

Abstract
Background
Anatomic tunnel positioning is important in anterior cruciate ligament (ACL) reconstructive surgery. Recent studies have suggested the limitations of a traditional transtibial technique to place the ACL graft within the anatomic tunnel position of the ACL on the femur. The purpose of this study is to determine if the 2-incision tibial tunnel-independent technique can place femoral tunnel to native ACL center when compared with the transtibial technique, as the placement with the tibial tunnel-independent technique is unconstrained by tibial tunnel.
Methods
In sixty-nine patients, single-bundle ACL reconstruction with preservation of remnant bundle using hamstring tendon autograft was performed. Femoral tunnel locations were measured with quadrant methods on the medial to lateral view of the lateral femoral condyle. Tibial tunnel locations were measured in the anatomical coordinates axis on the top view of the proximal tibia. These measurements were compared with reference data on anatomical tunnel position.
Results
With the quadrant method, the femoral tunnel centers of the transtibial technique and tibial tunnel-independent technique were located. The mean (± standard deviation) was 36.49% ± 7.65% and 24.71% ± 4.90%, respectively, from the over-the-top, along the notch roof (parallel to the Blumensaat line); and at 7.71% ± 7.25% and 27.08% ± 7.05%, from the notch roof (perpendicular to the Blumensaat line). The tibial tunnel centers of the transtibial technique and tibial tunnel-independent technique were located at 39.83% ± 8.20% and 36.32% ± 8.10%, respectively, of the anterior to posterior tibial plateau depth; and at 49.13% ± 4.02% and 47.75% ± 4.04%, of the medial to lateral tibial plateau width. There was no statistical difference between the two techniques in tibial tunnel position. The tibial tunnel-independent technique used in this study placed femoral tunnel closer to the anatomical ACL anteromedial bundle center. In contrast, the transtibial technique placed the femoral tunnel more shallow and higher from the anatomical position, resulting in more vertical grafts.
Conclusions
After single-bundle ACL reconstruction, three-dimensional computed tomography showed that the tibial tunnel-independent technique allows for the placement of the graft closer to the anatomical femoral tunnel position when compared with the traditional transtibial technique.
Keywords: Anterior cruciate ligament, Three-dimensional computed tomography, Transtibial technique, 2-Incision tibial tunnel-independent technique
The transtibial technique has been wildly accepted as a gold standard in the arthroscopic anterior cruciate ligament (ACL) reconstructive surgery since its introduction. The transtibial drilling of femoral tunnels can simplify the procedure, enabling further reductions in surgical time and trauma by means of a single-incision approach. The traditional transtibial technique has been commonly used in the ACL reconstruction of the past 25 years, and its successful outcomes have been reported.1)
Despite some advantages and favorable outcomes of the transtibial technique, recent researchers have questioned whether this technique sufficiently recreates the anatomy and the function of the native ACL.2) Proper positioning of the femoral tunnel during ACL reconstruction is principal, with nonanatomic tunnel placement cited as the most common cause of clinical failure secondary to pain and persistent instability.3) Inaccurate placement of femoral tunnel is a common cause of graft failure in ACL reconstruction, with the too anteriorly positioned tunnel.4)
The limitations of linear surgical instrumentation coupled with the constraints imposed by tibial tunnel have often led to femoral tunnels that are vertical and nonanatomic in position.5) Although modifications to the conventional transtibial technique such as posterolateral beveling of the tibial tunnel and using a more collinear, proximal, and medial tibial starting point have been used to improve femoral tunnel positioning, these have been employed primarily with the 10 or 11 mm tunnels created for bone-patellar tendon-bone reconstructions.6,7)
According to the incompleteness of the widely used methodology, many researchers have searched for a better method to improve the tunnel placement after ACL reconstruction. As a result, the technique of ACL reconstruction evolved from a traditional transtibial technique to a 2-incision tibial tunnel-independent technique, using outside-in femoral tunnel drilling.8) Recently, successful results of tibial tunnel-independent technique have been studied.5) Although more anatomical placement of femoral tunnel after tibial tunnel-independent technique was reported in several cadaver studies,9,10) it is important that these results be replicated in the clinical sample, with the technique used in the actual clinical field.
We assumed that the 2-incision tibial tunnel-independent technique would allow for a more anatomic tunnel placement, as it is unconstrained by the tibial tunnel. In order to demonstrate this hypothesis, we retrospectively evaluated the three-dimensional (3D) positions of the femoral and tibial tunnels in the patients who had undergone a traditional transtibial technique and 2-incision tibial tunnel-independent technique, using 3D reconstruction computed tomography (CT). Tunnel positions of each technique were then compared with the reference data of established anatomic anteromedial and posterolateral bundle tunnel positions in the tibia and femur.
METHODS
Patient Selection and Study Design
The patients who had undergone ACL reconstruction between 2 and 8 months after unilateral ACL injury with preservation of remnant bundle using hamstring tendon autograft were included in this study. The ACL reconstruction was performed using either of the two techniques (transtibial or tibial tunnel-independent technique) by a single surgeon (JHA), from October 2010 to June 2011. We divided the patients into two groups according to the femoral tunnel placement method (transtibial vs. tibial tunnel-independent technique group). Patients operated between October 2010 and February 2011 underwent ACL reconstruction using transtibial technique. In the second group, ACL reconstruction was performed using tibia tunnel-independent technique. This group of patients operated between March and June 2011, as the senior surgeon changed his technique from March 2011. Our exclusion criteria included: 1) combined collateral or posterior cruciate ligament injuries; 2) revision ACL reconstruction; 3) double bundle ACL reconstruction; and 4) tunnel aperture could not be clearly identified in the 3D CT model. Thus, seven patients were excluded due to the exclusion criteria.
The 69 participants were mean age at 29.91 ± 9.21 years; and 54 male and 15 female. Transtibial technique was used in 34 subjects (9 female, 25 male; mean age, 30.06 ± 8.32 years; range, 15 to 44 years). Tibial tunnel-independent technique was used in 35 subjects (6 female, 29 male; mean age, 29.77 ± 10.11 years; range, 17 to 48 years). There was no statistical difference in sex distribution (χ2 = 0.882, p = 0.259) and mean age (t = 0.129, p = 0.898) between the two groups. The protocol of this retrospective, cross-sectional comparative study was approved by the Ethics Committee of the Kangbuk Samsung Hospital.
The Transtibial Technique
In the transtibial technique, a tibial tunnel made by a commercial tibial drill guide (Linvatec, Largo, FL, USA), with a 45° angle between the aiming arm and the drilling arm, placed a guide pin at the inner border of the anterior horn of the lateral meniscus, just lateral to the medial eminence and 7 mm anterior to posterior cruciate ligament in the intercondylar plateau. A cannulated reamer was used for over-reaming the guide pin. A 5.5 mm femoral tunnel offset guide was then inserted through the reamed tibial tunnel. Once the tip of the guide was hooked around the posterior wall of the intercondylar notch, the guide was maximally rotated in an attempt to place the femoral tunnel guide pin as close as possible to the anatomic location of the ACL, as judged visually by the surgeon. Femoral tunnel was made to a 30 to 35 mm depth and a 1 to 2 mm before the posterior cortex (Fig. 1).
Fig. 1.
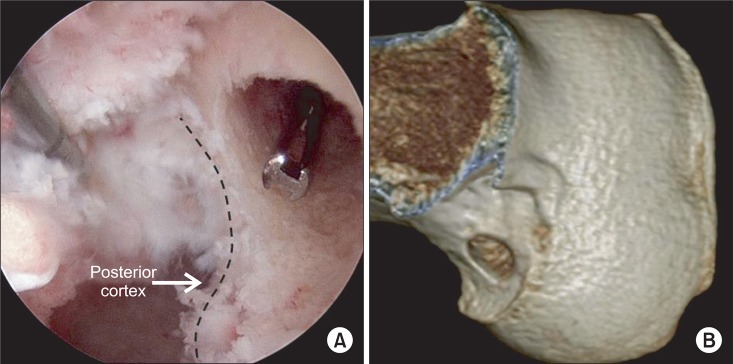
Femoral tunnel made by the transtibial technique. (A) The femoral tunnel was made 1 to 2 mm before the posterior cortex. (B) Three-dimensional computed tomography shows the femoral tunnel made by the transtibial technique.
The 2-Incision Tibial Tunnel-Independent Technique
After diagnostic arthroscopy, the femoral footprint of the torn ACL was identified. With the knee at 90° flexion, the microfracture awl was inserted through the anteromedial portal and positioned to the center of the anatomic anteromedial bundle footprint of the ACL femoral origin as closely as possible, assessed visually by surgeon. The method of positioning tibial tunnel was identical to the transtibial technique described above.
If surgeon was unable to observe ACL footprint because of the after-notchplasty or chronic ACL deficiency, the surgeon placed a marking hole using a microfracture awl at 5 to 6 mm shallow on horizontal axis (along the notch roof), from the posterior edge of the intercondylar notch (over-the-top), and then from this point, 2 to 3 mm low on vertical axis (vertical to notch roof) in anterolateral portal view. The arthroscope was moved to an anteromedial portal viewing position, the tip of ACL femoral guide (Linvatec) was placed precisely at the marking hole, and a 3.5 mm outside-in minimally invasive drilling pin (Flipcutter, Arthrex, Naples, FL, USA) was introduced through a stab incision at the distal midlateral femoral metaphyseal flare, 3 cm proximal to the lateral epicondyle, and drilled to create an outside-in femoral tunnel. The cutter chosen to match the diameter of the graft was used to cut a socket into the femur to the desired depth (Fig. 2).
Fig. 2.

Femoral tunnel made by the tibial tunnel-independent technique. (A) The marking hole was located at 5 to 6 mm shallow from the most proximal high deep point on the cartilage-bone border of lateral condyle (over-the-top), and from this point, 2 to 3 mm low. (B) Through a stab incision at the distal midlateral femoral metaphyseal flare, 3.5 mm outside-in minimally invasive drilling pin (Flipcutter) was introduced. (C) The cutter chosen to match the diameter of the graft; 10 mm drilled to create an outside-in femoral tunnel. (D) Three-dimensional computed tomography shows the femoral tunnel made by the tibial tunnel-independent technique.
3D Reconstruction of CT
Three of four days after surgery, 3D CT images of the knee in the extended position were obtained. The 3D CT images can depict the bone tunnel apertures in three dimensions from all viewpoints. The 128 channels Brilliance iCT SP and Brilliance 64-channel scanner (Philips, Amsterdam, Netherlands) were used for 3D reconstruction CT imaging. The 3D CT images were reconstructed, scanning with 0.5 mm interval and obtaining sagittal, coronal, and transverse plane view with 2 mm interval, using Extended Brilliance Workstation (EBW, Philips). For the geometric measurement, the file was converted as a form of Digital Imaging and Communication in Medicine (DICOM) and transmitted to picture archiving and communication system (PACS; PiViewSTAR 5.0, INFINITT, Seoul, Korea).
Measurements on 3D Images
Femoral tunnel position
As previously described, the rotation and positioning of the 3D femur and tibia models were performed. On radiographs, the grid is aligned with the Blumensaat line, which is a projection of the femoral notch roof on the radiograph. However, since no such line exists on a 3D CT graphy model, the most anterior edge of the femoral notch roof was chosen as the reference for the grid alignment.
Distance DS (parallel to the Blumensaat line) was defined as the total sagittal diameter of the lateral femoral condyle, measured along the intercondylar notch roof. Distance HL (perpendicular to the Blumensaat line) represented the height of the intercondylar notch, measured from the intercondylar notch roof to a line tangent to the distal subchondral bone contour of the condyle. The location of the tunnel was quantified from the center of the tunnel to the deepest subchondral bone contour (distance FA) and the intercondylar notch roof (distance FB), respectively. In the transtibial technique group, elliptical shape of tunnel showed the most; and we calculated the point where the longest diameter and the shortest diameter of ellipse met on the radiographs as the center of tunnel.
For comparing the tunnel position of each technique with anatomical ACL center position, we calculated the ACL center through the 2D mean value of anteromedial bundle center and posterolateral bundle center from Forsythe et al.11) In the femur, the Euclidean distance from the anatomical reference position to the actual postoperative positions was measured with the formula as follows: Euclidean distance = √ {(FA distance to ACL center)2 + (FB distance to ACL center)2}
Tibial tunnel position
The centers of the tibial tunnel apertures were determined with an anatomically aligned coronal plane grid, as previously described.12)
Using a top view on the tibial plateau, the tibial tunnel locations were presented in a grid aligned with the medial to lateral and anterior to posterior anatomical tibial axes. Distance anterior to posterior and distance medial to lateral represented the total depth and the total width of the proximal tibia, respectively. The tibial tunnel location was measured from the anterior border (distance TA) and medial border (distance TB) of this reference grid.
The pictures of the medial to lateral view of the lateral femoral condyle and the top view of proximal tibia were measured independently by one orthopedic surgeon, in order to evaluate the ACL tunnel position. The measurements were performed on a PACS monitor (GE Healthcare, Barrington, IL, USA), using a mouse point cursor and automated computer calculation for the distances between points and lines. All measurements were performed twice by the same investigator.
All measurements were expressed as a percentage of the corresponding maximum dimension. Tunnel locations were presented as the mean and standard deviation, with the range (minimum to maximum) in parentheses. These tunnel positions were then compared with the reference data of previous cadaver study by Forsythe et al.,11) which evaluated tunnel positions after anatomic double-bundle ACL reconstruction.
In this study, arthroscopic terminology was used to describe the position of the femoral tunnel in the notch relative to the flexed knee: shallow or deep; and high or low.13) The anatomical reference positions were calculated from the mean numerical value of anatomical position of anteromedial and posterolateral bundle of ACL in each axis (tibia: anterior to posterior and medial to lateral; and femur: parallel line and perpendicular line to Blumensaat line), as measured by Forsythe et al.11) In tibia, the Euclidean distances from the anatomical reference position to the actual postoperative coordinates were also measured as: Euclidean distance = √ {(TA distance to ACL center)2 + (TB distance to ACL center)2}.
Statistical Analysis
The demographic characteristics between two groups were compared by Fischer's exact test and independent t-test. As the continuous variables measuring the distance from anatomical center to actual postoperational tunnel position were normally distributed (by Kolmogorov-Smirnov test), the differences in distance between the two ACL reconstruction techniques and those among the other continuous variables were analyzed with an independent t-test. All the analyses were performed using PASW ver. 17.0 (SPSS Inc., Chicago, IL, USA), with the cut-off for statistical significance set at p < 0.05. The Bonferroni correction was used to correct for multiple comparisons.
RESULTS
Femoral Tunnel Positions
On the femur, the tibial tunnel-independent technique placed the femoral tunnel closer to the calculated ACL femoral center than transtibial technique (transtibial vs. tibial tunnel-independent: 38.20% ± 7.15% vs. 18.08% ± 7.38%; t = 11.493; p < 0.001). Parallel to the Blumensaat line (DS), the tunnel positions after transtibial technique were significantly more shallow than the tibial tunnel-independent technique (transtibial vs. tibial tunnel-independent: 36.49% ± 7.65% vs. 24.71% ± 4.90%; t = 7.590; p < 0.001) and distanced more apart from the calculated ACL center (transtibial vs. tibial tunnel-independent: 8.09% ± 7.65% vs. 3.61% ± 4.90%; t = 3.521; p = 0.001). Perpendicular to the Blumensaat line (HL), TTs were positioned significantly closer (higher) to the Blumensaat line compared with the tunnel positions after transtibial technique (transtibial vs. tibial tunnel-independent: 7.71% ± 7.25% vs. 27.08% ± 7.05%; t = -11.256; p < 0.001). The tunnel positions are summarized in Table 1 and displayed in Figs. 3 and 4.
Table 1.
Summary of Femoral Tunnel Positions of the TT and TI Technique
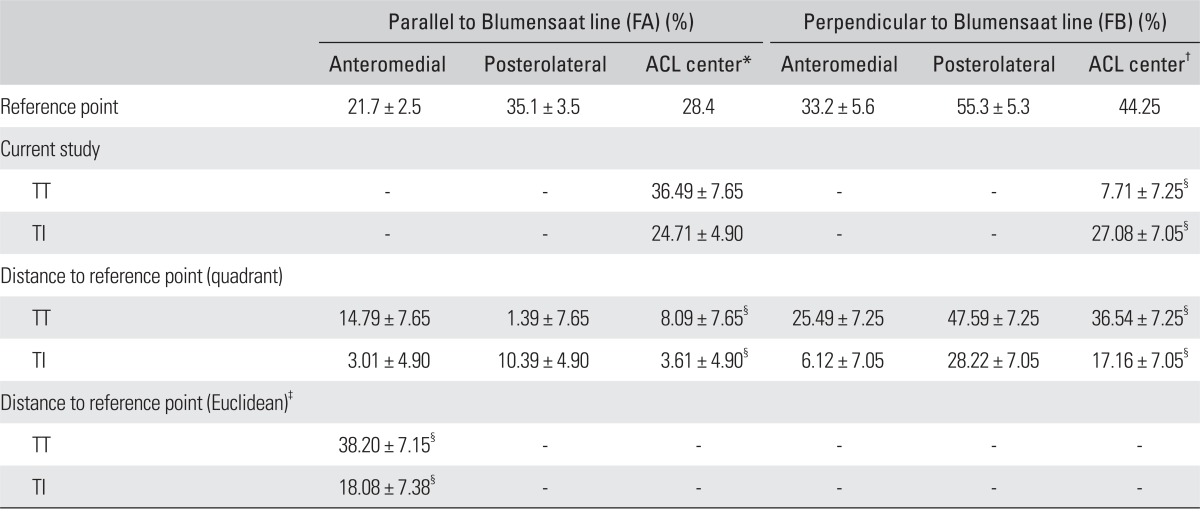
Values are presented as mean ± standard deviation.
TT: transtibial, TI: tibial tunnel-independent, FA: femur 'A' line, FB: femur 'B' line, ACL: anterior cruciate ligament.
*ACL center was calculated as a mean value of anteromedial and posterolateral bundle coordinate on the axis parallel to Blumensaat line. †ACL center was calculated as a mean value of anteromedial and posterolateral bundle coordinate on the axis perpendicular to Blumensaat line. ‡Distance to reference point (Euclidean) = √ {(FA distance to ACL center)2 + (FB distance to ACL center)2}. §The difference between transtibial and tibial tunnel-independent technique was significant (p < 0.05, independent t-test).
Fig. 3.

On the lateral femoral side of three-dimensional computed tomography, the location of the transtibial and tibial independent femoral tunnel are shown. The location of tunnel was quantified from center of the tunnel to the deepest subchondral bone contour (distance FA) and the intercondylar notch roof (distance FB). ACL: anterior cruciate ligament, AM: anteromedial, PL: posterolateral, TT: transtibial, TI: tibial tunnel-independent, DS: distance deep to shallow, HL: distance high to low, FA: femur 'A' line, FB: femur 'B' line.
Fig. 4.

4 × 4 grid of quadrant method, by tibial tunnel-independent technique: 9 (25.7%) and 14 (40.0%) of 35 femoral tunnels located in 2a and 2b grid, respectively. On the other hand, by transtibial technique, 28 (82.4%) of 34 femoral tunnels were located in 1b grid; furthermore, 3 of 34 were located over the Blumensaat line (red line).
Tibial Tunnel Positions
As expected, there was no significant difference in the Euclidean distance to calculated ACL tibial center between transtibial and tibial tunnel-independent tunnel positions on the tibia (transtibial vs. tibial tunnel-independent: 8.85% ± 5.07% vs. 8.86% ± 3.95%; t = -0.002; p = 0.999). In anterior to posterior direction, the transtibial tunnel positions were posterior to the tibial tunnel-independent technique positions, although the difference was not significant (transtibial vs. tibial tunnel-independent: 4.13% ± 8.59% vs. 0.62% ± 8.10%; t = 1.788; p = 0.078). However, in the medial to lateral direction, both positions of transtibial and tibial tunnel-independent technique were located medial to the calculated ACL center and not significantly different (transtibial vs. tibial tunnel-independent: 2.32% ± 4.02% vs. 3.70% ± 4.04%; t = 1.423; p = 0.159). The tunnel positions are summarized in Table 2 and displayed in Fig. 5.
Table 2.
Summary of Tibial Tunnel Positions of the TT and TI Technique
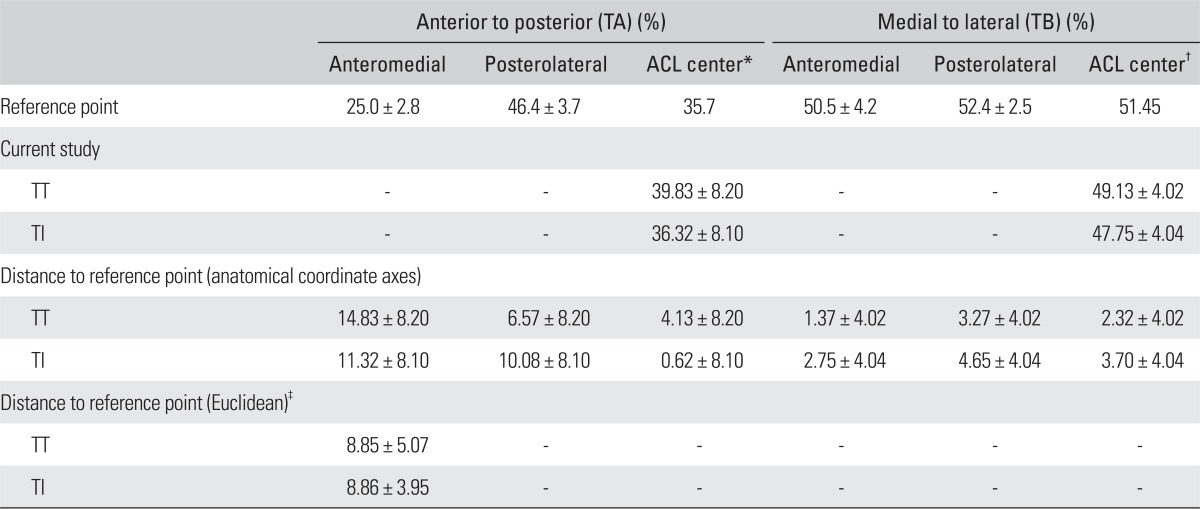
Values are presented as mean ± standard deviation.
TT: transtibial, TI: tibial tunnel-independent, TA: tibia 'A' line, TB: tibia 'B' line, ACL: anterior cruciate ligament.
*ACL center was calculated as a mean value of anteromedial and posterolateral bundle coordinate on the anterior to posterior axis. †ACL center was calculated as a mean value of anteromedial and posterolateral bundle coordinate on the medial to lateral axis. ‡Distance to reference point (Euclidean) = √ {(TA distance to ACL center)2 + (TB distance to ACL center)2}. §The difference between transtibial and tibial tunnel-independent technique was significant (p < 0.05, independent t-test).
Fig. 5.

On the top view of the proximal tibia, the location of the transtibial and tibial independent tibial tunnel are shown. The location of tunnel was measured from the anterior border (distance TA) and medial border (distance TB). AP: distance anterior to posterior, ML: distance medial to lateral, AM: anteromedial, PL: posterolateral, TT: transtibial, TI: tibial tunnel-independent, TA: tibia 'A' line, TB: tibia 'B' line.
DISCUSSION
In this study, we compared the tunnel position of the transtibial technique and the 2-incision tibial tunnel-independent technique in single-bundle ACL reconstruction using 3D CT. As expected, our results demonstrated that the conventional transtibial technique for arthroscopic ACL reconstruction placed the femoral tunnel more apart from the calculated ACL center. On the other hand, the tibial tunnel-independent technique placed the femoral tunnel closer to the calculated ACL center and in a more anatomic position. There was no significant difference in tibial tunnel placement between the two techniques.
The anatomical placement of tunnel is a major concern in the ACL reconstructive surgery.14) Our data are in agreement with the previous results that anatomic femoral placement is more difficult to achieve with the transtibial technique. The transtibial technique was thought to cause anterior (high) oriented graft with limited ability to restore the oblique orientation of the ACL and to restore normal knee stability.15) While we agree with the results which indicated the difficulty of placing anatomical femoral tunnel using the transtibial technique, several recent researchers have tried to improve the femoral tunnel position in this method. Howell and colleagues16) have recommended a method which made more horizontal tibial tunnels in the coronal plane for avoiding the tendency to place vertical grafts during transtibial drilling. However, their practice often required tunneling through the medial collateral ligament and under the medial tibial plateau. Other researchers have recommended transtibial drilling to place femoral tunnel near the center of femoral attachment of the ACL, but this method induces a posterior tibial tunnel. 17) Although transtibial technique could place the graft to a more accurate femoral and tibial position if the tibial starting point was meticulously aligned with the native ligament's axis and moved to a more proximal position, this method would require a meticulous positioning of the tibial tunnel with a little margin for error and some degree of graft-tunnel mismatch.18) Moreover, a recent study reported that the best efforts to rotate the over-the-top guide to improve guide pin positioning could not make for the resultant femoral tunnels which had a mean 30% overlap with the native femoral insertion site.19) We also found that accurate femoral placement is more difficult to achieve with the transtibial technique than tibia tunnel-independent technique. In this study, guide pins placed using the transtibial technique were shallow and high in position from the calculated ACL center. We also suppose that the limited ability of the transtibial technique to place the guide pin in the femoral footprint is likely the result of the constraints of the tibial tunnel.
Many approaches have been used to achieve more accurate tunnel placement near the center of the ACL on the femur and tibia, such anterior medial portal technique, posterior tibial tunnel method, and 2-incision tibial tunnel-independent technique.20-22) Among the techniques, 2-incision tibial tunnel-independent technique has become known to more closely center the graft, relative to the native ACL footprint.20) The result from a recent researcher showed the grafts placed with independent drilling to have better horizontal alignments compared to grafts placed with transtibial drilling.23) There are many reasons for the tibial tunnel-independent techniques in reproducing the anatomy and function of native ACL better. This technique allows for placement of the guide pin within 2 mm of the center of the ACL footprint; then the tunnel can be centered in the ACL footprint, low on the wall of the notch, without the constraint of a guide through the tibial tunnel.
The independent technique could place the guide pin near the center of the ACL footprint with a visible remnant or visible bony landmarks. It might be difficult to observe the ACL remnant in chronic ACL deficient knee, or to observe bony landmarks after notchplasty of lateral condyle. In this study, when we targeted the femoral tunnel center during the tibial tunnel-independent technique, we referenced most proximal high deep point on the cartilage-bone border of lateral condyle (over-the-top) from anteromedial viewing portal after minimal notch plasty. The femoral tunnel center was decided by the 5 to 6 mm distal (shallow) in parallel line to the intercondylar notch roof from the over-the-top; and from this point, by the 2 to 3 mm posterior (low) in perpendicular line to intercondylar notch roof. This placement was close to the anteromedial bundle, and more anterior (high) and proximal (deep) to the calculated anatomic ACL center in the postoperative 3D CT. The authors preferred to the femoral tunnel close to anteromedial bundle rather than close to native ACL femoral footprint center. However, we considered it as an optimal position which could negotiate the anatomic position of ACL and isometric position in single-bundle ACL reconstruction. Some researchers also reported that the anteromedial graft can play a role in rotatory stability in addition to the posterolateral graft.24,25) Although this targeting point leads to the more vertical ACL graft, we assumed that the independent technique had more rotational stability than the convention transtibial technique, because the independent technique placed the more oblique femoral tunnels in the lateral femoral part. Thus, the position of femoral tunnel by independent tibia-tunnel technique was quite close to the anatomic center of anteromedial bundle in this study.
Although we replicated the previous results, novelty of our study was to use 3D CT for comparing tunnel placement of two techniques. The 3D CT scans have been used to evaluate tunnel location11,26) and tunnel widening after ACL reconstruction.27) The 3D CT scans provide an excellent perspective of the tunnel aperture and bony morphology by selectively removing section of the bone from the model and rotating the model view. With the scan, the regions of the bone that are traditionally difficult to see can be clearly visualized. It is thought that preoperative 3D CT evaluation would be useful when surgeons estimate the cause of previous ACL reconstruction failure due to femoral tunnel malposition before revisional ACL reconstruction.
While some studies have recently reported the results of comparing the tunnel position of transtibial technique and tibial tunnel-independent technique with anatomic ACL center,12,18) these studies used magnetic resonance imaging (MRI) to measure the tunnel position or used cadaveric knee dissection.22) The MRI is an accurate modality to evaluate graft orientation and position, but 3D CT is considered the best standard to evaluate osseous structure.26) To the best of our knowledge, this is the first study to compare the tunnel position of transtibial technique and tibial tunnel-independent technique of ACL reconstruction using 3D CT. The 3D CT was used in an in vivo study which measured femoral and tibial tunnel position, but this study was conducted only on transtibial technique, without comparing the two techniques.26) All cases of both techniques in this study were operated by a single surgeon (JHA) who is a well-experienced expert in the transtibial technique of arthroscopic ACL reconstruction. The difference in tibial tunnel place was not significant between two techniques, whereas the difference in femoral tunnel place was statistically significant between transtibial technique and tibial tunnel-independent technique. Thus, significant difference in femoral tunnel position between the two techniques would not be derived from the variety of surgeon's techniques, but from the outcome difference between the two techniques.
There are several limitations in this study. First, we could not independently measure the anatomic ACL center, which was a reference point to the position of tunnel center in 3D CT. As our study was a clinical in vivo study, we could not measure the center of attached native ACL; and as such, we compared our data with the location of femoral and tibial tunnels in the previous cadaver study.11) However, the study which qualified the position of anatomic anteromedial and posterolateral bundle center for double-bundle ACL reconstruction did not suggest a single anatomic ACL center. We calculated the 2D mean value of anteromedial bundle center and posterolateral bundle center, respectively. Second, this study was without clinical correlation such as stability and clinical scoring between the two methods. Thus, our study could not demonstrate whether other confounding factors affected on the clinical outcome of the independent tibial tunnel technique. Third, the authors preferred to position femoral tunnel close to anteromedial bundle rather than close to native ACL femoral footprint center. Further study is necessary to prove if the tunnel position close to anteromedial bundle deducts clinically and biomechanically better outcome.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Asagumo H, Kimura M, Kobayashi Y, Taki M, Takagishi K. Anatomic reconstruction of the anterior cruciate ligament using double-bundle hamstring tendons: surgical techniques, clinical outcomes, and complications. Arthroscopy. 2007;23(6):602–609. doi: 10.1016/j.arthro.2007.01.009. [DOI] [PubMed] [Google Scholar]
- 2.Heming JF, Rand J, Steiner ME. Anatomical limitations of transtibial drilling in anterior cruciate ligament reconstruction. Am J Sports Med. 2007;35(10):1708–1715. doi: 10.1177/0363546507304137. [DOI] [PubMed] [Google Scholar]
- 3.Getelman MH, Friedman MJ. Revision anterior cruciate ligament reconstruction surgery. J Am Acad Orthop Surg. 1999;7(3):189–198. doi: 10.5435/00124635-199905000-00005. [DOI] [PubMed] [Google Scholar]
- 4.Piasecki DP, Bach BR, Jr, Espinoza Orias AA, Verma NN. Anterior cruciate ligament reconstruction: can anatomic femoral placement be achieved with a transtibial technique? Am J Sports Med. 2011;39(6):1306–1315. doi: 10.1177/0363546510397170. [DOI] [PubMed] [Google Scholar]
- 5.Steiner ME, Battaglia TC, Heming JF, Rand JD, Festa A, Baria M. Independent drilling outperforms conventional transtibial drilling in anterior cruciate ligament reconstruction. Am J Sports Med. 2009;37(10):1912–1919. doi: 10.1177/0363546509340407. [DOI] [PubMed] [Google Scholar]
- 6.Cain EL, Jr, Clancy WG., Jr Anatomic endoscopic anterior cruciate ligament reconstruction with patella tendon autograft. Orthop Clin North Am. 2002;33(4):717–725. doi: 10.1016/s0030-5898(02)00026-3. [DOI] [PubMed] [Google Scholar]
- 7.Scopp JM, Jasper LE, Belkoff SM, Moorman CT., 3rd The effect of oblique femoral tunnel placement on rotational constraint of the knee reconstructed using patellar tendon autografts. Arthroscopy. 2004;20(3):294–299. doi: 10.1016/j.arthro.2004.01.001. [DOI] [PubMed] [Google Scholar]
- 8.Brophy RH, Pearle AD. Single-bundle anterior cruciate ligament reconstruction: a comparison of conventional, central, and horizontal single-bundle virtual graft positions. Am J Sports Med. 2009;37(7):1317–1323. doi: 10.1177/0363546509333007. [DOI] [PubMed] [Google Scholar]
- 9.Arnold MP, Kooloos J, van Kampen A. Single-incision technique misses the anatomical femoral anterior cruciate ligament insertion: a cadaver study. Knee Surg Sports Traumatol Arthrosc. 2001;9(4):194–199. doi: 10.1007/s001670100198. [DOI] [PubMed] [Google Scholar]
- 10.Tsukada H, Ishibashi Y, Tsuda E, Fukuda A, Toh S. Anatomical analysis of the anterior cruciate ligament femoral and tibial footprints. J Orthop Sci. 2008;13(2):122–129. doi: 10.1007/s00776-007-1203-5. [DOI] [PubMed] [Google Scholar]
- 11.Forsythe B, Kopf S, Wong AK, et al. The location of femoral and tibial tunnels in anatomic double-bundle anterior cruciate ligament reconstruction analyzed by three-dimensional computed tomography models. J Bone Joint Surg Am. 2010;92(6):1418–1426. doi: 10.2106/JBJS.I.00654. [DOI] [PubMed] [Google Scholar]
- 12.Bedi A, Altchek DW. The "footprint" anterior cruciate ligament technique: an anatomic approach to anterior cruciate ligament reconstruction. Arthroscopy. 2009;25(10):1128–1138. doi: 10.1016/j.arthro.2009.03.008. [DOI] [PubMed] [Google Scholar]
- 13.Amis AA, Beynnon B, Blankevoort L, et al. Proceedings of the ESSKA Scientific Workshop on Reconstruction of the Anterior and Posterior Cruciate Ligaments. Knee Surg Sports Traumatol Arthrosc. 1994;2(3):124–132. doi: 10.1007/BF01467913. [DOI] [PubMed] [Google Scholar]
- 14.Kaseta MK, DeFrate LE, Charnock BL, Sullivan RT, Garrett WE., Jr Reconstruction technique affects femoral tunnel placement in ACL reconstruction. Clin Orthop Relat Res. 2008;466(6):1467–1474. doi: 10.1007/s11999-008-0238-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Howell SM, Gittins ME, Gottlieb JE, Traina SM, Zoellner TM. The relationship between the angle of the tibial tunnel in the coronal plane and loss of flexion and anterior laxity after anterior cruciate ligament reconstruction. Am J Sports Med. 2001;29(5):567–574. doi: 10.1177/03635465010290050801. [DOI] [PubMed] [Google Scholar]
- 16.Howell SM, Deutsch ML. Comparison of endoscopic and two-incision techniques for reconstructing a torn anterior cruciate ligament using hamstring tendons. Arthroscopy. 1999;15(6):594–606. doi: 10.1053/ar.1999.v15.015059. [DOI] [PubMed] [Google Scholar]
- 17.Kondo E, Yasuda K, Ichiyama H, Azuma C, Tohyama H. Radiologic evaluation of femoral and tibial tunnels created with the transtibial tunnel technique for anatomic double-bundle anterior cruciate ligament reconstruction. Arthroscopy. 2007;23(8):869–876. doi: 10.1016/j.arthro.2007.02.016. [DOI] [PubMed] [Google Scholar]
- 18.Kopf S, Forsythe B, Wong AK, et al. Nonanatomic tunnel position in traditional transtibial single-bundle anterior cruciate ligament reconstruction evaluated by three-dimensional computed tomography. J Bone Joint Surg Am. 2010;92(6):1427–1431. doi: 10.2106/JBJS.I.00655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Behrendt S, Richter J. Anterior cruciate ligament reconstruction: drilling a femoral posterolateral tunnel cannot be accomplished using an over-the-top step-off drill guide. Knee Surg Sports Traumatol Arthrosc. 2010;18(9):1252–1256. doi: 10.1007/s00167-010-1112-6. [DOI] [PubMed] [Google Scholar]
- 20.Abebe ES, Moorman CT, 3rd, Dziedzic TS, et al. Femoral tunnel placement during anterior cruciate ligament reconstruction: an in vivo imaging analysis comparing transtibial and 2-incision tibial tunnel-independent techniques. Am J Sports Med. 2009;37(10):1904–1911. doi: 10.1177/0363546509340768. [DOI] [PubMed] [Google Scholar]
- 21.Harner CD, Honkamp NJ, Ranawat AS. Anteromedial portal technique for creating the anterior cruciate ligament femoral tunnel. Arthroscopy. 2008;24(1):113–115. doi: 10.1016/j.arthro.2007.07.019. [DOI] [PubMed] [Google Scholar]
- 22.Hantes ME, Zachos VC, Liantsis A, Venouziou A, Karantanas AH, Malizos KN. Differences in graft orientation using the transtibial and anteromedial portal technique in anterior cruciate ligament reconstruction: a magnetic resonance imaging study. Knee Surg Sports Traumatol Arthrosc. 2009;17(8):880–886. doi: 10.1007/s00167-009-0738-8. [DOI] [PubMed] [Google Scholar]
- 23.Anderson AF, Snyder RB, Lipscomb AB., Jr Anterior cruciate ligament reconstruction: a prospective randomized study of three surgical methods. Am J Sports Med. 2001;29(3):272–279. doi: 10.1177/03635465010290030201. [DOI] [PubMed] [Google Scholar]
- 24.Fujita N, Kuroda R, Matsumoto T, et al. Comparison of the clinical outcome of double-bundle, anteromedial single-bundle, and posterolateral single-bundle anterior cruciate ligament reconstruction using hamstring tendon graft with minimum 2-year follow-up. Arthroscopy. 2011;27(7):906–913. doi: 10.1016/j.arthro.2011.02.015. [DOI] [PubMed] [Google Scholar]
- 25.Kato Y, Maeyama A, Lertwanich P, et al. Biomechanical comparison of different graft positions for single-bundle anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2012 Mar 15; doi: 10.1007/s00167-012-1951-4. http://dx.doi.org/10.1007/s00167-012-1951-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Lertwanich P, Martins CA, Asai S, Ingham SJ, Smolinski P, Fu FH. Anterior cruciate ligament tunnel position measurement reliability on 3-dimensional reconstructed computed tomography. Arthroscopy. 2011;27(3):391–398. doi: 10.1016/j.arthro.2010.08.018. [DOI] [PubMed] [Google Scholar]
- 27.Zantop T, Petersen W. Double bundle revision of a malplaced single bundle vertical ACL reconstruction: ACL revision surgery using a two femoral tunnel technique. Arch Orthop Trauma Surg. 2008;128(11):1287–1294. doi: 10.1007/s00402-007-0504-7. [DOI] [PubMed] [Google Scholar]