

Abstract
Limb shaking Transient Ischemic Attack is a rare manifestation of carotid-occlusive disease. The symptoms usually present with seizure like activity and often misdiagnosed as focal seizures. Only on careful history the important clinical clues-which may help in differentiating from seizure-are revealed: Lack of Jacksonian march or aura; precipitation by maneuvers that lead to carotid compression. We present the case of an elderly gentleman with recurrent limb shaking transient ischemic attacks that was initially diagnosed as a case of epilepsy. His symptoms responded to optimization of blood pressure. The case report highlights the importance of accurate diagnosis as the treatment of the associated carotid artery occlusion may not only abolish the attacks but also reduce the risk of future stroke.
Keywords: Carotid occlusion, hypertension, limb-shaking transient ischemic attack, seizure mimics, stroke, transient ischemic attack
Introduction
Transient ischemic attacks (TIA) typically present with neurological deficits such as loss of muscle power, reduced sensation, or loss of vision. Symptoms such as involuntary movements are not generally regarded to be a feature of cerebral ischemic episodes. Limb shaking TIAs are a rare form of TIAs that present as involuntary movements and often confused with focal motor seizures.[1–6] This distinction, however, is crucial as this form of TIA is often an indicator of severe carotid occlusive disease and patients are at high risk of future stroke.[5–8] Moreover, such attacks may be relieved by surgical revascularization procedures in selected cases.[2,3,8] We present a case of limb shaking TIA which responded to optimization of blood pressure control and discuss the clinical manifestations, diagnosis, and management of this condition.
Case Report
In April 2009, a 71-year-old gentleman presented with a four-month history of difficulty in walking. While walking for short distances, which would vary, he used to develop involuntary jerky movements in his right leg. Occasionally, the movement also spread to his right hand. He had to clutch nearby objects to prevent the fall. These episodes occurred invariably during walking but never at rest or simply standing. The episodes would last for 1-2 minutes and were relieved by rest – either by sitting or lying down. During his visit he was having 3-4 episodes per day with significant disability. Additionally, he also had two episodes of transient right hemiparesis lasting for 20 minutes with spontaneous improvement. His medical history revealed relatively well controlled diabetes and hypertension for last 20 years and he was a chronic smoker (Two packs per day for last 30 years).
On examination his pulses were regular with blood pressure of 120/70 mm Hg without any orthostatic hypotension. The carotid pulses were feeble bilaterally without any bruit and he had subtle right hemiparesis. Walking for a short distance, he developed sudden tremulousness of the right leg with a tendency to fall towards his right. The rest of his examination was normal.
Interictal electroencephalogram (EEG) was normal. Magnetic resonance imaging (MRI) of brain revealed sub-acute infarcts in left periventricular region and centrum semiovale. MR angiography showed bilateral proximal internal carotid artery (ICA, 80-90%) and bilateral vertebral artery stenosis [Figure 1]. The rest of the investigations, including echocardiogram were normal. These features suggested a diagnosis of “Limb-shaking transient ischemic attack (TIA)” or low flow TIA.
Figure 1.
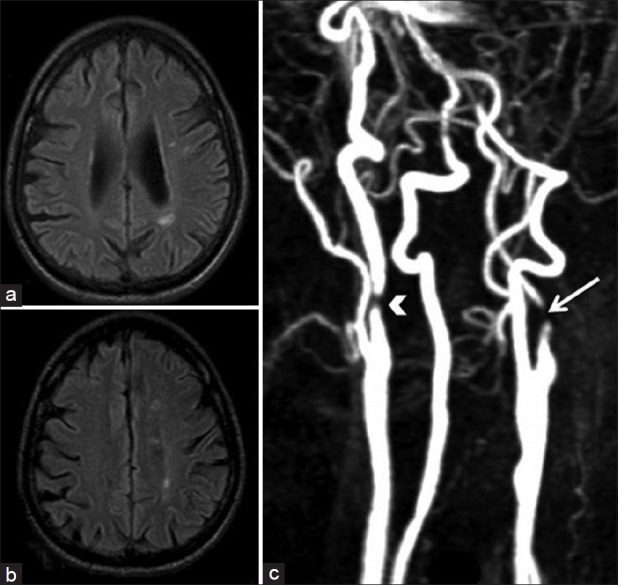
(a-b) MRI Brain (Axial section FLAIR sequence) showing infarcts in left periventricular region and centrum semiovale, (c) contrast MR angiography showing bilateral proximal internal carotid artery stenosis [(R) ICA – arrowhead, (L) ICA – arrow]
The patient refused to undergo cerebral angiography and further intervention due to personal reservations about the risk of procedures. He was treated conservatively with anti-platelet and lipid-lowering medications. In view of possible low flow state, his antihypertensive medications were withdrawn. He had significant reduction in the severity and frequency of attacks at resting blood pressure of 130-140/80-90 mm Hg.
Discussion
Recurrent, transient attacks of repetitive limb shaking are uncommon manifestations of cerebrovascular disease first described by Miller-Fisher in1962.[1] These are characterized by brief, arrhythmic, flailing or jerking movements of the leg or arm, and often misdiagnosed as focal seizures or movement disorder. As TIAs are traditionally believed to be associated with negative neurological symptoms, a diagnosis of TIA is usually not considered in a patient presenting with episodic abnormal movements. However, there are important clinical clues which help in differentiating these episodes from the seizure: absence of loss of consciousness; lack of aura; absence of incontinence; absence of tongue bite or a Jacksonian march. EEG is always normal and anticonvulsants are ineffective.[2,3] The most important clinical clue is the precipitation of symptoms by maneuvers causing cerebral hypoperfusion; such as arising from a bed or a chair, hyperextending the neck or hyperventilation; and cessation after sitting or lying down. These features also help to differentiate it from various hyperkinetic movement disorders such as hemichorea-hemiballism, hemidystonia and focal myoclonus that may occur in association with ischemic vascular disease.[4]
Limb shaking TIAs are associated with severe unilateral, and, more often, bilateral occlusive internal carotid artery disease resulting in low cerebral perfusion and ischemia-especially in the border zone areas of vascular territories. With activities that precipitate further “hypoperfusion” the reversible neurodeficit develops.[1,2,5]
The management involves improving cerebral blood flow by careful control of blood pressure and/or surgical revascularization.[1,3,4] In several cases an improvement of symptoms has been reported after raising blood pressure only, like in our case.[5]
It is worthwhile to recognize this classical but rare neurological symptom and differentiate it from conditions like focal seizures or ischemic movement disorders. A simple question about the precipitating factors may help in its recognition. Importantly, the timely treatment of the associated carotid artery occlusion may not only abolish the attacks in the patients but also reduce their risk of future stroke.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Fisher CM. Concerning recurrent transient cerebral ischemic attacks. Can Med. 1962;86:1091–19. [PMC free article] [PubMed] [Google Scholar]
- 2.Yanagihara T, Piepgras DG, Klass DW. Repetitive involuntary movements associated with episodic cerebral ischemia. Ann Neurol. 1985;18:244–250. doi: 10.1002/ana.410180212. [DOI] [PubMed] [Google Scholar]
- 3.Baquis GD, Pessin MS, Scott RM. Limb shaking-a carotid TIA. Stroke. 1985;16:444–8. doi: 10.1161/01.str.16.3.444. [DOI] [PubMed] [Google Scholar]
- 4.Salah Uddin AB. Limb shaking transient ischemic attack-an unusual presentation of carotid occlusive disease. A case report and review of the literature. Parkinsonism Relat Disord. 2004;10:451–3. doi: 10.1016/j.parkreldis.2004.04.006. [DOI] [PubMed] [Google Scholar]
- 5.Ali S, Khan MA, Khealani B. Limb-shaking Transient Ischemic Attacks: Case report and review of literature. BMC Neurol. 2006;6:5. doi: 10.1186/1471-2377-6-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Niehaus L, Neuhauser H, Meyer BU. TIAs of hemodynamic origin mimicking simple partial motor seizures. Nervenarzt. 1998;69:901–4. doi: 10.1007/s001150050361. [DOI] [PubMed] [Google Scholar]
- 7.Klijn CJ, Kappelle LJ, van Huffelen AC, Visser GH, Algra A, Tulleken CA, et al. Recurrent ischemia in symptomatic carotid occlusion. Prognostic value of hemodynamic factors. Neurology. 2000;55:1806–1812. doi: 10.1212/wnl.55.12.1806. [DOI] [PubMed] [Google Scholar]
- 8.Firlik AD, Firlik KS, Yonas H. Physiological diagnosis and surgical treatment of recurrent limb shaking: Case report. Neurosurgery. 1996;39:607–11. doi: 10.1097/00006123-199609000-00037. [DOI] [PubMed] [Google Scholar]