

Abstract
BACKGROUND:
Anxiety is the one of the most common problems before the surgery. Its prevalence rate ranged from 11 to 80 percent in all the adult patients. Delay in wound healing and increasing use of narcotics and anesthetics are some of the other accompanying problems. Aromatherapy is one of the complementary medicine components. It is applied by special type of oil extracted from aromatic plants for medical objectives. This study aimed to investigate the effects of inhalation aromatherapy on anxiety level in preoperative patients.
METHODS:
This was a clinical study done on 72 patients candidate for heart and abdominal surgery admitted in Golestan and Imam Khomeini hospitals. The patients were selected according to our study objectives and inclusion criteria. Then, they were divided in two case and control groups. The Spielberger scale was used for evaluating the anxiety level. Twenty minute of inhalation with handkerchief containing lavandula was used in the case group and placebo also (water) in the control group.
RESULTS:
The average of anxiety level in inhalation aromatherapy group decreased from 51.00 to 38.61 from before to after the intervention. This average in the inhalation group with placebo was 50.67 before the intervention and decreased to 49.53 after the intervention. The results of independent t-test statistically showed a significant difference between the two groups after the intervention.
CONCLUSIONS:
The findings showed that inhalation aromatherapy was effective on reduction of anxiety level and this method can be applied as a complementary medicine on the clinic.
KEY WORDS: Aromatherapy, anxiety, surgery, preoperative period, lavandula
Surgery is an intentional procedure change on body anatomical structure in order to establish relief, tranquilize or remove pathologic part and healing traumatic damages. Anxiety is one of the most common problems before the surgery.1 In the United States, 23 million patients annually undergo surgery and most of them experience anxiety.2
Furthermore, anxiety is the most common psychiatric disorder which is experienced in 15-20 percent of the patients admitted in clinical and health care centers.3
In adult patients, the incidence of preoperative anxiety varied from 11-80 percent.4 Before the surgery, anxiety is resulted often from problems such as pain, morbidity, body image changes, or body function deficiency, dependency, family concerns or probable life style changes.5
The studies showed that severe preoperative anxiety can prevent from expectable wound healing in the postoperative period. High anxiety is associated with high pain level after the surgery,4 reduced ability to resist infections, increase in needing postoperative analgesia, delayed wound healing,6 negative impacts on patient's mood7 and an increase in hospitalization duration.8
It is obvious that reduction in anxiety level would cause beneficial effects such as a better and expeditious recovery, declining in narcotics and palliative injections during anesthesia, pain tolerance and early hospital discharging.9 Considering the mentioned points, we would expect decrease in expenses and surgery complications.
The main objective in preoperative period is to achieve the maximum point of patients’ psychological and physical health, and helping patients to cope with conditions and anxiety is one of the important nursing roles.10
There are two types of pharmacological and non-pharmacological remedies for reducing anxiety. All of the pharmacological methods such as benzodiazepines and analgesics groups need physician's authorization and prescription. Most of the non-pharmacological or complementary methods are safe and without any serious side effects. Many of these methods are branches of the complementary medicine. Aromatherapy is one of them, which has had considerable progress among many countries. In addition, it is the second most common method of complementary therapy accepted by nurses.11 Aromatherapy is the utilization of vaporizable and unstable oils extracted from aroma plants for medical objectives.12 For the first time, it was used in India and Egypt as a remedy for different diseases thousands years ago.13 This method has been recognized by American state boards nurses, as a part of the holistic nursing and also accepted as a nursing intervention in Britain.13,14 In more than 30 countries, nurses are authorized to use complementary medicine such as aromatherapy in holistic nursing care plans.15 Different studies have showed that aromatherapy could be effective in decreasing the anxiety, pain, fatigue and dermal wound healing. We are not exactly sure about its mechanism and the way it affects.13
Generally, aromatherapy is used via bath, massage and inhalation. One of the most applicable aromatic plants is lavandula. It had been used in traditional medicine many years ago. Lavandula belongs to green mints family, herbal and aromatic plants and evergreen plants.
Some of the effects are antibacterial, fungicidal and carminative or anti-bloating, muscle relaxation and analgesia.16 The exact neurologic mechanism of the aromatherapy has not been recognized and there are controversial results in different researches in this field. Study of Saeki and Mayumi (2001) proved the effects of aromatherapy on anxiety reduction.17
Moreover, Lehrner et al. (2005) showed that inhalation aromatherapy with lavandula essence could decline anxiety of patients before dental procedures.18 In this regard, Muzzarelli et al. (2006) in the United States showed that inhalation aromatherapy with lavandula essence was not effective in decreasing anxiety on pre colonoscopy.19 Considering the importance of decreasing anxiety before the surgery and also undesirable side effects on patients recovery as well as nurses’ ability to use the complementary medicine, the researchers decided to evaluate the effects of inhalation aromatherapy on decreasing the preoperative anxiety.
Methods
This was a quasi-experimental clinical trial study on patients who were candidate for thorax and abdominal surgery admitted in Golestan and Imam Khomeini hospitals in Ahvaz.
The inclusion criteria included age more than 18 years, obtaining score higher than 20 from Spielberger questionnaire,20 admitted at the night before the surgery, ability to talk and understand Persian language. The exclusion criteria also included severe acute pain at the time of completing the questionnaire, taking benzodiazepines, analgesics opioids, history of eczema and allergy to plants, migraine, chronic headaches, acute mental illness according to physician diagnosis and olfactory disorder.
Data collection method was based on completing the questionnaire, interviewing and recording the vital signs. In this study, the main data collection tool included a questionnaire containing four parts. The first part contained demographic information such as age, sex, monthly income, educational level, occupation, place of living and mental status. The second part included the data associated with illness such as the history of hospitalization, surgery, the duration of preoperative hospitalization, type of surgery, type of disease and consumed medications.
These two parts contained interventional factors and were arranged according to the previous studies. To evaluate the validity of these two parts of questionnaire, content validity method was used.
The third part of the questionnaire contained a standard questionnaire of Spielberger. It included twenty questions related to State Trait Anxiety Inventory (STAI). The least obtained score of 20 indicated no anxiety and the maximum score of 80 illustrated the highest level of anxiety. The score of 21-39 indicated mild anxiety. The scores 40-59 indicated moderate anxiety and the scores of 60-80 also indicated severe anxiety.20 This questionnaire enjoys universal validity and reliability and its reliability had already been confirmed on 600 people in Mashhad and Cronbach's alpha coefficient obtained 0.94 on the norm population. This questionnaire has been used in local and international studies widely.21 The forth part of the questionnaire included the vital signs recording.
In order to calculate the sample size, a pilot study was performed on 15 people. Then, according to the obtained data by formula under the supervision of a statistic professor, sample size was estimated as 36 subjects for each group according to 0.8 power test, 95% confidence level and clinical significant level d = 8. This was an available-purposive sampling study. The qualified samples were randomly divided into two groups of inhalation aromatherapy and placebo inhalation.
After the initial sampling and taking consent form the patients, the researcher measured the anxiety level according to Spielberger's standard questionnaire, provided with obtaining score higher than 20 first and second parts of the questionnaire were filled and the patient's vital signs were recorded. The intervention was performed as follows: in the inhalation aromatherapy group two drops of lavandula oil (0.1 cc per drop with 100% concentration) was rubbed
on a handkerchief and inhaled by the patient for 20 minute. In the placebo inhalation group also, 2 drops of water was rubbed on handkerchief and inhaled by the patient 20 minute. Thereafter, the Spielberger's questionnaire was recompleted and vital sign were recorded.
After the sampling, data were analyzed using Software SPSS13. In order to review the similarity of changes in individual-familial data and any data related to disease, chi-square test was used. In addition, for comparing the level of anxiety and vital signs, the independent t-test was performed.
Results
The obtained finding showed that in the two groups of case and control, there was no significant statistical difference in term of age, sex, marital status, occupation, monthly income, educational level, ethnicity, insurance status, place of living, type of surgery, history of surgery and hospitalization, the number of the days hospitalized and the level of anxiety (p > 0.05).
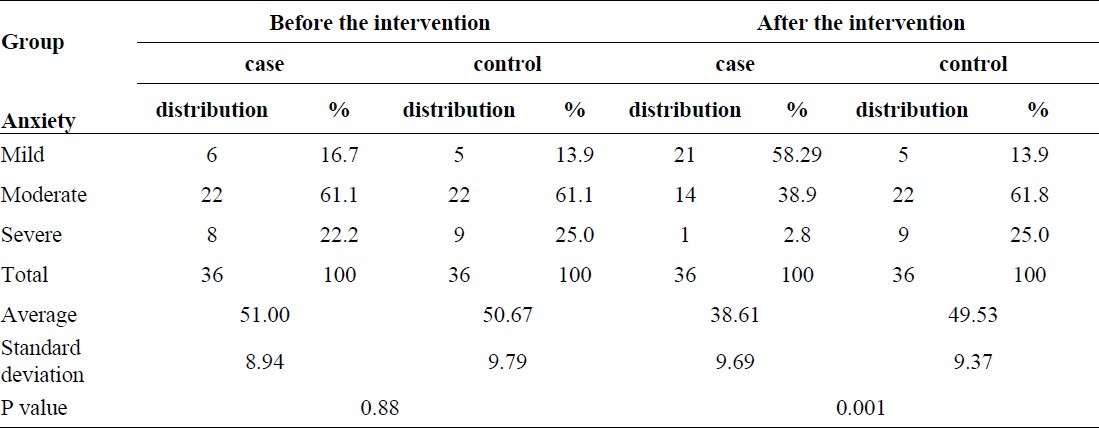
The mean level of anxiety before the intervention in the case group was 51.00 that decreased to 38.61 after intervention. However, in the control group it was 50.67 before the intervention and reached to 49.53 after the intervention.
The mean differences before and after the intervention were 12.388 in case group and 2.416 in control group. The independent t-test showed that there was no significant statistical difference in the both groups before the intervention; however, after the intervention both groups had a significant statistical difference (p = 0.001).
The results of the present study about anxiety control before the intervention showed that the highest distribution in case and control group (61.1%) before intervention had the moderate anxiety that after the intervention the maximum frequency of anxiety (58.29%) in the case group had mild anxiety but in the control group it was the same as before the intervention with highest frequency of samples with moderate anxiety (61.1%). Chi-square test showed a significant difference between the two groups in this regard (p = 0.001) (Table 1).
Table 1.
The distribution of anxiety level in the two groups of case and control
Thus, reviewing the vital signs before and after the intervention demonstrated that there was no significant statistical difference in terms of mean pulse rate, respiratory rate, temperature, and diastolic blood pressure in the two groups (p > 0.05). However, there was a significant statistical difference in terms of mean differences of systolic blood pressure before and after the intervention in the two groups (p < 0.05).
Discussion
Anxiety is an unpleasant feeling, pressure and phobia. In those with anxiety, the main reason is fear from disease, hospitalization, anesthesia or surgery, and is associated with physiologic and behavioral, emotional and cognitive symptoms10,22 which are seen in 15-20% of the patients in the medical clinics.3 Nowadays, anxiety is proved as a harmful phenomenon for patients. Muzzarelli's study (2006) showed that inhalation aromatherapy with lavender essence had no effect on reducing anxiety of the patients (p = 0.63) which was not in accordance with the present study. Perhaps this might be due to doses of lavender used in Muzzarelli's study. In the study of Muzzarelli, lavender essence (10%) that had been solved with grape's seeds oil was used.19 But in this study, pure herbal essences oil had been used. The other reason of dissimilarity could be due to length of inhalation. The length of inhalation in Muzzarelli's study was 5 minutes while it was 20 minutes in the present study.
The study of Lehrner et al. indicated that inhalation aromatherapy with lavender essence could reduce anxiety level before the dental procedure (p = 0.039), which was in accordance with the results of this study.18 The length of inhalation in the both study was 20 minutes.
The accurate mechanism of aromatherapy is not identified yet. It is believed that aromatherapy can effect through psychological and physical methods. The odor of aroma makes olfactory nerve cells active and it would lead to motivate limbic system. Depending on the type of aroma, nerve cells release different neurotransmitters. These neurotransmitters are including encephalin, noradrenalin and serotonin. On the other hand, considering the association between olfactory with psyche and emotions of human can effect on human spirit and physic, constantly. In fact, odors can change feeling in humans.13
Studies about benefits of lavender's aroma showed - that linalool and linalyl acetate existing in this plant can stimulate parasympatic system. In addition, linalyl acetate has narcotic effects and linalool acts as a sedative. However, accurate mechanism of neurological function of lavandula is not identified yet.
Some of studies stated that lavandula may have effects similar to benzodiazepines and it can increase the effects of Gabaaminobutyric acid and through which it acts as an anti-anxiety effect.16
The acquired result from Garham et al. in Australia showed that inhalation aromatherapy did not affect on reducing anxiety in patients who underwent radiotherapy, even the level of anxiety in the control group was less than aromatherapy group. Researcher believed that this increase in anxiety was due to association between specific odor and anxiety caused by radiotherapy.23 which was not in accordance with the results of the present study. Furthermore, the other finding of this study showed that inhalation aromatherapy caused reduction in systolic blood pressure in patients.
The study of Hwang et al. about the effects of inhalation method using essential oils on blood pressure and stress responses showed that inhalation aromatherapy was an effective intervention that caused decrease in blood pressure (p < 0.05).24 It was in accordance with the present study.
The study of Shiina et al. showed that inhalation aromatherapy had no effect on blood pressure which was not in accordance with the results of the present study.25 Perhaps, the cause might be due to the difference in dosage of essential oils used in the two studies. Shiina used 4 drops of lavender mixture with 20 ml of water for inhalation. While in the present study, this essence was used without being diluted.
Moreover, study of Saeki and Mayumi showed that 10 minutes inhalation of lavender essence can cause reduction in systolic blood pressure which was in accordance with the present study.17 The reason why this happened only on systolic blood pressure and not on the diastolic blood pressure could be concluded that to create a change in diastolic BP, long intervention is needed and stress resulted from surgery is state anxiety and diastolic blood pressure has low variation compared with systolic blood pressure.
However, the findings related to vital signs in this study were the observation of the researcher and are considered as an adverse finding and explaining the effects of intervention require large sample size and longer intervention.
Conclusion
Since the main objective of the preoperative care is to maximize the patient's physical and mental health1 and helping the patients to be adapted with the situations and overcoming anxiety is one of the nurses’ responsibilities; a nurse plays an important role to make the patients ready, emotionally and mentally in preoperative period.26,10 The results of this study showed that inhalation aromatherapy had positive effects on reducing anxiety in patient before the surgery which is recommended as a new and easy alternative for nurses in order to reduce anxiety in the patients. For scientific advance and promotion in quality of nursing interventions, further studies about long-term effects of usage of this method for reducing anxiety disorders is recommended.
The authors declare no conflict of interest in this study.
Acknowledgments
Thanks go to Professor Haghighizadeh the statistics counselor, and all the staffs of Imam Khomeini and Golestan hospitals in Ahvaz for helping us to conduct this study. Furthermore, we would appreciate from Mrs. Fataneh Ghadirian and Kobra Karami.
References
- 1.Nikravan Mofrad M, Atashzadeh Shoorideh F. Principles of patient care, comprehensive nursing approach. Tehran: Ghazi Jahan; 2003. [Google Scholar]
- 2.Roohy GR, Rahmany A, Abdollahy AA, Mahmoody GhR. The effect of music on anxiety level of patients and some of physiological responses before abdominal surgery. Journal of Gorgan University of Medical Sciences. 2005;7(1) [Google Scholar]
- 3.Ghardashi F, Salehe Moghadam A, Hasanabadi H, Setayesh Y. Correlation Between Duration of Waiting Befor Surgery and Anxiety of Patients. Scientific Journal of Sabzevar University of Medical Sciences. 2003;4(30) [Google Scholar]
- 4.Agarwal A, Ranjan R, Dhiraaj S, Lakra A, Kumar M, Singh U. Acupressure for prevention of pre-operative anxiety: a prospective, randomised, placebo controlled study. Anaesthesia. 2005;60(10):978–81. doi: 10.1111/j.1365-2044.2005.04332.x. [DOI] [PubMed] [Google Scholar]
- 5.O’Brien ME. Spirituality in Nursing: Standing on Holy Ground. 2nd ed. Sudbury: Jones and Bartlett Publishers; 2002. [Google Scholar]
- 6.Granot M, Ferber SG. The roles of pain catastrophizing and anxiety in the prediction of postoperative pain intensity: a prospective study. Clin J Pain. 2005;21(5):439–45. doi: 10.1097/01.ajp.0000135236.12705.2d. [DOI] [PubMed] [Google Scholar]
- 7.Montgomery GH, Bovbjerg DH. Presurgery distress and specific response expectancies predict postsurgery outcomes in surgery patients confronting breast cancer. Health Psychol. 2004;23(4):381–7. doi: 10.1037/0278-6133.23.4.381. [DOI] [PubMed] [Google Scholar]
- 8.Frazier SK, Moser DK, Daley LK, McKinley S, Riegel B, Garvin BJ, et al. Critical care nurses’ beliefs about and reported management of anxiety. Am J Crit Care. 2003;12(1):19–27. [PubMed] [Google Scholar]
- 9.Mahfoozi A, Hasani Mian M. Effect of midazolam on anxiety reduction surgery. Journal of legal medicine. 2000;19:20. [Google Scholar]
- 10.Pudner R. Nursing the Surgical Patient. 2nd ed. Philadelphia: Elsevier; 2005. [Google Scholar]
- 11.Tseng YH. [Aromatherapy in nursing practice] Hu Li Za Zhi. 2005;52(4):11–5. [PubMed] [Google Scholar]
- 12.Mahmoodi B. Introduction to aromatic oils and herbal healing effects of their medical prescriptions drugstore including aromatic. 1st ed. Tehran: Noore Danesh; 2002. [Google Scholar]
- 13.Kyle G. Evaluating the effectiveness of aromatherapy in reducing levels of anxiety in palliative care patients: results of a pilot study. Complement Ther Clin Pract. 2006;12(2):148–55. doi: 10.1016/j.ctcp.2005.11.003. [DOI] [PubMed] [Google Scholar]
- 14.Soden K, Vincent K, Craske S, Lucas C, Ashley S. A randomized controlled trial of aromatherapy massage in a hospice setting. Palliat Med. 2004;18(2):87–92. doi: 10.1191/0269216304pm874oa. [DOI] [PubMed] [Google Scholar]
- 15.Buckle J. Aromatherapy: What Is It? HerbalGram. 2003;57:50–6. [Google Scholar]
- 16.Daghighbin E. Comparison of Honey and Lavender Cream on Pain and Wound Healing in Primigravidas Episiotomy. Ahvaz: Ahvaz Junishapur University of Medical Sciences; 2007. [Google Scholar]
- 17.Saeki Y, Mayumi S. Physiological effects of inhaling fragrances. The International Journal of Aromatherapy. 2001;11(3):118–25. [Google Scholar]
- 18.Lehrner J, Marwinski G, Lehr S, Johren P, Deecke L. Ambient odors of orange and lavender reduce anxiety and improve mood in a dental office. Physiol Behav. 2005;86(1-2):92–5. doi: 10.1016/j.physbeh.2005.06.031. [DOI] [PubMed] [Google Scholar]
- 19.Muzzarelli L, Force M, Sebold M. Aromatherapy and reducing preprocedural anxiety: A controlled prospective study. Gastroenterol Nurs. 2006;29(6):466–71. doi: 10.1097/00001610-200611000-00005. [DOI] [PubMed] [Google Scholar]
- 20.Spielberger C. Manual for the State Trait Anxiety Inventory. CA USA: Consulting Psychologists Publishers; 1983. [Google Scholar]
- 21.Abolhasani S. Effect of sensory stimulation on signs of sleep deprivation and heart inductor in patient on Intensive Care Unit [Thesis] Isfahan: School of Nursing and Midwifery, Isfahan University of Medical Sciences; 2002. (Persian) [Google Scholar]
- 22.Videbeck SL. Psychiatric Mental Health Nursing. 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 2003. [Google Scholar]
- 23.Graham PH, Browne L, Cox H, Graham J. Inhalation aromatherapy during radiotherapy: results of a placebo-controlled double-blind randomized trial. J Clin Oncol. 2003;21(12):2372–6. doi: 10.1200/JCO.2003.10.126. [DOI] [PubMed] [Google Scholar]
- 24.Hwang JH. [The effects of the inhalation method using essential oils on blood pressure and stress responses of clients with essential hypertension] Taehan Kanho Hakhoe Chi. 2006;36(7):1123–34. doi: 10.4040/jkan.2006.36.7.1123. [DOI] [PubMed] [Google Scholar]
- 25.Shiina Y, Funabashi N, Lee K, Toyoda T, Sekine T, Honjo S, et al. Relaxation effects of lavender aromatherapy improve coronary flow velocity reserve in healthy men evaluated by transthoracic Doppler echocardiography. Int J Car-diol. 2008;129(2):193–7. doi: 10.1016/j.ijcard.2007.06.064. [DOI] [PubMed] [Google Scholar]
- 26.Farahi H. Counseling and psychotherapy with children and adolescents (theory and practical applications in schools and health centers) 1st ed. Tehran: Arjmand; 2004. [Google Scholar]