

Abstract
Background:
Efficacy of preemptive analgesia with nonsteroidal antiinflammatory drugs (NSAIDs) in comparison with acetaminophen is controversial. The present study evaluates the preemptive analgesia efficacy of celecoxib and acetaminophen in comparison with placebo for postoperative pain relief in patients who underwent orthopedic surgery under general anesthesia.
Materials and Methods:
Ninetypatients eligible for elective distal extremity surgery were categorized in three groups: group C includedpatients who received oral celecoxib 200 mg 2 h before surgery; group A included those who received oral acetaminophen 320 mg 2 h before surgery; and group P included those who received oral placebo 2 h before surgery. Pain scores were recorded at 4, 12, and 24 h after operation.
Results:
The pain scores 4 h after operation was significantly less in group C than in groups A and P (4.7±1.7 vs. 5±1.5 vs. 6.8±1.7, respectively, P = 0.015). No significant difference was noted in pain scores at 12 h (4.6±2, 4.9±1.9, 4.3±1.4 in group A, group C, group P, respectively P > 0.05) and 24 h (3.1±1.7, 3.0±1.4, 3.3±1.7 in group A, group C, group P, respectively, P > 0.05) after operation among the three groups.
Conclusion:
Using oral celecoxib 200 mg 2 h before operation is better thanusing oral acetaminophen 320 mg 2 h before the beginning of surgery for control of postoperative pain in patients who underwent lower extremity orthopedic surgery under general anesthesia.
Keywords: Celecoxib, acetaminophen, postoperative pain, preemptive analgesia, analgesia, orthopedic surgery, elderly patients
INTRODUCTION
Adequate dose of analgesia is important in postoperative care in patients undergoing surgery.[1,2] Management of acute postoperative pain is suboptimal. As many as 80% of patients report moderate-to-extreme pain following surgery.[1] It has been demonstrated previously that up to one-third of patients suffer moderate-to-severe postoperative pain owing to inadequate analgesia.[2,3] On-demand intramuscular opiates fail to produce adequate pain relief for more than 80% of patients. A combination of opioids, nonsteroidal antiinflammatory drugs (NSAIDs),[1,2] and local anesthetic agents provides good pain relief. Although opioids provide effective pain relief, they are associated with known side effects. Apprehension concerning potential adverse side effects of opioids, such as emesis, excessive sedation, and risk of respiratory depression and addiction, has contributed to underutilization of prescribed opiates.[3,4]
The analgesic effect and lack of opioid-induced adverse effects of NSAIDs have popularized their use in the treatment ofpostoperative pain. Due to gastrointestinal, renal and coagulation adverse effects of these drugs, high dose and prolonged therapy are harmful. Celecoxib, a cyclooxygenase (COX2) inhibitor, is a member of the NSAIDs group with potent analgesic and antiinflammatory properties.[2–10] It was shown that compared with conventional NSAIDs, celecoxib has fewer gastrointestinal side effects with long-term use.[8–12]
Acetaminophen is a nonnarcotic analgesic and antipyretic drug but has no antiinflammatory effects.[13–17]
The concept of preemptive analgesia has gained popularity and previous studies have demonstrated the value of preemptive effect of some drugs such as opioids, local anesthetics,and NSAIDs.[6,10] Experimental studies with animal pain models have demonstrated that brief noxious stimuli, which are perceived as pain, may result in long-lasting neuronal sensitization. When this sensitization occurs, innocuous stimuli may be perceived as pain.[6–8] Surgical procedures, even skin incisions, may result in this initial sensitization. These observations on the genesis and perception of pain led to the concept that analgesia administered before an initial noxious stimulus may be more effective than the same dose given later.
Concepts for control of postoperative pain have progressed as a result of the discovery that early control of pain can alter its subsequent evolution, the recognition that nociception produces important physiological responses even in adequately anesthetized individuals, and an understanding that for many patients minimization of pain can improve clinical outcomes.[6,9]
Al-Sukhun et al.[18] showed that oral administration of 200 mg celecoxib preemptively before surgery had superior analgesic effect for relief of postoperative pain when compared with the other NSAIDs. Toms et al.[19] concluded that using a single dose of oral paracetamol (acetaminophen) preemptively provided effective analgesia in about 50% patients with acute postoperative pain.
As our literature review showed, there was no previous study to compare the preemptive analgesic effect of oral celecoxib with oral acetaminophen in patients who underwent orthopedic surgery. Hence, we designed the present study to compare the preemptive analgesic efficacy of oral celecoxib 200 mg with oral acetaminophen 320 mg in patients eligible for elective distal extremity surgery under general anesthesia.
MATERIALS AND METHODS
Afterobtaining institutional approval from the ethics committee of the University and taking written informed consent from the patients, thisrandomized, double-blind, prospectiveclinicaltrialstudywasperformed in 90Americane Social Anesthesia (ASA )I and II patients, aged 18–65 years and who wereeligiblefor electivesurgery of distal extremity. The other inclusion criteria were patients without pulmonary, renal, hepatic, or cardiovascular disease, without allergy to the study drugs and without history of drug abuse. If anesthesia technique was changed for some reason or if there was intra-operative bleeding which necessitated blood transfusion, the patient was excluded from the study. This study was performed throughout 2003–2004 in the Alzahra teaching hospital of Isfahan University of Medical Sciences.
A formal sample size calculation was performed. From previous work the standard deviation of visual analogue scale (VAS) pain scores was approximately 1.5 cm. A two-sided significance level of 0.05 and a power of 80% were used with a specified mean difference of 1 cm. The calculated sample size was 24 patients in each group.
The patients were randomized according to table of random numbers into one of the three groups; group C included patients who received oral celecoxib 200 mg 2 h before surgery; group A included those who received oral acetaminophen 320 mg 2 h before surgery; group P included those who Received oral placebo 2 h before surgery.
We used an online random number generator to create a list of random numbers, based on our specifications. Our specification was generation of 90 random numbers in which the minimum value was 1 and the maximum value was 3 while we allowed duplicate entries without Seed. After hitting the calculate button, atable of 90 random numbers according to our specification was produced. The first patient received treatment number 2 while the second patient received treatment number 3 and randomization was continued till 90 patients received one of the three treatments. One possible limitationwith this method of randomization is that itdemonstratesalack of predictability in the values. This may be overcome by plotting consecutive pairs on a scatterplot. If the sequence was truly random then such a plot should show no correlation. We relied onthe sequence of random numbers and assumedit to be truly random. Hence, we didnot plot them on a scatterplot.This can be considered as one of the limitations of our study. Sequence allocation and patient enrolment were carried out by two physicians who were blinded to data collection. The participants were assigned to the intervention by a nurse who was not involved in data collection.
The study drugs were prepared as capsules ofsimilar size, shape, and color. Placebo was prepared using starch. We used closed packets with numbers from randomization list written on them for each patient. The patients received the study drugs with 150 ml water in the reception part of the operating room by a nurse who was not involved in data collection.
Peak plasma concentration of celecoxib occurs about 3 h after ingestion.[20] Hence, we administered celecoxib 2 h prior to surgery. Plasma half-life of acetaminophen is between 1 and 2.5 h in normal, healthy patients.[21] Hence, we administered acetaminophen 2 h prior tosurgery.
After patient arrival to the operating room, mean arterial pressure (MAP), heart rate (HR), and oxygen saturation of arterial blood (SpO2) were recorded at 20 min intervals during operation. All patients received a standard anesthetic and no premedication was administered. Patients were induced with fentanyl (2g/ kg), thiopental (5mg/kg), and atracurium (0.5mg/kg).
Anesthesia was maintained with 50% nitrous oxide and oxygen, adding inhaled agent 1.25%isoflurane. The patients also received intravenous morphine (0.1 mg/kg) before incision as analgesic. After operation, the administration of anesthetic gas was terminated and muscle relaxant was reversed by using neostigmine 0.04 mg/kg and atropine 0.02mg/kg intravenously. After reversal of muscle relaxant, if the patient's airway reflex was reversed, extubation was performed and the patient was transferred to the postanesthesia care unit (PACU).
The primary objectiveof the study was to measure postoperative pain based on VAS and rescue analgesic consumption. The secondary outcome of the study was to record duration of PACU stay, occurrence of postoperative vomiting, demographic data, and duration of surgery.Collection of data was performed by an anesthesia nurse who had no knowledge of the group to which the patient belonged.
The pain score was assessed using VAS (from 0 cm, no pain, to 10 cm, worst possible pain) at 4, 12, and 24 h after operation. Duration of recovery room stay was recorded based on using Modified Aldrete's Scoring system.[22] An investigator, without any knowledge of the group to which the patient belonged, recorded pain scores and analgesic requirements.
For postoperative pain management, we administered morphine 0.05mg/kg at 6 h intervals. If patients had pain with VAS≥4, we administered additional dose of morphine 0.05 mg/kg.All enrolled patients completed the study. Statistical analysis was performed using repeated measures ANOVA. Significance was assumed at the 5% level.
RESULTS
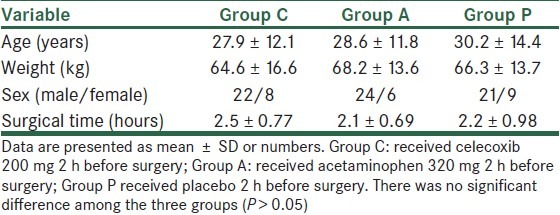
A total of 90 patients were enrolled in the study from September 2003 to September 2004. Flow diagram of randomized patients is illustrated in Figure 1. There was no significant difference among the three groups with respect to age and sex of the patient and surgical time [Table 1].
Figure 1.
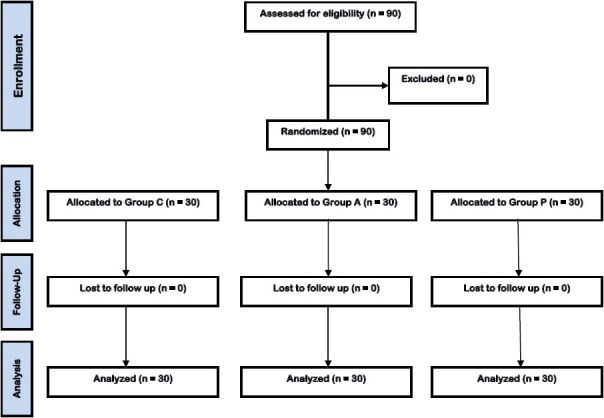
Flow diagram of randomized patients
Table 1.
Demographic characteristics and duration of operation in the three groups
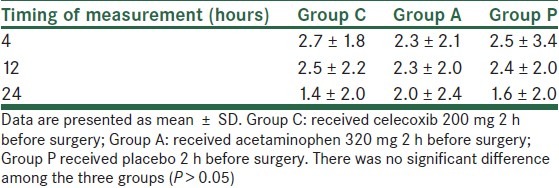
The pain score at 4 h after operation was significantly less in group C compared with group A and group P (P<0.05) [Table 2]. The mean dosage of rescue analgesic used for postoperative pain was no significantly different in the three groups (P> 0.05) [Table 3].
Table 2.
The VAS scores at different time intervals after operation in three groups
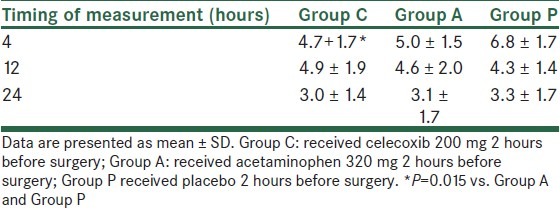
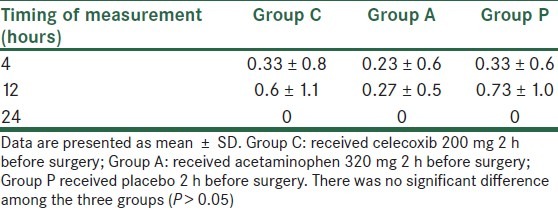
Table 3.
The mean dosage of rescue analgesic at different time intervals after operation in the three groups
Vomiting episodes was no significantly different among the three groups (P>0.05) [Table 4].
Table 4.
The mean of vomiting episodes in the three groups
DISCUSSION
Our study showed that preemptive administration of oral celecoxib 200 mg 2 h before surgery significantly reduced postoperative pain till 4 h compared with preemptive using of oral acetaminophen 320 mg and placebo.
In a randomized, double-blind, placebo-controlled, prospective clinical trial that performed by Al-Sukhun et al.[18] the patients were randomly allocated to receive preemptively oralcelecoxib 200mg, oral ibuprofen 400mg, or a placebo containing lactose 1h before surgery. They showed that celecoxib was better with respect to analgesic effects on all measures of analgesic efficacy (including total pain relief over 8 h, time to onset of effect, peak pain relief, and duration of effect compared with ibuprofen. The pain intensity was significantly lower in the group that received celecoxib compared with pacebo for over 8 h after operation. They also reported no significant adverse effect with using celecoxib when it was used in lower doses for providing analgesia for patients who need minor surgery. In our study, preemptive use of 200 mg oral celecoxib 2 h before surgery has significantly reduced pain intensity till 4 h after surgery compared with placebo. The difference between the results of our study with Al-Sukhun et al. can be due to low sample size of patients enrolled in our study. Moreover, it can be origined from difference in initial state of the patient, difference in the intensity, and quality of the nociceptive stimulus. Control of some of these factors are difficult in clinical studies and may be a reason for the discrepancies between different investigations in this regard.[9–12,14]
In a review performed by Derry and colleagues[23] it was shown that the number needed to treat to benefit (NNT)for celecoxib 200 and 400 mg in comparison with placebo for at least 50% of maximum pain relief over 4–6 h was 4.2 (95% confidence interval (CI) 3.4–5.6) and 2.5 (2.2–2.9), respectively. The median time to use rescue analgesic was 6.6 h with celecoxib 200 mg, 8.4 h with celecoxib 400 mg, and 2.3 h with placebo.The incidence of patients that needed rescue analgesic throughout the 24 h was 74% with celecoxib 200 mg, 63% for celecoxib 400 mg, and 91% for placebo.The NNT to prevent one patient from using rescue analgesic was 4.8 (3.5–7.7) and 3.5 (2.9–4.6) for celecoxib 200 and 400 mg, respectively. Adverse events following use of celecoxib were mild to moderate in severity, and there was no significant difference with the placebo group in proportion of the patients experiencing these complications.
In a review by Toms et al.,[19] concluded that about 50% patients who were treated with a single oral dose of acetaminophen had at least 50%pain relief for over 4–6 h compared with 20% in the placebo group. About 50% patients required additional analgesic for over 4–6 h compared with 70% in the placebo group. No significant adverse effect was recorded. The results of our study is in agreement with Toms et al. study.
It was shown in animal studies that pain causes neuronal sensitization which transmit to brain via dorsal horn neurons.[6,13–17] After neuronal sensitization, endogenous analgesic responses are activated and balance between these processes determine the final response of an individual to the injury.[7,9,12,13]
The surgical trauma may lead to alteration in neuronal sensitization. If analgesics administer before an initial noxious sensitization occurs, it was shown that efficacy of analgesic drugs can be enhanced. This effect is defined as preemptive analgesia.[6–8,13,14]
The efficacy of preemptive analgesia depends on many factors including the nature of tissue injury, the duration of surgery, the type of drug used preemptively, the route and timing of drug administration, duration of its action, the degree of afferent nerve block, and finally emotional, physiological, and psychological condition of the patients.[6–10,12,24]
Our study had some limitations: (1) we didnot find statistical difference in postoperative VAS scores 4-24 h and mean dosage of rescue analgesic used among the three groups. It can be due to low sample size of the enrolled patients. We recommended performing studies with more sample size in future; (2) we evaluated efficacy of preemptive use of only one dose of celecoxib and acetaminophen on postoperative pain. It is recommended that designing more studies with different dosages of both the drugs in future.
CONCLUSION
In conclusion, our study showed that preemptive administration of oral celecoxib 200 mg can control postoperative pain better than preemptive using of oral acetaminophen 320 mg till 4 h after operation in patients who underwent lower extremity orthopedic surgery under general anesthesia.
ACKNOWLEDGMENT
The authors wish to sincerely thank the support of all the colleagues in Alzahra Hospital Medical Center affiliated to Isfahan University of Medical Sciences in Isfahan, Iran. Furthermore, our special thanks to the patients, who wholeheartedly and actively assisted us to carry out this research. No conflict of interest existed. This prospective randomized observational study was approved by the Ethics Committee of our university, (Anesthesiology and Critical Care Research Center, Isfahan University of Medical Sciences, Isfahan, Iran) and all patients gave written, informed consent.
Footnotes
Source of Support: Anesthesiology and Critical Care Research Center, Isfahan University of Medical Sciences, Isfahan, Iran
Conflict of Interest: None declared
REFERENCES
- 1.Brown ST, Kirkpatrick MK, Swanson MS, McKenzie IL. Pain experience of the elderly. Pain Manag Nurs. 2011;12:190–6. doi: 10.1016/j.pmn.2010.05.004. [DOI] [PubMed] [Google Scholar]
- 2.Battisti WP, Katz NP, Weaver AL, Matsumoto AK, Kivitz AJ, Polis AB, et al. Pain management in osteoarthritis: A focus on onset of efficacy-a comparison ofrofecoxib, celecoxib, acetaminophen, and nabumetone across four clinical trials. J Pain. 2004;5:511–20. doi: 10.1016/j.jpain.2004.09.004. [DOI] [PubMed] [Google Scholar]
- 3.Watcha MF, Issioui T, Klein KW, White PF. Costs and effectiveness of rofecoxib, celecoxib, and acetaminophen for preventing pain after ambulatory otolaryngologic surgery. Anesth Analg. 2003;96:987–94. doi: 10.1213/01.ANE.0000053255.93270.31. [DOI] [PubMed] [Google Scholar]
- 4.Wynn RL. New reports on dental analgesics.NSAIDs and cardiovascular effects,celecoxib for dental pain, and a new analgesic--tramadol with acetaminophen. GenDent. 2002;50:218–20. 22. [PubMed] [Google Scholar]
- 5.Kissin I. A call to reassess the clinical value of preventive (preemptive) analgesia. Anesth Analg. 2011;113:977–8. doi: 10.1213/ANE.0b013e31822d39f9. [DOI] [PubMed] [Google Scholar]
- 6.Issioui T, Klein KW, White PF, Watcha MF, Coloma M, Skrivanek GD, et al. The efficacy of premedication with celecoxib and acetaminophen in preventing pain after otolaryngologic surgery. Anesth Analg. 2002;94:1188–93. doi: 10.1097/00000539-200205000-00025. [DOI] [PubMed] [Google Scholar]
- 7.Gimbel JS, Brugger A, Zhao W, Verburg KM, Geis GS. Efficacy and tolerability of celecoxib versus hydrocodone/acetaminophen in the treatment of pain after ambulatory orthopedic surgery in adults. Clin Ther. 2001;23:228–41. doi: 10.1016/s0149-2918(01)80005-9. [DOI] [PubMed] [Google Scholar]
- 8.Gatoulis SC, Voelker M, Fisher M. Assessment of the efficacy and safety profiles of aspirin and acetaminophen with codeine: Results from 2 randomized, controlled trials in individuals with tension-type headache and postoperative dental pain. Clin Ther. 2012;34:138–48. doi: 10.1016/j.clinthera.2011.11.018. [DOI] [PubMed] [Google Scholar]
- 9.Sniezek PJ, Brodland DG, Zitelli JA. A randomized controlled trial comparing acetaminophen, acetaminophen and ibuprofen, and acetaminophen and codeine for postoperative pain relief after Mohs surgery and cutaneous reconstruction. Dermatol Surg. 2011;37:1007–13. doi: 10.1111/j.1524-4725.2011.02022.x. [DOI] [PubMed] [Google Scholar]
- 10.Braun CA. Ibuprofen provides similar pain relief but reduces adverse effects and improves function compared with acetaminophen plus codeine in children with uncomplicated fractures. Evid Based Nurs. 2010;13:10–1. doi: 10.1136/ebn1008-1. [DOI] [PubMed] [Google Scholar]
- 11.Richardson C. NSAIDs similarly effective to acetaminophen plus codeine for post-laparotomy pain and may reduce adverse effects. Evid Based Nurs. 2010;13:4–5. doi: 10.1136/ebn1002-1. [DOI] [PubMed] [Google Scholar]
- 12.Drendel AL, Gorelick MH, Weisman SJ, Lyon R, Brousseau DC, Kim MK. A randomized clinical trial of ibuprofen versus acetaminophen with codeine for acute pediatric arm fracture pain. Ann Emerg Med. 2009;54:553–60. doi: 10.1016/j.annemergmed.2009.06.005. [DOI] [PubMed] [Google Scholar]
- 13.Schachtel BP, McCabe D, Berger M, Zhang R, Sanner KM, Savino L, et al. Efficacy of low-dose celecoxib in patients with acute pain. J Pain. 2011;12:756–63. doi: 10.1016/j.jpain.2010.12.014. [DOI] [PubMed] [Google Scholar]
- 14.Steffens JP, Santos FA, Pilatti GL. The use of etoricoxib and celecoxib for pain prevention after periodontal surgery: a double-masked, parallel-group, placebo-controlled, randomized clinical trial. J Periodontol. 2011;82:1238–44. doi: 10.1902/jop.2011.100682. [DOI] [PubMed] [Google Scholar]
- 15.White PF, Tang J, Wender RH, Zhao M, Time M, Zaentz A, et al. The effects of oral ibuprofen and celecoxib in preventing pain, improving recovery outcomes and patient satisfaction after ambulatory surgery. Anesth Analg. 2011;112:323–9. doi: 10.1213/ANE.0b013e3182025a8a. [DOI] [PubMed] [Google Scholar]
- 16.Boonriong T, Tangtrakulwanich B, Glabglay P, Nimmaanrat S. Comparing etoricoxib and celecoxib for preemptive analgesia for acute postoperative pain in patients undergoing arthroscopic anterior cruciate ligament reconstruction: A randomized controlled trial. BMC Musculoskelet Disord. 2010;11:246. doi: 10.1186/1471-2474-11-246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rezende RM, Paiva-Lima P, Dos Reis WG, Camêlo VM, Bakhle YS, de Francischi JN. Celecoxib induces tolerance in a model of peripheral inflammatory pain in rats. Neuropharmacology. 2010;59:551–7. doi: 10.1016/j.neuropharm.2010.07.022. [DOI] [PubMed] [Google Scholar]
- 18.Al-Sukhun J, Al-Sukhun S, Penttilä H, Ashammakhi N, Al-Sukhun R. Preemptive analgesic effect of low doses of celecoxib is superior to low doses of traditional nonsteroidal anti-inflammatory drugs. J Craniofac Surg. 2012;23:526–9. doi: 10.1097/SCS.0b013e31824cd4fb. [DOI] [PubMed] [Google Scholar]
- 19.Toms L, McQuay HJ, Derry S, Moore RA. Single dose oral paracetamol (acetaminophen) for postoperative pain in adults. Cochrane Database Syst Rev. 2008;4:CD004602. doi: 10.1002/14651858.CD004602.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Davies NM, McLachlan AJ, Day RO, Williams KM. Clinical pharmacokinetics and pharmacodynamics of celecoxib: A selective cyclo-oxygenase-2 inhibitor. ClinPharmacokinetics. 2000;38:225–42. doi: 10.2165/00003088-200038030-00003. [DOI] [PubMed] [Google Scholar]
- 21.Shayiq RM, Roberts DW, Rothstein K, Snawder JE, Benson W, Ma X, et al. Repeat exposure to incremental doses of acetaminophen provides protection against acetaminophen-induced lethality in mice: An explanation for high acetaminophen dosage in humans without hepatic injury. Hepatology. 1999;29:451–63. doi: 10.1002/hep.510290241. [DOI] [PubMed] [Google Scholar]
- 22.Aldrete JA. The post-anesthesia recovery score revisited. J Clin Anesth. 1995;7:89–91. doi: 10.1016/0952-8180(94)00001-k. [DOI] [PubMed] [Google Scholar]
- 23.Derry S, Moore RA. Single dose oral celecoxib for acute postoperative pain inadults. Cochrane Database Syst Rev. 2012;3:CD004233. doi: 10.1002/14651858.CD004233.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Lau WK, Lau YM, Zhang HQ, Wong SC, Bian ZX. Electroacupuncture versus celecoxib for neuropathic pain in rat SNL model. Neuroscience. 2010;170:655–61. doi: 10.1016/j.neuroscience.2010.07.031. [DOI] [PubMed] [Google Scholar]