

Abstract
Suicide is a major public health problem in the United States as well as around the world. The significant role that alcohol plays in suicidality is well known and accepted in the scientific community. The use of alcohol does not necessarily lead to suicide, but through its action and effects, alcohol is an important proximal risk factor for suicidal behavior. There is very little data showing how and why alcohol exerts such tremendous influence and “lubricates the gears” to propel the act of committing suicide. This article will elucidate the complex relationship between alcohol and suicide and how alcohol use can lead to suicide. The article also describes how alcohol affects brain neurophysiology in regards to suicidal behavior.
Keywords: Alcohol, suicidality, lubricant, neurotransmitters, blood alcohol level, anxiolytic, lethality, alcohol influence, chemicals, social factor, cerebral cortex, limbic system, neurotransmitters
INTRODUCTION
Suicide is one of the leading causes of injury and death worldwide.1,2 Suicide is ranked 10th among all causes of death in the United States.3 An estimated 11 nonfatal suicide attempts occur per every suicide death. Risk factors for suicidality include mental disorders (e.g., depression, bipolar disorder, alcohol and other substance abuse disorders). Other risk factors are environmental (e.g., marital separation or divorce, job or financial loss), social/cultural risk factors (e.g., lack of social support, sense of isolation), prior suicide attempt, incarceration, family history of mental disorder, family history of substance abuse, and major medical illnesses (e.g., cancer).4,5
Alcohol use may not lead to suicide, but the action and effects of alcohol abuse can “lubricate the gears” for suicidal behavior. In an earlier study, Kokkevi et al6 demonstrated that a suicide attempt approximately doubled for every additional substance used. The quality of alcohol is also important. In a recent Russian study, Razvodovsky7 demonstrated that vodka consumption was significantly associated with suicide rate for both men and women; however, the consumption of beer and wine was not associated with suicide rate.
Alcohol abuse is linked to impulsivity, aggression, disinhibition of social norms, poor judgment, abnormal speech, blunting of the senses, and increased pain threshold. If a person has other risk factors for suicide, the above-mentioned behaviors facilitate the process of suicidality. Alcohol use disorders (AUDs) frequently affect the course of mental illness, such as depression, anxiety, schizophrenia, bipolar disorder, dementia, sleep disorders, and personality disorder, especially cluster B personality disorders.8 The addition of new mental illness and/or worsening of mental illness is an important contributor in precipitating suicidality. Alcohol can cause and exacerbate symptoms of mental disorders.9
Alcohol dependence often increases an individual’s vulnerability to environmental and sociocultural risk factors.5,10 For example, in many instances, alcohol is a cause of social decline, break-up of a marriage, or loss of job and family ties.11 The resulting social isolation is a potent cause of suicidality. In addition, alcohol dependence leads to loss of self-esteem and subsequently to depression; these psychological changes may predispose an individual to suicide.11 Overall, alcohol abets the entire process of suicide. In this article, the authors demonstrate how alcohol facilitates the mechanism for suicidality.
METHODS
A variety of tools was used to compile available literature to form the basis for this review article. Articles were searched by use of the following key words: alcohol, suicidality, lubricant, neurotransmitters, blood alcohol level, anxiolytic, lethality, alcohol influence, chemicals, social factor, cerebral cortex, limbic system, and neurotransmitters. More than 300 articles from 1960 to 2012 were reviewed. Finally, 82 articles were selected for this review. Selected articles mainly include retrospective human as well as animal studies and review articles on alcoholism, suicidality, and neurophysiology for either one. Statistical data from the Centers for Disease Control and Prevention (CDC) and National Institute of Mental Health (NIMH) for alcoholism and suicidality were also included. No specific exclusion criteria were applied, but articles were selected if some correlation between suicidality and alcoholism or neurophysiology of alcoholism and/or suicidality was explained in the article.
DISCUSSION
Alcohol and its association with suicidality. It is generally well known in the scientific community that alcohol plays significant role in suicidality. Alcohol is at the top of the list among drug-related suicide attempts that present at the emergency department (Figure 1).12 Persons with alcohol dependence are at a markedly elevated risk for suicide.13 The following information illustrates associations between alcohol and suicidality: 96 percent of alcoholics who die by suicide continue their substance abuse up to the end of their lives; alcoholism is a factor in approximately 30 percent of all completed suicides; approximately seven percent of those with alcohol dependence will die by suicide.14
Figure 1.

Selected substances involved in emergency department visits for drug-related suicide attempts by young adults, by sex: 2008. Source: SAMHSA
Recently, McLean et al15 demonstrated in a study on patients with schizophrenia that there is a significant association between lifetime alcohol abuse/dependence and suicide attempts (odds ratio [OR]=1.66; 95% confidence interval [CI], 1.23–2.24; P=0.001).Lejoyeux et al16 conducted a study on 180 patients who were examined in an emergency department after a suicide attempt and compared them with 180 control subjects paired for gender and age. All patients answered the CAGE Questionnaire76 and the Fagerstrom Questionnaire.77 This study concluded that 43 percent of the patients examined after a suicide attempt presented with AUD. They had taken alcohol before committing suicide more often (61% vs. 23%) and had more previous suicide attempts.16 Branas et al17 conducted a case-control study on 149 intentionally self-inflicted gun injury cases (including completed suicides by gunshot) and 302 population-based control subjects in a major United States city. This study demonstrated that acute alcohol consumption (especially to excess) is associated with higher suicide risk by gunshot.17
Similarly, retrospective studies of suicides consistently found that a high proportion were committed by alcoholics (varying from 15% in Southern England in 197418 to 27% in Seattle in 196019]. One-third of those who died by suicide were positive for alcohol use at the time of death.20 A sizeable proportion of male and female suicide decedents were legally intoxicated at the time of death.13 The evidence of these retrospective studies shows that suicide usually occurs at a late stage of alcoholism. Ilgen et al21 noted that among those with an AUD, a greater severity of recent drinking is associated with the greater likelihood of suicide attempt and suicide mortality.
Although the origins of the close relationship between alcoholism and suicide have rarely been investigated, the relationship is readily comprehended. This prompts the question: Is alcohol consumption really a lubricant to suicidality? The fact that countries that were former members of the Soviet Union have high rates of suicide and alcoholism supports the possibility that alcohol is the lubricant to suicidality.22 This lends credence to the possibility that suicidality needs a lubricant to occur. Such a lubricant could be alcohol or any other mood-altering substance. Given the effects of alcohol on the individual, alcohol may facilitate the temporary avoidance of reality, as well as numb the user to the consequences and rationale behind suicidal thoughts, ideation, and behavior. Furthermore, the low suicide rate in Islamic countries, where access to alcohol is limited, contrasted with high suicide rates in Western countries, where alcohol use is common,79 also suggests a connection between alcohol use and suicidality. This does not advocate for repression but rather publicizes the statistical association of suicide with alcohol.
If alcohol and drugs are closely related to suicidal behavior, we cannot conclude that all users are at risk. Although a consistent association exists between alcohol and suicidality, the vast majority of those with alcohol-related problems will not die by suicide. Therefore, it is important to identify those individuals with substance use disorders who might be at particularly high risk for suicide.21 Those with co-occurring psychiatric disease are in danger. The underlying psychological stressors are the main issue promoting suicidality and alcohol abuse. Public education regarding the relation between alcohol consumption and suicidality may also help to reduce suicidality among individuals with alcohol misuse.10
Substance abuse also increases lethality in the suicide attempter. A recent bivariate analysis showed that suicide attempters with substance abuse disorders had higher levels of lethality than did attempters without substance abuse.23 Suicide completers tended to be positive for high blood alcohol, and the authors concluded that intoxicated individuals are more likely to attempt suicide through the use of more lethal methods.24
Because of the prevalence of high blood alcohol levels (BAL) in individuals who commit suicide,24 all individuals with AUDs should be assessed for suicide. Such assessments are especially important at the end of a binge or in the very early phase of withdrawal.24,25 Moreover, in a retrospective survey, Hayward et al25 found that among 515 consecutive suicide victims in Western Australia, 35.8 percent had some alcohol in their blood and 24.5 percent had BAL of greater than 0.05 percent.25 Similarly, Kraft and Babigian26 also found 25 percent of suicide victims from Monroe County, New York, had BAL of 0.05 percent or greater.26 Therefore, we posit that individuals with BAL 0.05 percent or greater fall under the high-risk category for suicidality and that individuals with BAL 0.05 percent or greater require more attention during suicide assessment.
Alcohol’s impact on the brain. Alcohol (ethanol), when consumed, is absorbed through the stomach into the blood stream and then goes to the brain. Alcohol easily dissolves in fat. This property makes it easy for alcohol to go into cell membranes and bind to neural receptors. Alcohol acts not only on a single neurotransmitter but on multiple receptors.27 This disrupts and changes the receptor and neurotransmitter functions. The end result is the observed abnormalities in intoxication and the physiologic effects of alcohol. These physiologic effects are dependent on the amount consumed and the percentage concentration of alcohol.
The ventral striatum, particularly the nucleus accumbens, is critical in the reward system of the brain, and lesions in this brain region decrease the rewarding effects of many drugs of abuse. The main neurotransmitter involved in the reward pathway is dopamine. Alcohol stimulates the dopamine pathway—reward pathway. When a person drinks alcohol, within seconds it goes directly to the brain’s reward pathway (Figure 2). Dopamine gives pleasurable feelings. Instead of a small surge of pleasure, it stimulates the release of excessively high levels of neurotransmitters, which result in an immediate surge of extremely intense pleasure. It is important to note that lower doses of alcohol may cause a person to feel good, to feel free from fear, and to feel confident, whereas in higher doses, alcohol causes feelings of hopelessness and depression.28 The amount of dopamine released by alcohol can be several times higher than the amount released by natural means; this is what is commonly called the “high.”29,30 Alcohol diminishes inhibitory control of the prefrontal cortex and increases the pain threshold; this may cause uncontrolled high-risk behavior in certain individuals under the influence of alcohol.31
Figure 2.
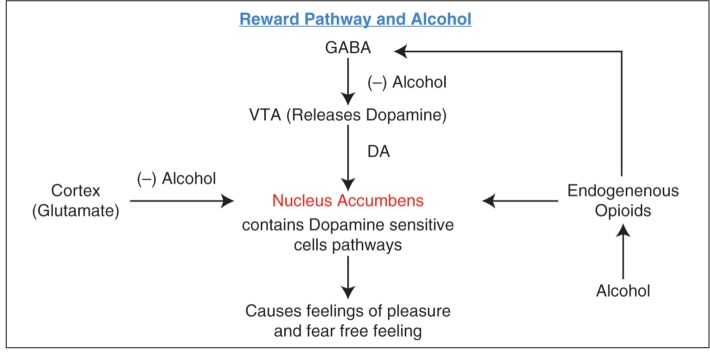
Reward pathway for alcohol
Alcohol exerts a global effect on the brain and causes negative effects on the limbic system, cerebral cortex, cerebellum, hypothalamus, pituitary glands, and brainstem.32–36 The effect of alcohol, particularly on the limbic structures (amygdala, hippocampus and parahippocampal gyrus, cingulate cortex, orbit frontal cortex, and insular cortex) is important in suicidality (Figures 3 and 4). Limbic regions tend to have a more primitive structure than the neocortex and are highly interconnected with the basal forebrain and hypothalamus.32 The limbic system is generally responsible for emotions, mood, motivation, pleasure, pain, and hormonal secretion. As alcohol affects limbic system, the person may be subject to exaggerated states of emotion: anger, aggressiveness, isolation, and memory loss. The orbitofrontal cortex is extremely well-developed in humans and is critical to judgment, insight, motivation, and mood. It is also important for conditioned emotional reactions.
Figure 3.

Connections of the amygdala. B = brain stem; T = thalamus; S = septal nuclei; Hip = hippocampus; PHG = parahippocampal gyrus; H = hypothalamus; OF = orbital frontal cortex; CG = cingulate gyrus.
Source: Swenson, Chapter 9: Limbic System
Figure 4.

Alcohol, brain areas, and suicidality
The prefrontal cortex receives input from the other areas of the limbic cortex, from the septal nuclei, and from the dorsomedial nucleus of the thalamus, and has reciprocal connections with each of these areas.37 Alcohol can damage the prefrontal cortex, where thinking, perception, and language are controlled.38 Alcohol can depress behavioral inhibition, which may cause the person to be more talkative, confident, and less socially inhibited;39 this effect is the anxiolytic effect. Alcohol can blunt the senses and increases the threshold for pain, limiting the perception of injury.40
The amygdala is a critical center for coordinating behavioral, autonomic, and endocrine responses to environmental stimuli, especially those with emotional content, such as stress and anxiety. This coordination is required for an individual to survive. Lesions of the amygdala reduce responses to stress, particularly conditioned emotional responses, such as anxiety and happiness.37 Alcohol significantly reduces the amygdala’s reactivity to threat signals, and, by this mechanism, alcohol produces its anxiolytic effect.33
Alcohol also modulates emotional processing in limbic and visual regions by decreasing the difference in activation between threatening and nonthreatening stimuli, which may contribute to both the anxiolytic properties of alcohol and to risky decision-making during intoxication.41 The hypothalamus and pituitary glands represent a part of the limbic system that control and influence many autonomic and (hormonal) endocrine functions of the brain through actions on the medulla.
According to Sher,34 alterations in the mechanisms that regulate hypothalamic-pituitary-adrenal (HPA) axis activity predate the development of AUDs. Human and animal studies indicate that chronic alcohol consumption induces a persistent impairment in the ability of the HPA axis to respond to stress. Therefore, HPA axis abnormalities may contribute to the development of AUDs and may be a result of alcohol misuse. The HPA axis interacts with serotonergic mechanisms. Hippocampal function is modulated by serotonergic projections, mostly from the dorsal raphe nucleus in the midbrain.34
Sher34 also reports an association between suicidality and hyperactivity of the HPA axis. An abnormal interaction between the HPA mechanisms and serotonergic systems may substantially contribute to suicidality in adolescents because abnormalities in HPA and serotonin functions may be inherited and may manifest at a young age. Vulnerability to AUDs and suicide probably is due to multiple interacting genetic loci of small to modest effects. The identification and treatment of adolescents at risk for suicidality is one of the most critical issues in adolescent psychiatry. The identification of alcohol and drug misuse is critical to the proper assessment of suicide risk in adolescents. HPA deregulation may contribute to both alcohol abuse and suicidality in adolescents.34
Figure 5 describes different mechanisms for hippocampus damage by alcohol. The fatty acid ethyl esters (FAEs) produced in the brain from ethanol are especially damaging to the hippocampus. When alcohol is degraded, FAEs are produced in the brain. The FAEs cause damage to the hippocampus by activating delay rectifier K+ channels in intact hippocampal cells.42 Adult neurogenesis within the hippocampus is selectively impaired in alcoholism. This may be the mechanism mediating cognitive deficits, and it may be due to oxidative stress caused by alcohol.43 Ethanol can increase release of arachidonic acid from cell membranes, and, with increased cyclooxygenase activity, can further cause oxidative stress in the brain. Hydroxyethyl free radicals derived directly from ethanol are nearly as damaging (to the hippocampus) as hydroxyl radicals and are more long-lived.44 Moreover, there is an increased deposition of lipofuscin in the neurons of chronic alcohol users. Lipofuscin is the product of the oxidation of unsaturated fatty acids and may be symptomatic of membrane damage or damage to mitochondria and lysosomes.45 Previous studies found that hippocampus in association with cortex has very important role in stress response, decision making and self-destructive behavior.
Figure 5.

Alcohol, hippocampus damage, increased self-destructive behavior, and suicidality
The cerebellum controls fine movements, muscle tone, balance, and equilibrium. As alcohol affects the cerebellum, the individual becomes uncoordinated and loses balance. Another mechanism for the motor incoordination is due to alcohol-induced potentiation of gamma-amino butyric acid (GABA)-A-associated adenosine A2A receptors in the striatum (caudate nucleus and putamen).35 Incoordination and loss of balance may be appending physical factors that might be a cause for accidental death in persons with temporary suicidal ideation caused by the high impulsive drive. Alcohol depresses the reticular activating system (RAS), which controls judgment, reflection, observation, attention, impulses, restraint, and thought processes, and may cause suicidality.36
Proposed mechanisms. The relationship between alcohol abuse and suicidality is complex. Several different possible relationships exist between alcohol abuse and suicidality. Alcohol by itself might not affect suicidality, but it may be the lubricant in the presence of other factors that lead to suicidality; or, alcohol abuse and suicidality may each be affected by some third factor without them being directly affected by each other (e.g., alcohol dependence and suicidality may be manifestations of the same underlying disorder, such as depression).10 The relationship between alcohol abuse and suicidality can be conceptualized in two ways. It can be explained from a perspective of biochemical effects and/or psychosocial effects.
Biochemical effects. Alcohol enhances GABA receptor function46 and reversibly reduces sodium transport in neurotransmission.47 GABA is the major inhibitory neurotransmitter in the brain. It acts by increasing the inflow of chloride (Cl−) across neural membranes; this prevents the tendency of neurons to depolarize. Ethanol augments the influx of chlorine ions caused by GABA, which has much to do with the sedative, tranquilizing, and/or anesthetic properties of alcohol. This causes feelings of calmness, anxiety reduction, and sleep.48 Ethanol does not have this effect on all GABA receptors, only the GABA A-subtypes (the GABA-benzodiazepine receptors) containing subunits that can be phosphorylated with protein kinase C-an enzyme that normally provides negative feedback inhibition for receptor stimulation.
Another brain neurotransmitter receptor most strongly affected by ethanol is the NMDA (M-methyl-d-aspartate) receptor for glutamic acid (glutamate). Ethanol, especially in high doses associated with heavy drinking, is a potent inhibitor of the NMDA receptor. NMDA function in the hippocampus is associated with memory formation through a process known as LTP (long-term potentiation). Ethanol produces a dose-dependent suppression of the magnitude of LTP. In high doses, ethanol can block LTP almost entirely. LTP blockage is the likely explanation for the fact that after an evening of heavy drinking, 30 to 40 percent of men in their late teens or early twenties experience a blackout, which eliminates all or part of their memory of what occurred while drinking.49 Alcohol tolerance and dependence can be attributed to compensatory synaptic plasticity, particularly an adaptive increase in NMDA receptors. Through inhibition of the glutamate receptor, alcohol causes muscular relaxation, incoordination, slurred speech, staggering, memory disruption, and blackouts.48
When ethanol is metabolized, one of its byproducts is adenosine; adenosine acts as an inhibitory neurotransmitter.50 Alcohol increases the extracellular ADP levels in brain by reducing ADP reuptake into the cell. Increased ADP is responsible for increased locomotor activity and decreased motor coordination. This behavior may contribute to the accidental death in an individual with suicidal ideation.
Alcohol raises dopamine levels.48 In addition to previously described effects, dopamine also leads to excitement and stimulation.48 A high level of dopamine is also a contributing factor for poor impulse control and aggressive behavior.52 Alcohol also raises endorphin levels,53 which kills pain and leads to a high threshold level for pain in those who consume alcohol.48
The complex relationship between alcohol, aggression, impulsivity, and suicidality can be explained by serotonergic dysfunction.54 Alcohol use exerts substantial effects on serotonin metabolism.55–60 Lower serotonin activity is tied to increased aggression/impulsivity, which in turn is presumed to enhance the probability of suicidality. For example, high-lethality depressed suicide attempters with comorbid alcohol dependence have lower cerebrospinal fluid 5-hydroxyin -doleacetic acid (5-HIAA) levels, compared with low-lethality depressed suicide attempters with comorbid alcohol dependence.59 Reduced serotonin transporter binding in the hippocampus was found in the postmortem brain tissue of patients with alcohol dependence. Similarly, binding was reduced in the 5-HT1A receptors of alcohol consumers compared with those of subjects who did not use alcohol. Hypofrontality in the anterior medial prefrontal cortical area was found in depressed patients with co-morbid alcohol dependence compared with depressed patients without alcohol dependence.24 Furthermore, another recent postmortem study on brain tissue demonstrated that region-specific change rather than global serotonin blunting is involved in alcohol dependence and suicide.61 This study tested the abnormalities in components of the serotonin (5HT) system in the prefrontal cortex and its association with suicide in alcohol-dependent subjects. This study also suggests that symptoms are differentially influenced by prefrontal cortex serotonin receptor mRNA levels.61
Psychosocial effects. External and internal risk factors as well as external and internal protective factors for suicidality are described in Figure 6. Alcohol adds risk factors to an individual’s life, making them more prone to suicidality, while removing protective factors and thus weakening an individual’s defense against the suicidality.62,63
Figure 6.

Suicidality cross
Several elements probably contribute to suicidality. Alcohol abuse exposes the person to environmental (external) suicide risk factors, such as job or financial loss and relational (e.g., break-up of marriage) or social loss. Alcohol abuse also exposes the person to social/cultural risk factors, such as lack of social support and a sense of isolation and barriers to accessing healthcare, especially mental health treatment.4,5,64 Partner-relationship disruptions are strongly associated with suicidal behavior in individuals with alcohol dependence.10
Alcohol abuse leads to loss of self-esteem and hence to depression, and these psychological changes predispose to suicidality. Moreover, major depressive episodes and stressful life events (especially interpersonal difficulties) are conceptualized as precipitating factors for suicidality.62 Elder age and major medical conditions (e.g., cancer) are also risk factors for suicidality.4,5 These are counted as internal risk factors for suicidality. When alcohol abuse combines with these external and internal risk factors, we posit that it increases suicidality. Therefore, we believe that alcohol lubricates the gears of suicidality and reduces the friction, which is an obstacle to suicidality.
Conner et al62 demonstrated a model of suicidal behavior among subjects with alcohol dependence. According to this model, predisposing factors that are presumed to increase the risk for suicide among individuals with alcohol dependence are aggression/impulsivity, severe alcoholism, and hopelessness.62 Aggression and impulsivity are related to suicidal and self-destructive behaviors; alcohol abuse is a precipitation factor for aggression and impulsivity.63–65,78,80 Skog et al60 noted that a state of intoxication might trigger self-inflicted injuries by promoting depressive thoughts and feelings of hopelessness while simultaneously removing inhibiting barriers to self-injury. Therefore, a person under the influence of alcohol may be more prone to suicidality.
Alcohol constricts attention and inhibits effective coping strategies to avoid suicidal behavior.64 Kresnow et al67 described disinhibition, in which alcohol acts to remove psychologic and physiologic barriers, leading to self-harm. Young suicide attempters have been found to have difficulties with problem-solving style and constricted thinking.68,69 The inability to generate alternative solutions is particularly associated with suicide attempts; this and other stages of problem-solving are likely to be interfered with by alcohol.70
Despite the detrimental effects and consequences of alcohol consumption, the majority of alcohol abusers use alcohol for self-medication and as a means to escape from reality.71 Most suicidal patients describe a lack of pleasure in their life as a major reason for becoming suicidal, although a recent painful event may have a triggering effect.72 Alcohol abusers admit that they are frequently bored and turn to their substance of choice mostly to get high or to feel good rather than to relieve some specific discomfort.72
Genetic predisposition. Interestingly, alcohol misuse and suicidal behavior may have a genetic link (e.g., 5-HTTLPR) involving serotonergic dysfunction.73,74 It has been suggested that the polymorphism in intron 7 of the tryptophan hydroxylase (TPH) gene has a significant link to suicidality and alcohol.54,75
CONCLUSION
On the basis of current available literature, we conclude that alcohol reduces “barriers” for suicidality through its biochemical and psychosocial mechanisms. Alcohol by itself is not necessarily a primary cause for suicidality; however, in the presence of other risk factors (e.g., psychiatric or medical illness, financial loss, and relationship issues) alcohol acts as a lubricant to suicidality. More studies are required to confirm this finding. It is important to note that suicidality also depends on BAL. During the literature review, we noted that BAL greater than 0.05 percent is a high risk for suicidality; however, there are few data available for this finding, and there is room for further research on this subject.
Footnotes
FUNDING: There was no funding for the development and writing of this article.
FINANCIAL DISCLOSURES: The authors have no conflicts of interest relevant to the content of this article.
REFERENCES
- 1.Nock MK, Borges G, Bromet EJ, et al. Suicide and suicidal behavior. Epidemiol Rev. 2008;30:133–154. doi: 10.1093/epirev/mxn002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.National Research Council. Reducing Suicide: A National Imperative. Washington, DC: The National Academies Press; 2002. [PubMed] [Google Scholar]
- 3. [Jan 11, 2012]. URL-http://www.cdc.gov/nchs/fastats/suicide.htm Suicide and Self-Inflicted Injury.
- 4. [Jan 11, 2012]. http://www.nimh.nih.gov/health/publications/suicide-in-the-us-statistics-and-prevention/index.shtml NIMH data: Suicide in the US: Statistics and Prevention. National Institute of Mental Health (2009). NIH Publication No. 06-4594.
- 5.Risk and Protective Factors for Suicide—Suicide Prevention Resource Center. [Jan 11, 2012]. http://www.sprc.org/sites/sprc.org/files/library/srisk.pdf
- 6.Kokkevi A, Richardson C, Olszewski D, et al. Multiple substance use and self-reported suicide attempts by adolescents in 16 European countries. Eur Child Adolesc Psychiatry. doi: 10.1007/s00787-012-0276-7. 2012 Apr 26: [Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- 7.Razvodovsky YE. The effects of beverage type on suicide rate in Russia. Psychiatria Danubia. 2011;23:378–383. [PubMed] [Google Scholar]
- 8.Alcoholism and psychiatric disorders: diagnostic challenges. Alcohol Res Health. 2002;26:90–98. [Google Scholar]
- 9.Laurence M, Westreich MD. Alcohol and mental illness. Primary Psychiatry. 2005;12:41–46. [Google Scholar]
- 10.Sher L. Alcohol consumption and suicide. QJM. 2006;99:57–61. doi: 10.1093/qjmed/hci146. [DOI] [PubMed] [Google Scholar]
- 11.Kendall RE. Alcohol and suicide. Substance Alcohol Actions/Misuse. 1983;4:121–127. [PubMed] [Google Scholar]
- 12. Selected Substances Involved in Emergency Department (ED) Visits for Drug-related Suicide Attempts by Young Adults, by Gender: 2008. Source: SAMHSA. (http://www.samhsa.gov/samhsanewsletter/Volume_18_Number_4/DrugRelatedSuicide.aspx Jan 11, 2012
- 13.Kaplan MS, McFarland BH, Huguet N, et al. Acute alcohol intoxication and suicide: a gender-stratified analysis of the National Violent Death Reporting System. Injury Prevention. J Intern Soc Child Adolesc Injury Prevention. doi: 10.1136/injuryprev-2012-040317. 2012 May 24. [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. [Jan 11, 2012]. URL:http://www.afsp.org/index.cfm?fuseaction=home.viewpage&page_id=050fea9f-b064-4092-b1135c3a70de1fda American Foundation of Suicide Prevention: Facts & Figure— National Statistic: Available from.
- 15.McLean D, Gladman B, Mowry B. Significant relationship between lifetime alcohol use disorders and suicide attempts in an Australian schizophrenia sample. Aust N Z J Psychiatry. 2012;46:132–140. doi: 10.1177/0004867411433211. [DOI] [PubMed] [Google Scholar]
- 16.Lejoyeux M, Gastal D, Bergeret A, et al. Alcohol use disorders among patients examined in emergency departments after a suicide attempt. Eur Addict Res. 2012;18:26–33. doi: 10.1159/000332233. [DOI] [PubMed] [Google Scholar]
- 17.Branas CC, Richmond TS, Ten Have TR, Wiebe DJ. Acute alcohol consumption, alcohol outlets, and gun suicide. Substance Use Misuse. 2011;46:1592–1603. doi: 10.3109/10826084.2011.604371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Barraclough B, Bunch J, Nelson B, Sainsbury P. A hundred cases of suicide: clinical aspects. Br J Psychiatry. 1974;125:355–373. doi: 10.1192/bjp.125.4.355. [DOI] [PubMed] [Google Scholar]
- 19. Dorpat T, Ripley H. (1960) A study of suicide in the Seattle area Comprehens Psychiatry. 1960. 1 349 359 [DOI] [PubMed] [Google Scholar]
- 20. [Jan 11, 2012]. http://www.cdc.gov/ViolencePrevention/pdf/Suicide-DataSheet-a.pdf Suicide Facts at a glance summer 2009.
- 21.Ilgen M, Kleinberg F. The link between substance abuse, violence, and suicide. Psychiatric Times. 2011;28 [Google Scholar]
- 22.Tousignant M, Goldney RD. Suicide influences and factors. [Jan 11, 2012];Macmillan Encyclopedia of Death and Dying. 2003 http://www.deathreference.com/Sh-Sy/Suicide-Influences-and-Factors.html [Google Scholar]
- 23.McManama, O’Brien KH, Berzin SC. Examining the impact of psychiatric diagnosis and comorbidity on the medical lethality of adolescent suicide attempts. Suicide Life Threat Behav. doi: 10.1111/j.1943-278X.2012.00102.x. 2012 May 30. doi: 10.1111/j.1943-278X.2012.00102.x. [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bilban M, Skibin L. Presence of alcohol in suicide victims. Forens Sci Int. 2005;147(Suppl):S9–12. doi: 10.1016/j.forsciint.2004.09.085. [DOI] [PubMed] [Google Scholar]
- 25.Hayward L, Zubrick SR, Silburn S. Blood alcohol levels in suicide cases. J Epidemiol Comm Health. 1992;46:256–260. doi: 10.1136/jech.46.3.256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kraft DP, Babigian HM. Suicide by persons with and without psychiatric contacts. Arch Gen Psychiatry. 1976;33:209–215. doi: 10.1001/archpsyc.1976.01770020047007. [DOI] [PubMed] [Google Scholar]
- 27.Gilman JM, Ramchandani VA, Davis MB, et al. Why we like to drink: a functional magnetic resonance imaging study of the rewarding and anxiolytic effects of alcohol. J Neurosci. 2008;28:4583–4591. doi: 10.1523/JNEUROSCI.0086-08.2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Di Chiara G. Alcohol and dopamine. Alcohol Health Res World. 1997;21(2):108–114. [PMC free article] [PubMed] [Google Scholar]
- 29. [Jan 11, 2012]. http://www.alternatives-for-alcoholism.com/alcohol-addiction.html Understanding Alcohol Addiction. Available from:
- 30. [Jan 11, 2012]. URL-http://www. newscientist.com/article/dn9923-glossary-drugs-and-alcohol.html?full=true New Scientist Health section — Glossary: Drugs and Alcohol. September 2006 by New Scientist Available from.
- 31.Abernathy K, Chandler LJ, Woodward JJ. Alcohol and the prefrontal cortex. Int Rev Neurobiol. 2010;91:289–320. doi: 10.1016/S0074-7742(10)91009-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Rhawn J. Neuropsychiatry, Neuropsychology, Clinical Neuroscience. New York, NY: Academic Press; 2000. The limbic system. In: [Google Scholar]
- 33.Sripada CS, et al. Effects of alcohol on brain responses to social signals of threat in humans. Neurolmage. 2011;55:371–380. doi: 10.1016/j.neuroimage.2010.11.062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Sher L. The role of the hypothalamic-pituitary-adrenal axis dysfunction in the pathophysiology of alcohol misuse and suicidal behavior in adolescents. Int J Adolesc Med Health. 2007;19:3–9. doi: 10.1515/ijamh.2007.19.1.3. [DOI] [PubMed] [Google Scholar]
- 35.Meng ZH, Anwer J, Dar MS. The striatal adenosinergic modulation of ethanol-induced motor incoordination in rats: possible role of chloride flux. Brain Res. 1997;776:235–245. doi: 10.1016/s0006-8993(97)00935-9. [DOI] [PubMed] [Google Scholar]
- 36.Rockerbie R. Alcohol and Drug Intoxication. Victoria, BC, Canada: Trafford Publishing Service; 1999. [Google Scholar]
- 37.Swenson RS. Dartmouth Medical School. Review of Clinical and Functional Neuroscience. Chapter 9: Limbic system. [Google Scholar]
- 38.Moselhy Hf, Georgiou G, Kahn A. Frontal lobe changes in alcoholism: a review of the literature. Alcohol Alcohol. 2001;36(5):357–368. doi: 10.1093/alcalc/36.5.357. [DOI] [PubMed] [Google Scholar]
- 39.Zahr NM, Sulliva EV. Translational studies of alcoholism: bridging the gap. Alcohol Res Health. 2008;31(3):215–230. [PMC free article] [PubMed] [Google Scholar]
- 40.Wolff HG, Hardy JD, Goodell H. Studies on pain: measurement of the effect of ethyl alcohol on the pain threshold and on the “alarm” reaction. J Pharmacol Exp Ther. 1942;75:38–49. [Google Scholar]
- 41.Hufford M. Alcohol and suicidal behavior. Clin Psychol Rev. 2001;21:797–811. doi: 10.1016/s0272-7358(00)00070-2. [DOI] [PubMed] [Google Scholar]
- 42.Gubitosi-Klug RA, Gross RW. Fatty acid ethyl esters, nonoxidative metabolites of ethanol, accelerate the kinetics of activation of the human brain delayed rectifier K+ channel, Kv1.1. J Biol Chem. 1996;271:32519–32522. doi: 10.1074/jbc.271.51.32519. [DOI] [PubMed] [Google Scholar]
- 43.Herrera DG, Yague AG, SivJohnsen-Soriano S, et al. Selective impairment of hippocampal neurogenesis by chronic alcoholism: protective effects of an antioxidant. Proc Natl Acad Sci U S A. 2003;100:7919–7924. doi: 10.1073/pnas.1230907100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Sun AY, Simonyi A, Sun GY. The “French Paradox” and beyond: neuro-protective effects of polyphenols. Free Radic Biol Med. 2002;32:314–318. doi: 10.1016/s0891-5849(01)00803-6. [DOI] [PubMed] [Google Scholar]
- 45.Borges MM, Paula-Barbosa MM, Volk B. Chronic alcohol consumption induces lipofuscin deposition in the rat hippocampus. Neurobiol Aging. 1986;7:347–355. doi: 10.1016/0197-4580(86)90161-2. [DOI] [PubMed] [Google Scholar]
- 46.Valenzuela CF. Alcohol and neurotransmitter interactions. Alcohol Health & Res World. 1997;21(2):144–148. [PMC free article] [PubMed] [Google Scholar]
- 47.Isreal Y, Kalant H. Effect of ethanol on the transport of sodium in frog skin. Nature. 1963;200:476–478. doi: 10.1038/200476a0. [DOI] [PubMed] [Google Scholar]
- 48.Anderson KL. Alcohol’s Effects in the Brain. [Jan 11, 2012]. http://ezinearticles.com/?Alcohols-Effects-in-the-Brain&id=1319880
- 49.Givens B, McMahon K. Ethanol suppresses the induction of long-term potentiation in vivo. Brain Res. 1995;688:27–33. doi: 10.1016/0006-8993(95)00499-g. [DOI] [PubMed] [Google Scholar]
- 50.Dohrman DP, Diamond I, Gordon AS. The role of the neuro-modulator adenosine in alcohol’s actions. Alcohol Health Res World. 1997;21:136–143. [PMC free article] [PubMed] [Google Scholar]
- 51.Carmichael FJ, Israel Y, Crawford M, et al. Central nervous system effects of acetate: contribution to the central effects of ethanol. J Pharmacol Exp Ther. 1991;259:403–408. [PubMed] [Google Scholar]
- 52.Seo D, Patrick CJ, Kennealy PJ. Role of serotonin and dopamine system interactions in the neurobiology of impulsive aggression and its comorbidity with other clinical disorders. Aggression Violent Behav. 2008;13:383–395. doi: 10.1016/j.avb.2008.06.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Jarjour S, Bai L, Gianoulakis C. Effect of acute ethanol administration on the release of opioid peptides from the midbrain including the ventral tegmental area. Alcohol Clin Exp Res. 2009;33(6):1033–1043. doi: 10.1111/j.1530-0277.2009.00924.x. [DOI] [PubMed] [Google Scholar]
- 54.Brady J. The association between alcohol misuse and suicidal behavior. Alcohol Alcohol. 2006;41:473–447. doi: 10.1093/alcalc/agl060. [DOI] [PubMed] [Google Scholar]
- 55.Gross-Isseroff R, Biegon A. Auto radiographic analysis of [3H] Imipramine binding in the human brain postmortem: effects of age and alcohol. J Neurochem. 1988;51:528–534. doi: 10.1111/j.1471-4159.1988.tb01070.x. [DOI] [PubMed] [Google Scholar]
- 56.Chen HT, Casanova MF, Kleinman JE, et al. 3H-paroxetine binding in brains of alcoholics. Psychiatry Res. 1991;38:293–299. doi: 10.1016/0165-1781(91)90019-l. [DOI] [PubMed] [Google Scholar]
- 57.Dillon KA, Gross-Isseroff R, Israeli M, Biegon A. Auto radiographic analysis of serotonin 5-HT1A receptor binding in the human brain postmortem: effects of age and alcohol. Brain Res. 1991;554:56–64. doi: 10.1016/0006-8993(91)90171-q. [DOI] [PubMed] [Google Scholar]
- 58.Sher L, Milak MS, Parsey RV, et al. Positron emission tomography study of regional brain metabolic responses to a serotonergic challenge in major depressive disorder with and without co morbid lifetime alcohol dependence. Eur Neuropsychopharmacol. 2007;17:608–615. doi: 10.1016/j.euroneuro.2007.03.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Sher L, Stanley BH, Grunebaum MF, et al. Lower cerebrospinal fluid 5-hydroxyindolacetic levels in depressed high-lethality suicide attempters with comorbid alcoholism. Biol Psychiatry. 2005;57:136S. [Google Scholar]
- 60.Ratsma JE, Van Der Stelt O, Gunning WB. Neurochemical markers of alcoholism vulnerability in humans. Alcohol Alcohol. 2002;37:522–533. doi: 10.1093/alcalc/37.6.522. [DOI] [PubMed] [Google Scholar]
- 61.Thompson PM, Cruz DA, Olukotun DY, Delgado PL. Serotonin receptor, SERT mRNA and correlations with symptoms in males with alcohol dependence and suicide. Acta Psychiatrica Scand. doi: 10.1111/j.1600-0447.2011.01816.x. 2011 Dec 19. [DOI] [PubMed] [Google Scholar]
- 62.Conner KR, Duberstein PR. Predisposing and precipitating factors for suicide among alcoholics: empirical review and conceptual integration. Alcohol Clin Exp Res. 2004;28:6S–17S. doi: 10.1097/01.alc.0000127410.84505.2a. [DOI] [PubMed] [Google Scholar]
- 63.Mann JJ, Waternaux C, Haas GL, Malone KM. Toward a clinical model of suicidal behavior in psychiatric patients. Am J Psychiatry. 1999;156:181–189. doi: 10.1176/ajp.156.2.181. [DOI] [PubMed] [Google Scholar]
- 64.Suominen K, Isometsa E, Henriksson M, et al. Hopelessness, impulsiveness and intent among suicide attempters with major depression, alcohol dependence, or both. Acta Psychiatrica Scand. 1997;96:142–149. doi: 10.1111/j.1600-0447.1997.tb09919.x. [DOI] [PubMed] [Google Scholar]
- 65.Hufford MR. Alcohol and suicidal behavior. Clin Psychol Rev. 2001;21:797–811. doi: 10.1016/s0272-7358(00)00070-2. [DOI] [PubMed] [Google Scholar]
- 66.Skog O. Alcohol and suicide— Durkheim revisited. Acta Sociologica. 1991;34:193–206. [Google Scholar]
- 67.Kresnow M, Powell KE, Webb KB, et al. Assigning time-linked exposure status to controls in unmatched case-control studies: alcohol use and nearly lethal suicide attempts. Stat Med. 2001;20:1479–1485. doi: 10.1002/sim.684. [DOI] [PubMed] [Google Scholar]
- 68.Rotherham-Borus MJ, Trautman PD, Dopkins SC, et al. Cognitive style and pleasant activities among female adolescent suicide attempters. J Consult Clin Psychol. 1990;58:554–561. doi: 10.1037//0022-006x.58.5.554. [DOI] [PubMed] [Google Scholar]
- 69.Leenaars P, Koedam M, Wester P, et al. Assessment of side effects induced by injection of different adjuvant/antigen combinations in rabbits and mice. Lab Anim. 1998;32:387–406. doi: 10.1258/002367798780599884. [DOI] [PubMed] [Google Scholar]
- 70.Hawton K. Adolescent suicide and attempted suicide: the importance of substance abuse. Crisis. 1994;15:13–14. [PubMed] [Google Scholar]
- 71. [Jan 15, 2013]. http://www.kap.samhsa.gov/products/manuals/taps/11d.htm Department of Health and Human Services. Treatment for alcohol and other drug abuse: opportunities for coordination. Technical Assistance Publication (TAP) Series 11. Chapter 3-Causes of Addiction and Modalities for Treatment. Last update Jan 31, 2002. DHHS Publication No. (SMA) 94-2075. Printed 1994.
- 72. [Jan 11, 2012]. http://www.mentalhealthandillness.com/w16.html Reward Pathway.
- 73.Preuss UW, Koller G, Soyka M, Bondy B. Association between suicide attempts and 5-HTTLPR-S-allele in alcohol-dependent and control subjects: further evidence from a German alcohol-dependent inpatient sample. Biol Psychiatry. 2001;50:636–639. doi: 10.1016/s0006-3223(01)01196-9. [DOI] [PubMed] [Google Scholar]
- 74.Collier DA, Stober G, Li T, et al. A novel functional polymorphism within promoter of the serotonin transporter gene: possible role in susceptibility to affective disorder. Mol Psychiatry. 1996;1:453–460. [PubMed] [Google Scholar]
- 75.Nielsen DA, Virkkunen M, Lappalainen J, et al. A tryptophan hydroxylase gene marker for suicidality and alcoholism. Arch Gen Psychiatry. 1998;55:593–602. doi: 10.1001/archpsyc.55.7.593. [DOI] [PubMed] [Google Scholar]
- 76.O’Brien CP. The CAGE Questionnaire for detection of alcohol. JAMA. 2008;300(17):2054–2056. doi: 10.1001/jama.2008.570. [DOI] [PubMed] [Google Scholar]
- 77.Rustin TA. Assessing nicotine dependence. Am Fam Physician. 2000;62(3):579–584. [PubMed] [Google Scholar]
- 78.Cherpitel CJ, Borges GLG, Wilcox HC. Acute alcohol use and suicidal behavior: a review of the literature. alcoholism. Clin Exp Res. 2004;28:18S–28S. doi: 10.1097/01.alc.0000127411.61634.14. [DOI] [PubMed] [Google Scholar]
- 79.World Health Organization. [January 15, 2013]. http://www.who.int/violence_injury_prevention/violence/world_report/factsheets/pb_violencealcohol.pdf WHO policy briefing. Alcohol and violence. Interpersonal violence and alcohol.
- 80.Burge SK, Schneider FD. Alcohol-related problems: recognition and intervention. Am Fam Physician. 1999;59(2):361–370. [PubMed] [Google Scholar]