.09) | |
|
| ||
| Extension | ||
| Time | Group | Mean (SD) |
|
| ||
| Visit 1 | AM (n = 24) | 1.00 (0.00) |
| VM (n = 22) | 0.89 (0.30) | |
| CI (n = 24) | 0.82 (0.33) | |
| Visit 2 | AM (n = 24) | |
| VM (n = 23) | ||
| CI (n = 20) | ||
Production
Next we asked whether production performance varied by group (Table 4). A Mann-Whitney U Test revealed no difference between CI and AM groups at visit 1, U = 227, z = −1.38, p = .17 or between CI and VM groups, U = 270, z = .15, p = .88. However, it should be noted that performance in all groups approached floor. Years of maternal education did not correlate with performance on the production task, r = .15, p = .22.
Across all three groups, children relied heavily on the experimenter to provide a phonetic cue during the production task. Only two children in the AM group, one child in the CI group, and one child in the VM produced one novel label each without a phonetic cue from the experimenter.
Summary
The CI group did map new information in this highly didactic setting: they could select referents from an array of six objects when named by the examiner at a level that exceeded chance. However, their performance on this comprehension probe was marginally poorer than that of the AM group. There was no difference between the CI and AM groups in production but it should be noted that production accuracy was uniformly low and approached floor. The CI and VM groups differed on neither comprehension nor production probes.
Retention
Comprehension
Just as at fast mapping, the AM, VM, and CI groups scored significantly higher than chance on the comprehension task at visit 2, t(11) = 5.98, p < .001; t(12) = 10.78, p < .001; t(19) = 11.08, p < .001, respectively.
Next we asked whether comprehension performance varied by group (Table 4). A Mann-Whitney U Test revealed a significant difference between the CI and AM groups at visit 2, U = 39.5, z = −2.94, p = .003, with the AM group demonstrating higher performance. The CI and VM groups did not differ, U = 118, z = .08, p = .94. Years of maternal education bore a marginal positive correlation with performance on the comprehension task, r = .29, p = .07. Running an ANCOVA on the comprehension data with group (CI, AM) as the between-subjects factor, years of maternal education as the covariate, and proportion correct as the dependent variable revealed a main effect of group, F(1,27) = 5.54, p = .03, η2partial = .17 but no effect of maternal education, F(1,27) = 1.99, p = .17. Therefore, the difference between the CI and AM groups is not driven by the difference in the educational levels of their mothers.
To compare change over the retention performance between groups, we first calculated normalized difference scores via the formula (total proportion correct at visit 2 − total proportion correct at visit 1)/(1 − total proportion correct at visit 1). The normalization serves to reduce dependence upon absolute level of the score at visit 1 (Hake, 1998). All three groups made some absolute change in comprehension from visit 1 to visit 2 (Table 4), but none of these changes differed significantly from 0, CI: t = −.78, df = 19, p = .45; VM: t = −.04, df = 11, p = .97; AM: t = .95, df = 9, p = .37. Nevertheless, because the CI group demonstrated a numerical decline but the AM group demonstrated a numerical gain, a Mann-Whitney U Test revealed a significant difference between CI and AM groups in relative change over time, U = 56, z = 1.95, p = .05. There was no difference between the CI and VM groups, U = 101.5, z = .73, p = .47.
Production
Next we asked whether production performance varied by group (Table 4). A Mann-Whitney U Test revealed a significant difference between the CI and AM groups, U = 30, z = −3.48, p = .0005, with the AM group demonstrating higher performance. The CI and VM groups did not differ, U = 84, z = 1.54, p = .12. Years of maternal education did not correlate with performance on the production task, r = .20, p = .21.
Again all three groups made some absolute change from visit 1 to visit 2, but none of these changes differed significantly from 0, CI: t = −.26, df = 19, p = .80; VM: t = .15, df = 11, p = .88; AM: t = 2.00, df = 10, p = .07. Nevertheless, because again the CI group demonstrated a numerical decline but the AM group demonstrated a numerical gain, the two groups differed significantly in relative change over time, U = 51.5, z = 2.51, p = .01. The CI and VM groups did not differ, U = 107, z = .55, p = .58.
Consistent with the results of Visit 1, all children relied heavily on phonetic cues from the experimenter to name the novel objects. One child in the VM group named two novel objects without cueing, one child in the AM group named one novel object without cueing, and no children in the CI group were able to name the objects without a cue from the experimenter.
Summary
Over an interval of one day, the CI group demonstrated retention of information they had fast mapped: they continued to perform better than chance on the comprehension probe. However, their absolute performance on this comprehension probe was poorer than that of their AM peers. Also, the AM group demonstrated larger gains in comprehension over the retention interval than the CI group. Similarly, the absolute level of production and the size of the production gain score were higher for the AM than CI group. In contrast, the CI group and VM peers never differed in absolute score or gain score, whether on the comprehension or production probe.
Extension
The extension task was only given to participants who accurately identified the target object on the comprehension task. All of the children, save one (in the VM group at visit 1), accurately identified at least one target object during the comprehension trials, and therefore moved on to at least one extension trial. We calculated extension scores as a proportion of the total number of objects accurately extended divided by the total number of objects accurately identified in the comprehension test. Extensions were accurate if a participant identified the extension of the target and replied “no” when the examiner repeated the question “Is there another one?”
At visit 1, the CI group had lower extension scores than the AM group, who were at ceiling, U = 216, z = −2.58, p = .01, but they did not differ from the VM group, U = 235.5, z = −.906, p = .365 (Table 4). At visit 2, the CI group had lower extension scores than the AM group (U = 180, z = −2.56, p = 0.01). Again, the CI and VM groups did not differ (U = 202, z = −1.00, p = .31).
To better understand the extension patterns in the CI and VM groups, a summary is depicted in Figure 3. In the VM group, all of the children extended the novel label to the extension object without exception. A small subset of children (3/23) continued to select objects that were not extension objects when the examiner asked for additional objects. In other words, these three children overextended the novel object label when prompted to “find another one.” In all three cases, the VM participants were accurate at extending on the control trial with familiar objects. This indicates that they understood the directions by the examiner when they were asked to extend (or not extend) familiar items such as dog but they had difficulty defining the category boundaries of the newly learned word-referent pairs.
Figure 3.
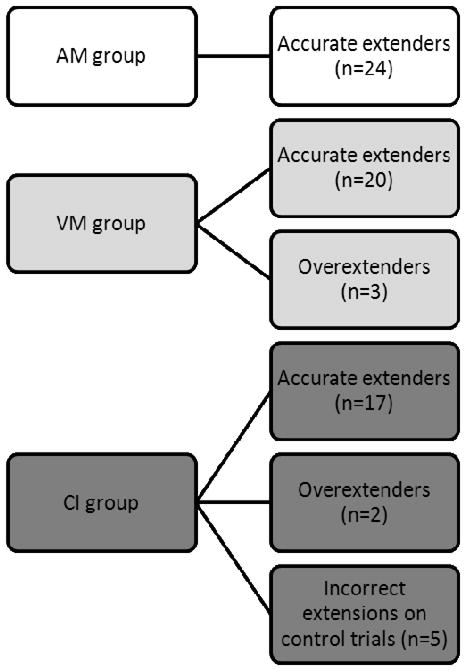
Patterns of extension for AM, VM, and CI groups.
The behaviors of the CI children were less straightforward. Seven out of 24 CI participants were inaccurate on at least one extension trial. Two of these children were accurate on the control trials, suggesting that they understood the task. Both of these children were “overextenders” like the VM children. Three other “overextenders” were incorrect on the control trials (even after training with familiar objects at the start of the experiment), suggesting that they did not understand the question put forth by the examiner. One of the CI participants (CI 032) underextended on two trials at Visit 1 (i.e., indicated that there were no extensions for the target item) and overextended for one trial. This child was incorrect on the control trial at Visit 1 and correct at Visit 2. The other CI participant (CI 016) underextended on two trials and never overextended. This child was correct on the control trial at Visit 1 and incorrect at Visit 2.
Four of the children who were inaccurate/inconsistent on control trials had PPVT-III standard scores that were at least one SD below the normative mean (range: 68–84, mean = 77). The fifth child did not complete the PPVT-III. After removing the five children from the CI group who did not understand the task, the CI and VM groups were very similar: 13% (3/23) of the VM group and 10% (2/20) of the CI group were overextenders; the others were accurate extenders. All of the children in the AM group were accurate extenders.
Individual differences
Finally we asked whether age at implantation or current vocabulary size as estimated by the PPVT-III raw score was the better predictor of overall learning performance. As a dependent variable, we summed all items correct on the comprehension and production probes at visit 2 (maximum possible score = 16; actual scores ranged from 1 – 9). When chronological age, age at implantation, and PPVT-III raw score were fed into a backward stepwise multiple regression model, only PPVT-III raw scores were significant, adjusted r2 = .35, F(1,18) = 11.21, p < .004.
Discussion
In the current study, we explored the word learning abilities of children with CIs. To do so, we exposed them to some novel word-referent pairs in a didactic setting and probed comprehension, retention, and extension behaviors immediately and following a delay. Given above-chance level performance on the comprehension probes directly after exposure and one day later, it is clear that the children with CIs fast mapped some information about the new words and retained this information as well. The majority of them also extended the newly learned words to untrained exemplars. It is important to note that the participants in this study all received their CIs at young ages and were enrolled in intensive auditory-verbal programs. Furthermore, a majority of the subjects (14 out of 24) tested within the average range on the PPVT-III. Thus, in what we might consider the “best-case scenario,” children with CIs demonstrated fast mapping, retention, and in many cases extension, of newly learned words.
Nevertheless, the children with CIs demonstrated weaker word learning than their age mates with normal hearing on a number of probes. They consistently performed like younger children who had similarly sized receptive vocabularies. Below we discuss the profile of word learning that characterized the CI group and then provide an account of the relationship between extant vocabulary size and word learning in the moment.
The word learning profile of children with CIs
Fast mapping
The children with CIs did not differ from their age mates on the immediate production probe but, in both groups, performance approached floor. Fast mapping exposures are rarely sufficient to enable production in normal-hearing children (Booth et al., 2008; Dollaghan, 1985; Gray, 2003; Gupta, 2005; Horst & Samuelson, 2008); therefore, it would be surprising if they enabled production among children with CIs.
The comprehension probe was more informative. The children with CIs performed less accurately on the immediate comprehension probe than their age mates but this difference was only marginal. Although Tomblin et al. (2007) reported a more robust difference, that study involved minimal exposure to the word and referent within a context that required inference of the word-to-referent link. In contrast, the current context was more didactic and it included three exposures to the target word forms. The extra scaffolding that this context provided likely explains the smaller effect. In fact, Lederberg and Spencer (2009) employed an inferential fast mapping condition as well as a more didactic fast mapping condition and they found that more children with CIs could fast map successfully in the didactic condition.
Extension
Extension of the newly fast mapped words to untrained exemplars was also a strength for the group of children with CIs as a whole, the majority of whom performed accurately. This tells us that these children not only map the new word to a specific referent but they also hold the useful heuristic that words apply to categories. Such a heuristic is essential for efficient word learning as it obviates the need to determine word-to-referent links each time a new referent is encountered.
Despite good performance at the group level for the children with CIs, five children failed to understand the task, and two were overextenders. No children who understood the task demonstrated underextensions. Unfortunately it is impossible to know the reason for failure to understand the task but it is worth pointing out that none of the hearing children, not even the youngest members of the VM group, had such difficulty. Furthermore, the children in the CI group who failed to understand the extension task had PPVT-III standard scores at or below 84, among the lowest vocabulary scores in the CI group. Therefore, it seems reasonable to assume that failure to understand the extension task was due to limited language skills.
The overextensions are easier to interpret. In fact, they are “developmentally appropriate” errors in that children tend to make under extensions prior to the vocabulary explosion and the onset of two-word combinations whereas overextensions persist for a developmentally longer period of time (Dromi, 2008). All of the current participants were well past the onset of two-word combinations so errors, if any, should be overextensions and they were. One of the CI children was very young (3;2) with vocabulary scores in the average range (PPVT-III standard score of 93), but a low PPVT-III raw score, commensurate with his age. The other child with a CI was older (4;5), but presented with significant delays in vocabulary (standard score of 70). That said, these two children with CIs who were overextenders had the lowest PPVT raw scores in the CI group save two other children who were among the five who failed to understand the task. This connection highlights the relationship between size of the lexicon and extension behavior that has previously been noted for normal-hearing children (Dromi, 2008).
Retention
Retention was a relative weakness for the children with CIs. After a one-day retention interval, they were significantly poorer than their age mates on both comprehension and production measures. This does not necessarily mean that they forgot the fast mapped words; in fact, their performance remained stable from visit 1 to visit 2 as evinced by normalized difference scores that did not vary from zero. However, they had begun a downward trajectory while their age mates had begun an upward trajectory. It might be telling to include a longer retention period in future studies to determine whether these trajectories continue on the same course. For now we conclude that children with CIs demonstrate consolidation characterized by stabilization over a one-day interval but the gap between them and their age mates was widening.
The role of the extant lexicon in new word learning
This study is the first to directly compare children with CIs and their vocabulary-matched peers. As predicted, these two groups had highly similar word learning outcomes whether measured as fast mapping, extension, or retention. Moreover, within the CI group, the size of the extant vocabulary as estimated by the PPVT-III, was a better predictor of word learning outcomes than age at implantation. Of course neither the CI-VM group comparisons nor the regression analysis constitute causal evidence.
Even if the relationship between extant vocabulary size and word learning in the moment is causal, the causality could be of three types. First, poor word learning in the moment could lead to a small extant vocabulary, in fact, this would seem a logical necessity as the vocabulary is the product of many instances of successful word learning over time. Second, a small extant vocabulary could lead to poor word learning. Word learning is dependent upon memory; memories are supported by activation spreading through networks of related information; and the vocabulary is such a network (McClelland & Elman, 1986). The larger and more robust that network the more easily new memories are encoded and retained. Extensive data from independent laboratories demonstrate that the ease and robustness of new word learning is influenced by established memories in the long-term lexicon (Gershkoff-Stowe & Hahn, 2007; Munro et al., 2012; Storkel, 2001; Storkel, 2009; Storkel et al., 2006). Third, and most likely in our opinion, is that the causality is reciprocal. A good word learner builds a large vocabulary which, in turn, enables additional learning. In other words, the system builds upon itself. If this is true, then the gap between good and poor word learners should widen over time, all things being equal. Of course, all things are never equal. Intervention, for one, should stave off such effects.
Although we cannot sort out the relationship between extant vocabulary size and word learning here, the very existence of the relationship may help us to understand why, in many cases, children with CIs continue to build their vocabularies more slowly than children with normal hearing even after they receive their implants (Connor et al., 2000) and why early implantation alone is not always sufficient to ensure age-level attainments (Hayes et al., 2009). Children who hear begin learning the language at birth, long before that learning is evinced as a spoken word. Moreover, they do so with the advantage of highly perceivable input. In contrast, children with CIs—even those implanted before their first birthday—experience a lag in spoken language learning and, subsequent to implantation, the disadvantage of distorted input. This situation may pose detriments to vocabulary attainment because the distortion makes for poor word learning in the moment or because the lag in exposure to spoken language makes for a small vocabulary base to build upon or because both of these factors interact reciprocally over time. The clinical implication is that vocabulary building should be an important focus of early intervention for children with CIs. Although retention was more problematic than fast mapping and extension, our data suggest that the development of all three processes was as expected given extant vocabulary size.
The role of maternal education level
There is a well-known body of literature proposing that maternal education level, as a proxy for socio-economic status, has a strong influence on word learning and vocabulary size (Hart & Risley, 1995; Hoff, 2003). Additional research in children with hearing loss indicates that maternal education significantly influences the age at which children are identified with hearing loss and fitted with hearing aids (Holte et al., in press), thus increasing the cumulative effect of socio-economic status on language outcomes. In the present study, the maternal education levels of the hearing control groups were significantly higher than the CI group. Therefore, it was important to examine the effects of this variable on performance; however, we did not find a significant correlation between years of maternal education and fast mapping (comprehension or production) or retention (production only). There was a marginally significant correlation between retention scores for comprehension and maternal education, but the subsequent ANCOVA did not demonstrate an effect of maternal education on this measure. Nevertheless, our attempt to account for maternal education is a relative strength in our research design. The only other study to compare children with CIs to children with normal hearing on a novel word learning task did not address the maternal education level of the participants (Tomblin et al., 2007). Given that most children in normal hearing control groups are recruited from university settings, maternal education levels may be skewed towards the higher end in the comparison groups, which could have a significant impact on results that compare children with CIs to children with normal hearing. Thus, future studies on word learning in children with CIs should address maternal education levels in the methods and account for this variable in statistical analyses.
The role of age at implantation
The present findings differ from previous studies (Tomblin et al., 2007; Willstedt-Svensson et al., 2004), in that we did not find a significant relationship between age at implantation and word learning. This divergence in results may be due to the ages at which the children received their CIs. In the present study, all CI children could be considered typical in terms of age at implantation – they all received CIs prior to 3 years of age, the mean age at implantation was 18 months, and 88% of the group received CIs by 2 years of age or younger. Willstedt-Svensson et al. (2004) reported on a group of CI participants who would now be considered to have a “late” age at implantation – the ages ranged from 2 years to 6 years, with a mean age of 3 years (Tomblin et al. did not report on age at implantation for their individual participants). Therefore, we may speculate that as long as children with CIs experience a short period of auditory deprivation, we may not see an influence of age at implantation on word learning performance. Further empirical study is needed to verify these findings, however.
Limitations and Future Directions
A limitation of this study is the small number of subjects within the CI group. This is a problem inherent in most CI research because it is challenging to find a sufficient number of participants who meet the inclusion criteria. We attempted to control for a number of variables by excluding children who used sign language, children with post-lingual onsets of hearing loss, and children with less than one year of CI experience. Controlling for these variables allowed us to avoid a number of confounds, but it also limited our ability to generalize these results to wider populations. Furthermore, we were limited in what we could include in an analysis of individual differences due to lack of sufficient power to examine independent variables of interest. Future directions may include a larger cohort of children, to determine the extent to which certain variables influence word learning in children with CIs. These variables may include maternal education level, age at implantation effects, and device configuration, just to name a few possibilities.
Summary
Children with CIs demonstrated deficits in word learning, with retention being especially problematic. Their learning did not differ from that of younger children who had similarly sized vocabularies. If successful word learning in the moment is predicated, in part, on an aggregation of past word learning achievements, then it becomes clear why the population of children with CIs continue to demonstrate slower vocabulary growth even after implantation.
Acknowledgments
This work was supported by a National Institutes of Health Grant NIH/NIDCD DC00242 (principal investigator Bruce J. Gantz, University of Iowa) and from the Lions Clubs International Foundation and the Iowa Lions Foundation. The second author acknowledges the support of NIH-NIDCD 1R21DC009292-01 (PI Karla K. McGregor, University of Iowa).
The authors thank Allison Bean for help with data collection. Special thanks go to the families and children who participated in the research, as well as educators at St. Joseph Institute for the Deaf in Chesterfield, MO, St. Joseph Institute for the Deaf in Indianapolis, IN, and Child’s Voice in Chicago, IL for help with recruitment.
Footnotes
This is an author-produced manuscript that has been peer reviewed and accepted for publication in the Journal of Speech, Language, and Hearing Research (JSLHR). As the “Papers in Press” version of the manuscript, it has not yet undergone copyediting, proofreading, or other quality controls associated with final published articles. As the publisher and copyright holder, the American Speech-Language-Hearing Association (ASHA) disclaims any liability resulting from use of inaccurate or misleading data or information contained herein. Further, the authors have disclosed that permission has been obtained for use of any copyrighted material and that, if applicable, conflicts of interest have been noted in the manuscript.
Portions of this article were submitted as the first author’s doctoral dissertation and presented at ASHA in New Orleans, LA on Nov 20, 2009 and the 13th Symposium on Cochlear Implants in Children in Chicago, IL on July 14, 2011.
References
- Behrend DA, Scofield J, Kleinknecht EE. Beyond fast mapping: Young children’s extensions of novel words and novel facts. Developmental Psychology. 2001;37:698–705. doi: 10.1037//0012-1649.37.5.698. [DOI] [PubMed] [Google Scholar]
- Blamey PJ, Sarant JZ, Paatsch LE, Barry JG, Bow CP, Wales RJ, Wright M, Psarros C, Rattigan K. Relationships among speech perception, production, language, hearing loss, and age in children with impaired hearing. Journal of Speech, Language, and Hearing Research. 2001;44:264–285. doi: 10.1044/1092-4388(2001/022). [DOI] [PubMed] [Google Scholar]
- Booth AE, McGregor KK, Rohlfing KJ. Socio-pragmatics and attention: contributions to gesturally guided word learning in toddlers. Language Learning and Development. 2008;4(3):179–202. [Google Scholar]
- Carey S, editor. The child as a word learner. Cambridge, MA: MIT Press; 1978. [Google Scholar]
- Carey S. Semantic development, state of the art. In: Gleitman L, Wanner E, editors. Language Acquisition, State of the Art. Cambridge: Cambridge University Press; 1982. pp. 347–389. [Google Scholar]
- Connor CM, Craig HK, Raudenbush SW, Heavner K, Zwolan TA. The age at which young children receive their cochlear implant and their vocabulary and speech-production growth: Is there an added value for early implantation? Ear and Hearing. 2006;27:628–644. doi: 10.1097/01.aud.0000240640.59205.42. [DOI] [PubMed] [Google Scholar]
- Connor CM, Hieber S, Arts H, Zwolan T. Speech, vocabulary, and the education of children using cochlear implants: Oral or total communication? Journal of Speech, Language, and Hearing Research. 2000;43:1185–1204. doi: 10.1044/jslhr.4305.1185. [DOI] [PubMed] [Google Scholar]
- Connor CM, Zwolan TA. Examining multiple sources of influence on the reading comprehension skills of children who use cochlear implants. Journal of Speech, Language, and Hearing Research. 2004;47:509–526. doi: 10.1044/1092-4388(2004/040). [DOI] [PubMed] [Google Scholar]
- Dollaghan C. Child meets word: “Fast mapping” in preschool children. Journal of Speech & Hearing Research. 1985;28:449–454. [PubMed] [Google Scholar]
- Dromi E. Old data - new eyes. Theories of word meaning acquisition. In: Gathercole VCM, editor. Routes to language: studies in honor of Melissa Bowerman. Hove, England: Psychology Press/Taylor and Francis; 2008. pp. 39–59. [Google Scholar]
- Dunn LM, Dunn LM. Peabody Picture Vocabulary Test-III. Circle Pines, MN: American Guidance Services; 1997. [Google Scholar]
- Gupta P. What’s in a word? A functional analysis of word learning. In: McGregor K, editor. Perspectives on language learning and education. Vol. 12. 2005. pp. 4–8. [Google Scholar]
- Geers AE, Moog JS, Biedenstein J, Brenner C, Hayes H. Spoken language scores of children using cochlear implants compared to hearing age-mates at school entry. Journal of Deaf Studies and Deaf Education. 2009;14:371–385. doi: 10.1093/deafed/enn046. [DOI] [PubMed] [Google Scholar]
- Gershkoff-Stowe L, Hahn ER. Fast mapping skills in the developing lexicon. Journal of Speech, Language, and Hearing Research. 2007;50:682–697. doi: 10.1044/1092-4388(2007/048). [DOI] [PubMed] [Google Scholar]
- Gray S. Word-learning by preschoolers with specific language impairment: What predicts success? Journal of Speech, Language, and Hearing Research. 2003;46:56–67. doi: 10.1044/1092-4388(2003/005). [DOI] [PubMed] [Google Scholar]
- Hake RR. Interactive engagement versus traditional methods: A six-thousand-student survey of mechanics test data for introductory physics courses. American Journal of Physics. 1998;66:64–74. [Google Scholar]
- Hart B, Risley TR. Meaningful differences in the everyday experience of young American children. Baltimore, MD: Paul H. Brookes Publishing; 1995. [Google Scholar]
- Hayes H, Geers AE, Treiman R, Moog JS. Receptive vocabulary development in deaf children with cochlear implants: Achievement in an intensive auditory-oral educational setting. Ear and Hearing. 2009;30:128–135. doi: 10.1097/AUD.0b013e3181926524. [DOI] [PubMed] [Google Scholar]
- Hirsch-Pasek K, Golinkoff RM, Hollich George. Trends and transitions in language development: Looking for the missing piece. Developmental Neuropsychology. 1999;16:139–162. [Google Scholar]
- Hoff E. The specificity of environmental influence: Socioeconomic status affects early vocabulary development via maternal speech. Child Development. 2003;74:1368–1378. doi: 10.1111/1467-8624.00612. [DOI] [PubMed] [Google Scholar]
- Holte L, Walker E, Oleson J, Spratford M, Moeller MP, Roush P, Tomblin JB, Ou H. Factors influencing follow-up to newborn hearing screening in infants who are hard-of-hearing. American Journal of Audiology. doi: 10.1044/1059-0889(2012/12-0016). (in press) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Horst JS, Samuelson LK. Fast mapping but poor retention by 24-month-old infants. Infancy. 2008;13:1288–157. doi: 10.1080/15250000701795598. [DOI] [PubMed] [Google Scholar]
- Imai M, Gentner D. A cross-linguistic study of early word meaning: Universal ontology and linguistic influence. Cognition. 1997;62:169–200. doi: 10.1016/s0010-0277(96)00784-6. [DOI] [PubMed] [Google Scholar]
- Ireton H, Thwing E. Minnesota Child Development Inventory. Minneapolis, MN: University of Minnesota; 1974. [Google Scholar]
- James D, Rajput K, Brinton J, Goswami U. Phonological awareness, vocabulary, and word reading in children who use cochlear implants: Does age of implantation explain individual variability in performance outcomes and growth? Journal of Deaf Studies and Deaf Education. 2008;13:117–137. doi: 10.1093/deafed/enm042. [DOI] [PubMed] [Google Scholar]
- Johnson C, Goswami U. Phonological awareness, vocabulary and reading in deaf children with cochlear implants. Journal of Speech, Language, and Hearing Research. 2010;53:237–261. doi: 10.1044/1092-4388(2009/08-0139). [DOI] [PubMed] [Google Scholar]
- Kaufman AS, Kaufman NL. Kaufman Brief Intelligence Test. 2. Circle Pines, MN: AGS Publishing; 2004. [Google Scholar]
- Kay-Raining Bird E, Chapman RS. Partial representations and phonological selectivity in comprehension. First Language. 1998;18:105–127. [Google Scholar]
- Kirk KI, Miyamoto RT, Ying EA, Perdew AE, Zuganelis H. Cochlear implantation in young children: Effects of age at implantation and communication mode. Volta Review. 2000;102:127–144. [Google Scholar]
- Landau B, Smith LB, Jones SS. The importance of shape in early lexical learning. Cognitive Development. 1988;3:299–321. [Google Scholar]
- Lederberg AR, Spencer PE. Word-learning abilities in deaf and hard of hearing preschoolers: Effect of lexicon size and language modality. Journal of Deaf Studies and Deaf Education. 2009;14:44–62. doi: 10.1093/deafed/enn021. [DOI] [PubMed] [Google Scholar]
- McClelland JL, Elman JL. The TRACE model of speechperception. Cognitive Psychology. 1986;18:1–86. doi: 10.1016/0010-0285(86)90015-0. [DOI] [PubMed] [Google Scholar]
- McGregor KK, Sheng L, Smith B. The precocious two-year-old: Status of the lexicon and links to the grammar. Journal of Child Language. 2005;32:563–585. doi: 10.1017/s0305000905006926. [DOI] [PubMed] [Google Scholar]
- Mervis CB, Bertrand J. Acquisition of the novel name^nameless category (N3C) principle. Child Development. 1994;65:1646–1662. doi: 10.1111/j.1467-8624.1994.tb00840.x. [DOI] [PubMed] [Google Scholar]
- Munro N, Baker E, McGregor KK, Docking K, Arculi J. Why word learning is not fast. Frontiers in Developmental Psychology. 2012;3:41. doi: 10.3389/fpsyg.2012.00041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Institute of Child Health and Human Development. NIH Publication No 00 4769. Washington, DC: U.S. Government Printing Office; 2000. Report of the National Reading Panel. Teaching children to read: An evidence-based assessment of the scientific research literature on reading and its implications for reading instruction. [Google Scholar]
- Rayner K, Foorman BR, Perfetti CA, Pesetsky D, Seidenberg MS. How psychological science informs the teaching of reading. Psychological Science in the Public Interest. 2001;2:31–74. doi: 10.1111/1529-1006.00004.. [DOI] [PubMed] [Google Scholar]
- Samuelson LK, Smith LB. Early noun vocabularies: Do oncology, category structure and syntax correspond? Cognition. 1999;73:1–33. doi: 10.1016/s0010-0277(99)00034-7. [DOI] [PubMed] [Google Scholar]
- Samuelson LK, Smith LB. They call it like they see it: Spontaneous naming and attention to shape. Developmental Science. 2005;9:182–198. doi: 10.1111/j.1467-7687.2005.00405.x. [DOI] [PubMed] [Google Scholar]
- Storkel HL. Developmental differences in the effects of phonological, lexical and semantic variables on word learning by infants. Journal of Child Language. 2009;36:291–321. doi: 10.1017/S030500090800891X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Storkel HL. Learning new words: Phonotactic probability in language development. Journal of Speech, Language, and Hearing Research. 2001;44:1321–1337. doi: 10.1044/1092-4388(2001/103). [DOI] [PubMed] [Google Scholar]
- Storkel HL, Armbrüster J, Hogan TP. Differentiating phonotactic probability and neighborhood density in adult word learning. Journal of Speech, Language, and Hearing Research. 2006;49:1175–1192. doi: 10.1044/1092-4388(2006/085). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swingley D. Fast mapping and slow mapping in children’s word learning. Language learning and Development. 2010;6:179–183. [Google Scholar]
- Tomblin JB, Barker BA, Hubbs S. Developmental constraints on language development in children with cochlear implants. International Journal of Audiology. 2007;46:512–523. doi: 10.1080/14992020701383043. [DOI] [PubMed] [Google Scholar]
- Willstedt-Svensson U, Lofqvist A, Almqvist &, Sahlen B. Is age at implant the only factor that counts? The influence of working memory on lexical and grammatical development in children with cochlear implants. International Journal of Audiology. 2004;43:506–515. doi: 10.1080/14992020400050065. [DOI] [PubMed] [Google Scholar]