

Abstract
BACKGROUND:
Breast cancer is the first-rank malignancy in women. Although surgery is the most common method of treatment, patients experience many threats both from the cancer and from the surgery itself. Exercises such as walking can improve body mass index, attitudes and life quality of patients. The aim of the present study was to determine the effect of walking on physical aspect of quality of life (QOL) in mastectomy patients in 2007.
METHODS:
Thirty four mastectomy patients took part in the study. Walking was performed in a flat surface 3 times a week, each lasting 30 minutes over 6 weeks. Data were collected by a questionnaire before and after the intervention and a self-report form. After identifying content and face validity of the questionnaire, its reliability was measured by Cronbach's alpha (α = 0.89) and test-retest (r = 0.91) methods.
RESULTS:
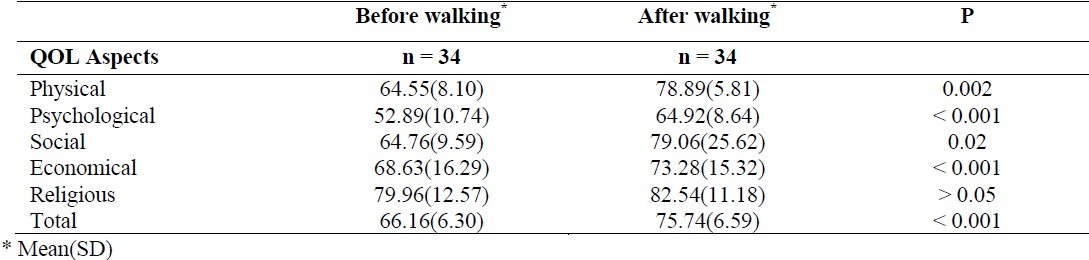
Mean scores (standard deviations) of physical, psychological, social, economic and religious aspects of QOL before the intervention were 64.55(8.10), 78.89 (5.81), 52.89 (10.74), 64.92 (8.64) and 64.76 (9.59), respectively. These aspects were 79.06 (25.62), 68.63 (16.29), 73.28 (15.32), 79.96 (12.57) and 82.54 (11.18) after the intervention, respectively. Total mean scores of QOL before the intervention was 66.16 (6.30) and increased to 75.74 (6.59) after the intervention with a significant difference in all aspects except the religious aspect. Therefore, this study showed the positive effects of walking on QOL of mastectomy patients.
CONCLUSIONS:
Patients with breast cancer experience physical as well as psychological malfunctions and fatigue during the condition and its treatment. Walking can solve many of their problems and, ultimately, improve their QOL.
KEY WORDS: Walking, quality of life, mastectomy, neoplasms
Breast cancer is malignant proliferation of epithelial cells in milk ducts and lobules.1 Cancer is the second leading cause of death after cardiovascular diseases in the United States.2 Breast cancer is the most common malignancy in women with an estimation of a catastrophic increase until 2030.3 In Iran, statistics show that breast cancer is the most common malignancy in women and the 22nd in men (2008). It is estimated that 1897 deaths have occurred in 2008 due to breast cancer and this malignancy accounts for 25.4% of all cancers in women. Surgery significantly affects on body image of the patients. Physical exercise during therapy of breast cancer can reduce the resultant fatigue and depression and lead to better quality of life (QOL) of the patients.4,5
Surgery is one of the common and definite interventions in cancer. However, patients experience many threats both from the disease itself and from the surgery.6 Women with breast cancer suffer from severe stress, anxiety and depression lasting many years after recovery. Functional limitations such as decreased shoulder movement and frozen shoulder keep the women away from daily activities and lower their QOL permanently by causing depression.7
QOL is a multidimensional and dynamic concept. The dynamic nature helps researchers investigate for better life style in people.8 Physical activity and exercise result in such changes as decreased body mass index, increased cardiac reserve and improved nutrition, pulmonary perfusion as well as mood. They reduce fatigue by restoring bodily functions. Exercises such as regular walking, without changing other habits, can improve body mass index, anthropometric criteria, attitude and QOL in patients with breast cancer.9
Many studies have been performed regarding the effects of exercise on life quality of patients with breast cancer. Sandel et al. conducted a study to identify the effects of activity and dance programs on improving life quality criteria in patients survived from breast cancer in the United States. Thirty eight patients were divided into 2 experimental and waiting-list groups and they performed preset movements in a cross-over format. The latter was asked to have their routine activities from week 1 to 12 and to perform scheduled movements from week 14 to 25. In contrast, the experimental group was asked to perform the movements in the first 12 weeks and to resume their routine activities in the second 12 weeks.7
The sequence of intervention had no effect on results. Meanwhile, no evidence was found regarding the relapse of the experimental group to the original state during weeks 13 to 26 and the temporariness of the outcomes since the intervention satisfied the physical and emotional needs of the patients and improved their QOL. Thus, in the first 12 weeks, the quality increased in the experimental group and, in the second 12 weeks, in the waiting-list group. The maintenance of the results in the second phase of the intervention (routine activities) in the experimental group showed the stability of the outcomes and similar improvements in both groups reinforced the findings.7
Wilson et al (2005) conducted a study regarding the effects of walking on physical profile of African-American women in the US. They studied about these effects at the beginning, immediately after and 3 months after the intervention. 24 available women participated in the walking program and educational as well as problem-solving classes to enhance their motivation for 8 weeks. Results showed that daily mean of walking steps increased from 4791 to 8297 with a significant decrease in body mass index (BMI), weight, body fat percentage and motion range of elbow from the beginning until immediately after the intervention. 3 months after the intervention, hip rotation, motion range of elbow and diastolic pressure improved and total physical profile remained similar to those of immediately after the intervention. In addition, incremental walking improved QOL in all aspects.9
Accordingly, with respect to increasing rate of breast cancer and its effects on different aspects of life, this quasi-experimental study was conducted to determine the effects of walking on QOL of mastectomy patients.
No similar study has been conducted in Iran before and such a study can be performed with respect to facilities, instruments and availability of patients. No complicated devices are needed and the study is applicable, practical and attainable over a relatively short time. The study can reflect the effects of noninvasive as well as inexpensive therapeutic methods on the QOL of mastectomy patients. This has always been a concern for health authorities to advise such methods which can lead to improved self-esteem, self-image, and self-control of cancer patients in a cost-effective way.
This quasi-experimental one-group study was conducted to determine and compare the effects of walking on QOL of mastectomy patients at selected hospitals in Tehran, Iran in 2007.
The aim of this study was to identify relationships between personal characteristics of the patients and QOL alterations (physical, psychological, social, economic and spiritual condition) after the intervention and to identify the relationships between changes in QOL domains (physical, psychological, social, economic and spiritual condition) of the patients after the intervention.
Methods
Subjects were selected by convenient and purposive sampling methods in Shohadaye Tajrish, Imam Khomeini, and Hazrate Rasul hospitals randomly from different hospitals. 32 patients were calculated. The subjects were selected with respect to the following criteria:
Age between 30-60;
At the 1st or 2nd stage of breast cancer;
Under modified unilateral mastectomy;
At least 3 months after therapy;
No history of chronic or underlying diseases such as cardiovascular, respiratory, renal, hepatic conditions or cancer as well as ambulatory limitations;
No history of psychological disorders;
No history of postoperative walking
Data collection tools contained a questionnaire and a report form. In the form, detailed data regarding walking including day, date, times of start and end, pulse rates before and after it, number of persons and a space for notes were documented in a table. The questionnaire consisted of 2 parts: demographics and QOL items. It was designed by examining different related references such as Quality of Life Instrument-Breast Cancer PatientVersion10 with 46 statements scored in a 10-scale format and divided into 4 domains (physical, psychological, socioeconomic and spiritual) and SF-36 QOL questionnaire translated, validated and made reliable in Iran. Content and face validities of the questionnaire were identified and it was made reliable by internal consistency (Cronbach's α = 91%) and test-retest method (r = 0.89).
Table 1.
QOL aspects before and after the intervention in mastectomy patients at hospitals of Tehran
Paired t test, Spearman and Mann-Whitney statistical tests were used for data analysis. Mean scores of QOL in physical, psychological, social, economic and spiritual domains before and after the intervention were compared by paired t test and, after grouping of the subjects, the effects of demographic variables on QOL before and after the intervention were compared by Mann-Whitney and Spearman tests in all domains.
The questionnaire had 49 items with five physical, psychological, social, economic, and religious domains. Each question had 4 scores (0-4) and the maximum scores in each domain were 56, 80, 32, 12 and 16 respectively with total score of 196. Conversion of scores to percent in all domains led to having 3 ranges for QOL [low (0-33%), moderate (34-67%) and high (67-100%)].
By the use of medical records of the patients, those with the following criteria were selected: age between 30 and 60; stage 1 or 2 of cancer; history of modified radical mastectomy at least 3 months before; no history of chronic diseases such as cardiovascular, respiratory, renal, hepatic as well as cephalic disorders, cancer, mobility limitations, and mental disorders; orient; no history of walking following mastectomy; and literacy. They were contacted by phone and the purpose and methods of the study were completely explained to them. During the first visit, the subjects first signed a consent form and then completed the questionnaire.
They were provided a self-report form. They were instructed to measure their carotid pulse and the desired heart beat (50-70% of maximum beat) for each subject was individually calculated and provided to them. The subjects were then instructed to walk in a flat surface for 30 minutes 3 times a week over 6 weeks during daily hours. They measured and documented their pulse rate before and after each walk. They walked in a way that their pulse rate reached 50-70% of their maximum rate and still could speak. All subjects walked with comfortable clothes and shoes. The self-report form was completed by the subjects after each session of walking. The questionnaire for QOL was also completed by the subjects before walking and after 6 weeks in a suitable place. Subjects’ questions were replied by the researchers instantly. During the intervention, the subjects were followed up by telephone calls or random visits.
Results
Findings showed the following demographic characteristics: the mean age of 44.1% of the subjects were 41-50 years; 55.9% of them were married; 35.3% had high school diploma; 52.9% were housekeepers; 26.5% of the subjects’ husbands had high school diploma; 26.5% of the subjects’ husbands were retired and 26.5% were businessmen; 44.1% of them had monthly income between $300 and $450; 41.2% of them had been diagnosed with breast cancer 13-24 months before; 38.2% of them had started their initial treatment 13-24 months before; the mean duration of treat-ment was 19.29 ± 11.68 months; 47.1% of the subjects had 25 radiotherapy sessions.
Discussion
Paired t test showed the significant and positive effects of walking on QOL of women with breast cancer after mastectomy. All subjects gained high scores in terms of religious aspect before and after the intervention. Therefore, no statistically significant difference was found. Strauss-Blasche et al. in their study regarding the effects of breast cancer on QOL of women found that patients suffer from physical dysfunction and fatigue during disease process and its treatment.11 Jennen and Uhlenbruck studied the effects of exercise on QOL of patients with breast cancer and found a significant improvement and higher scores of QOL in exercise group rather than control group.12
In the study of Basen-Engquist et al., it was found that exercises such as walking can significantly increase QOL of patients with breast cancer. They suggested that physical aspect of QOL improve more persistently than other aspects. They also found that light exercises related to life style and applicable during daily activities may have better effects on physical function and QOL of patients with breast cancer since these activities need no special facilities, cost and long-term instructions and are accessible with no negative influences on the disease.13 The effects of walking on life satisfaction of mastectomy patients as a future study is recommended.
The authors declare no conflict of interest in this study.
Limitations
Some personal differences might have influenced the results.
The results might be affected by daily events beyond the control of researchers.
Acknowledgments
We wish to express our gratitude to all the authorities of Shaheed Beheshti University, Faculty of Nursing and Midwifery and employees of medical record departments of Shohadaye Tajrish, Imam Khomeini, and Hazrate Rasul hospitals and all the patients who participated in this study for their sincere cooperation.
References
- 1.Harrison TR, Kasper DL. Harrison's principles of internal medicine. 16th ed. New York: McGraw-Hill; 2005. [Google Scholar]
- 2.Brunner LS, Suddarth DS, O’Connell Smeltzer SC, Bare BG. Brunner & Suddarth's textbook of medical-surgical nursing. 10th ed. Philadelphia: Lippincott Williams & Wilkins; 2004. [Google Scholar]
- 3.Mandelblatt J, Figueiredo M, Cullen J. Outcomes and quality of life following breast cancer treatment in older women: when, why, how much, and what do women want? Health Qual Life Outcomes. 2003;1(11):45. doi: 10.1186/1477-7525-1-45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mohaghagei M. National cancer Registry, [Project] Tehran: Cancer institute, Tehran University; 1992. [Google Scholar]
- 5.Mohaghagei M. Survival analysis of breast cancer patients in Imam Khomini hospital Tehran. Proceedings of the 10th Annual conference of cancer institute; 1995 Oct 12-14; Tehran, Iran. 1995 [Google Scholar]
- 6.Chan CW, Hon HC, Chien WT, Lopez V. Social support and coping in Chinese patients undergoing cancer surgery. Cancer Nurs. 2004;27(3):230–6. doi: 10.1097/00002820-200405000-00009. [DOI] [PubMed] [Google Scholar]
- 7.Sandel SL, Judge JO, Landry N, Faria L, Ouellette R, Majczak M. Dance and movement program improves quality-of-life measures in breast cancer survivors. Cancer Nurs. 2005;28(4):301–9. doi: 10.1097/00002820-200507000-00011. [DOI] [PubMed] [Google Scholar]
- 8.Potter PA, Perry AG. Basic nursing: a critical thinking approach. Philadelphia: Mosby; 1999. [Google Scholar]
- 9.Wilson DB, Porter JS, Parker G, Kilpatrick J. Anthropometric changes using a walking intervention in African American breast cancer survivors: a pilot study. Prev Chronic Dis. 2005;2(2):A16. [PMC free article] [PubMed] [Google Scholar]
- 10.Ferrell BR, Grant M. Quality of life instrument – Breast cancer patient version. 1995. Available at: http://prc.coh.org/pdf/QOL%20Breast%20Cancer%20Pt.pdf .
- 11.Strauss-Blasche G, Gnad E, Ekmekcioglu C, Hladschik B, Marktl W. Combined inpatient rehabilitation and spa therapy for breast cancer patients: effects on quality of life and CA 15-3. Cancer Nurs. 2005;28(5):390–8. doi: 10.1097/00002820-200509000-00009. [DOI] [PubMed] [Google Scholar]
- 12.Jennen C, Uhlenbruck G. Exercise and Life-Satisfactory-Fitness: Complementary Strategies in the Prevention and Rehabilitation of Illnesses. Evid Based Complement Alternat Med. 2004;1(2):157–65. doi: 10.1093/ecam/neh021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Basen-Engquist K, Taylor CL, Rosenblum C, Smith MA, Shinn EH, Greisinger A, et al. Randomized pilot test of a lifestyle physical activity intervention for breast cancer survivors. Patient Educ Couns. 2006;64(1-3):225–234. doi: 10.1016/j.pec.2006.02.006. [DOI] [PubMed] [Google Scholar]