

Abstract
Abdominal cocoon is a rare cause of intestinal obstruction. It is difficult to diagnose in most of the cases preoperatively. Surgical removal of the membrane resulted in complete recovery in the majority of the cases. The exact etiology of abdominal cocoon is still unknown. We reported a male patient who presented with features of intestinal obstruction and has been diagnosed as abdominal cocoon intraoperatively.
1. Introduction
Abdominal cocoon is a rare condition that refers to total or partial encapsulation of the small bowel by a fibrocollagenous membrane or cocoon with local inflammatory infiltrate leading to acute or chronic bowel obstruction [1]. The condition has been described with various names including “peritonitis chronica fibrosa incapsulata” by Owtschinnikow in 1907 [2]. Abdominal cocoon is predominantly reported among females from the tropical and subtropical regions. However, adult males were also reported to represent cases of abdominal cocoon [1, 3–5]. Herein, we present a case with this condition that we believe to be the first one reported in Qatar.
2. Case Report
A 41-year-old male patient was admitted to the general surgery department of our hospital, complaining of abdominal pain, nausea, and vomiting. He had clinical history of several attacks of abdominal pain over the last seven months. He is a known case of eczema and was on local steroids since four years. The patient had no history of previous abdominal operation. On physical examination, a soft, nontender, and mobile mass was palpated in the right half of the abdomen. No hepatomegaly or splenomegaly was observed. Bowel sounds were a bit hyperactive, and rectal examination was normal. There was no abnormality in the complete blood count and blood chemistry.
CT abdomen revealed multiple clumped small bowel loops in the lower abdomen on the right side with no passage of oral contrast. The adherent bowel loops showed wall enhancement with contrast (Figure 1).
Figure 1.

CT showing membrane enveloping loops of small bowel.
The patient underwent emergency explorative laparotomy. The entire small bowel was found to be encased in a cocoon-like fibrous membrane which extended laterally to involve ascending and descending colon (Figure 2). A 2 cm diverticulum was seen in the terminal ileum. Other organs were normal. Lysis of the membrane was carried out, and loops were separated by dissection. The freed small bowel segments were viable, and excision of the diverticulum was done.
Figure 2.
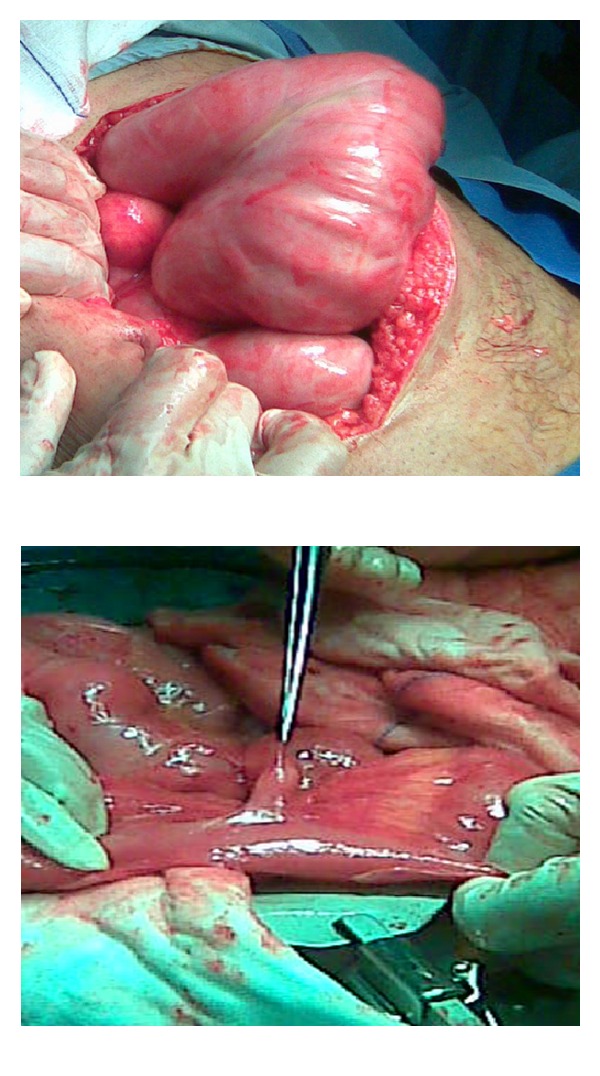
Intraoperative photograph shows the encapsulated small bowel with a dense fibrous layer.
Intraoperative findings showed encapsulation of small bowel by a dense whitish membrane as a cocoon, which was excised and adhesiolysis was done to release the loops of the intestine. The histological examination of the membrane revealed fibrous tissue focally lined by flatted mesothelial cells with scattered mononuclear inflammatory cell infiltrate and tissue culture fibroblasts. The patient showed a significant recovery postoperatively and was discharged from the hospital uneventfully.
3. Discussion
The preoperative diagnosis of abdominal cocoon is difficult and hence, the diagnosis is usually confirmed by laparotomy. The signs and symptoms of abdominal cocoon are usually nonspecific [6, 13, 14] including vomiting, abdominal pain and distention. The signs comprise soft abdomen with the presence of palpable nontender mass. In our case, the patient gave also history of recurrent episodes of abdominal pain over the last seven months, and he denied any history of previous abdominal operation.
Abdominal cocoon could be classified as primary (idiopathic) or secondary [14]. Table 1 shows a review of the literature for abdominal cocoon [3, 6–12].
Table 1.
Review of the literature for abdominal cocoon.
| Authors | Year | Age and gender | Country | Clinical association |
|---|---|---|---|---|
| Devay et al. [3] | 2006 | 30-year male | Turkey | Acute appendicitis |
| She et al. [6] | 2012 | 47-year woman | Hong Kong | Peritoneal dialysis |
| Sarmast et al. [7] | 2012 | 30-year male | India | Tuberculosis |
| Serter et al. [8] | 2012 | Turkey | ||
| Chatura and Nayak [9] | 2012 | 14-year girl | Indian | Tuberculosis |
| Kayastha and Mirza [10] | 2012 | 13-year girl | Pakistan | Suspected Acute appendicitis |
| Noormohamed and Kadi [11] | 2012 | N/A | UK | Peritoneal dialysis |
| Hur et al. [12] | 2004 | 34-year woman 47-year man |
South Korea | Unknown |
| This paper | 2012 | 41-year male | Qatar | Unknown |
The causative factor for primary form remains unknown, which might be caused by a subclinical peritonitis leading to the formation of a cocoon [15]. On the other hand, placement of LeVeen shunt for refractory ascites, continuous ambulatory peritoneal dialysis, tuberculosis, systemic lupus erythematosus, and the use of povidone iodine for abdominal washout as well as the beta-adrenergic blocker (practolol) are identified as secondary causes of abdominal cocoon [9]. Prevalence of sclerosing peritonitis among subjects under peritoneal dialysis is reported to be 0.7%, and the mortality rate varies from 56% to 93% despite various therapeutic modalities [11].
It is challenging to diagnose abdominal cocoon preoperatively, as these patients usually presented with normal biochemical investigations and imaging findings apart from CT and MRI are nonspecific [4]. Hence, often diagnosis is confirmed by laparotomy. It has been suggested that two clinical signs may be elicited. Firstly, in view of the dense fibrous sac, only bowel proximal to and out of the fibrous layer can distend and the patient may have a fixed, asymmetrical distension of the abdomen that does not vary with peristalsis. In addition, the patient would have a difference in consistency of the abdominal wall to palpation. This is because the distended area is soft and the flat area, which is covered by the dense fibrous capsule, is firm. In our patient, the entire small bowel was encased. Recurrent acute or chronic small bowel obstruction with increased compression of the encased intestine that causes abdominal pain has been reported in the majority of patients with abdominal cocoon syndrome [15, 16]. Clinical presentation also includes a palpable abdominal mass that resulted from encapsulated cluster of dilated small bowel loops.
CT findings are consistent in diagnosing abdominal cocoon [16]. CT abdomen in our case also revealed multiple clumped small bowel loops in the lower abdomen and the adherent bowel loops showed wall enhancement with the use of contrast. However, intraoperative and histopathology findings are usually considered for final diagnosis of abdominal cocoon, as most patients underwent surgical intervention without imaging [17].
Encasement of the whole or part of the small bowel in a thick shiny membrane is a characteristic finding of abdominal cocoon [3]. In the present case, the entire small bowel was encased in a cocoon-like fibrous membrane which extended laterally to involve ascending and descending colon. Surgical management of abdominal cocoon is usually done by careful dissection and excision of the thick sac with the release of the small intestine. We also performed surgical removal of the membrane which leads to complete recovery.
In conclusion, abdominal cocoon is a rare cause of small bowel obstruction. The preoperative diagnosis requires a high index of suspicion, supported by clinical data and imaging findings indicative of the condition. However, most cases are diagnosed at exploratory laparotomy.
Acknowledgments
The authors thank all the general surgery staff for their cooperation. The authors have no conflict of interest and no financial issues to disclose. All the authors read and approved the paper.
References
- 1.Kirshtein B, Mizrahi S, Sinelnikov I, Lantsberg L. Abdominal cocoon as a rare cause of small bowel obstruction in an elderly man: report of a case and review of the literature. Indian Journal of Surgery. 2011;73(1):73–75. doi: 10.1007/s12262-010-0200-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Owtschinnikow PJ. Peritonitis chronica fibrosa incapsulata. Archiv für Klinische Chirurgie. 1907;83:623–634. [Google Scholar]
- 3.Devay AO, Gomceli I, Korukluoglu B, Kusdemir A. An unusual and difficult diagnosis of intestinal obstruction: the abdominal cocoon. Case report and review of the literature. World Journal of Emergency Surgery. 2006;1(1, article 8) doi: 10.1186/1749-7922-1-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Altinli E, Sumer A, Celik A. Abdominal cocoon: a rare cause of intestinal obstruction. Israeli Journal of Emergency Medicine. 2007;7(3):42–44. [Google Scholar]
- 5.Chew MH, Sophian Hadi I, Chan G, Ong HS, Wong WK. A problem encapsulated: the rare peritoneal encapsulation syndrome. Singapore Medical Journal. 2006;47(9):808–810. [PubMed] [Google Scholar]
- 6.She HL, Ip PP, Cheung SC. Abdominal cocoon: uncommon cause of intestinal obstruction in peritoneal dialysis patient. Hong Kong Medical Journal. 2012;18(6)539.e1-2 [PubMed] [Google Scholar]
- 7.Sarmast AH, Showkat HI, Sherwani A, Kachroo MY, Parray FQ. Abdominal tuberculosis with a cocoon. Iranian Red Crescent Medical Journal. 2012;14(8):503–504. [PMC free article] [PubMed] [Google Scholar]
- 8.Serter A, Kocakoç E, Cipe G. Supposed to be rare cause of intestinal obstruction; abdominal cocoon: report of two cases. Clinical Imaging. 2012 doi: 10.1016/j.clinimag.2012.08.010. [DOI] [PubMed] [Google Scholar]
- 9.Chatura RK, Nayak VJ. Abdominal cocoon: case report of a rare cause of intestinal obstruction. Indian Journal of Pathology and Microbiology. 2012;55(3):379–380. doi: 10.4103/0377-4929.101751. [DOI] [PubMed] [Google Scholar]
- 10.Kayastha K, Mirza B. Abdominal cocoon simulating acute appendicitis. APSP Journal of Case Reports. 2012;3(1, article 8) [PMC free article] [PubMed] [Google Scholar]
- 11.Noormohamed MS, Kadi N. Abdominal cocoon in peritoneal dialysis—a fatal outcome. BMJ Case Reports. 2012 doi: 10.1136/bcr.01.2012.5581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hur J, Kim KW, Park MS, Yu JS. Abdominal cocoon: preoperative diagnostic clues from radiologic imaging with pathologic correlation. American Journal of Roentgenology. 2004;182(3):639–641. doi: 10.2214/ajr.182.3.1820639. [DOI] [PubMed] [Google Scholar]
- 13.Hamaloglu E, Altun H, Ozdemir A, Ozenc A. The abdominal cocoon: a case report. Digestive Surgery. 2002;19(5):422–424. doi: 10.1159/000065827. [DOI] [PubMed] [Google Scholar]
- 14.Deeb LS, Mourad FH, El-Zein YR, Uthman SM. Abdominal cocoon in a man: preoperative diagnosis and literature review. Journal of Clinical Gastroenterology. 1998;26(2):148–150. doi: 10.1097/00004836-199803000-00013. [DOI] [PubMed] [Google Scholar]
- 15.Foo KT, Ng KC, Rauff A. Unusual small intestinal obstruction in adolescent girls: the abdominal cocoon. British Journal of Surgery. 1978;65(6):427–430. doi: 10.1002/bjs.1800650617. [DOI] [PubMed] [Google Scholar]
- 16.Ranganathan S, Abdullah BJJ, Sivanesaratnam V. Abdominal cocoon syndrome. Journal of the Hong Kong College of Radiologists. 2003;6(4):201–203. [Google Scholar]
- 17.Kumar M, Deb M, Parshad R. Abdominal cocoon: report of a case. Surgery Today. 2000;30(10):950–953. doi: 10.1007/s005950070053. [DOI] [PubMed] [Google Scholar]