

Abstract
Intraoral dermoid and epidermoid cysts are rare and account for less than 0.01% of all the cysts in the oral cavity. A large majority of the same arise in the floor of the mouth and infrequently in other sites. These cysts often remain asymptomatic for years until they reach a size that interferes with mastication, speech and rarely, breathing. However, they also can become acutely symptomatic if they are secondarily infected. We would like to report a case of a rare epidermoid cyst in the buccal mucosa with its differential diagnosis and a review of literature.
Keywords: Cysts, Epidermoid, Dermoid, Oral cavity, Buccal mucosa
Introduction
Dermoid, epidermoid and teratoid cysts can be found anywhere in the body, particularly in areas where embryonic elements fuse together. Most cases are congenital and have been reported in the ovaries, the testicles, as well as the hands and feet. Dermoid and epidermoid cysts in the mouth are uncommon and account for less than 0.01% of all the cysts [1, 2]. Dermoid cysts are lined by epidermis and contain skin adnexa such as sebaceous glands, sweat glands and hair follicles. When there are no adnexa, these cysts are termed as epidermoid or epidermal with the lining containing only epithelium. Epidermoid cysts are also known by a number of other names, including follicular cysts, epidermal inclusion cysts and wen [3]. Teratoid cysts consist of dermoid material plus tissue of other embryonal sources like respiratory, gastrointestinal and connective tissues such as bundles of striated muscle and distinct areas of fat [1].
Epidermoid cysts can be acquired or posttraumatic. The posttraumatic cysts are also called as implantation keratinizing epidermoid cysts [4] and are always the result of previous trauma at the site which may have driven epithelial cells into the dermis. The large majority of cases arise in the floor of the mouth and rarely in other sites [2].
We present in this case report an exceptionally atypical existence of an epidermoid cyst in the buccal mucosa.
Case Report
A 25-year-old man reported to our department with a chief complaint of swelling in the left buccal mucosa for the last 2 years, which was accidentally noticed. Intraoral and extraoral examination revealed a 1.5 × 1.5 × 1.5 cm swelling extending from the left commissure along the occlusal plane up to first premolar region (Fig. 1). On palpation, the swelling was non tender and freely mobile. Intraorally, the overlying mucosa was normal and extraorally, the skin overlying the swelling did not show any induration. There was no associated lymphadenopathy. A detailed case history of the patient provided no association of cheek biting with the lesion. The dental examination also revealed no relevant findings. An ultrasonography (Fig. 2) of that region presented with a small, hypodense, compressible and non vascularised lesion suggestive of a cyst present behind the commissure just below the buccal mucosa and anterior to the buccinator muscle. Excisional biopsy of the lesion was planned to confirm the diagnosis.
Fig. 1.

Preoperative extraoral photograph
Fig. 2.

Ultrasonograph of the lesion
Enucleation of the cyst was done under general anaesthesia by giving a horizontal incision in the buccal mucosa (Fig. 3). The cyst was found immediately underlying the buccal mucosa. Careful dissection was carried out and the cyst enucleated (Fig. 4). Primary closure was obtained with a synthetic absorbable suture (Coated polyglactin 910 violet, Vicryl, Johnson & Johnson) material and the specimen was sent for histopathological examination.
Fig. 3.

Intra operative
Fig. 4.
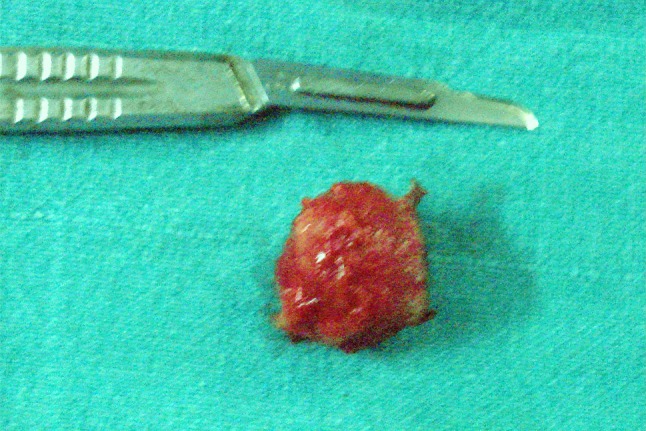
Gross specimen
Histopathology revealed a cystic cavity filled with keratin flakes. The lining of the cyst showed hyperorthokeratinized stratified squamous epithelium with prominent stratum granulosum. At places the surface was corrugated. The connective tissue was scanty and showed few blood vessels and chronic inflammatory cells (Figs. 5, 6). Overall features were suggestive of epidermoid cyst. The patient was kept on regular follow up for a period of 2 years with no signs of recurrence.
Fig. 5.

Histopathology of the lesion
Fig. 6.
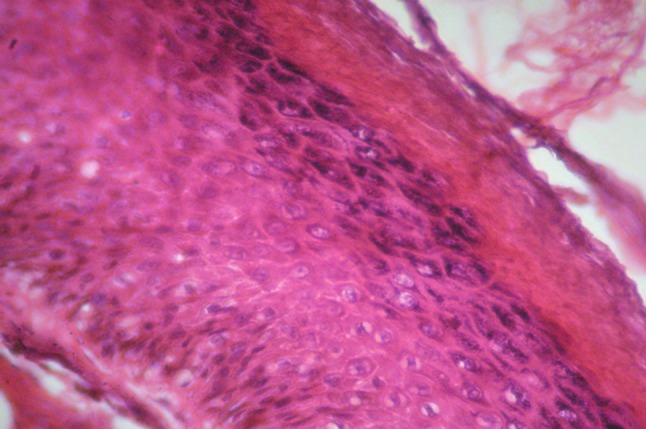
Histopathology showing the cystic lining under magnification (400×)
Discussion
Dermoid and epidermoid cysts may be present at birth and also in old patients, with the majority occurring between the ages of 15 and 35 years. New and Erich [5] in a review of 1,495 cases of Dermoid cysts found only 6.9% (103) of cases involving head and neck out of which only 1.6% (24) cases involved oral cavity. Most of the reported cases were located in the sublingual region, usually in the midline. However, occasionally such lesions are also found on the tongue, lips, and intraosseously [6–8]. Implantation keratinizing epidermoid cysts may occur in other parts of the oral cavity other than the floor of the mouth as a result of trauma [4]. However, for the cysts to form, a proper combination of events, namely; (a) trauma (b) an epithelial system capable of proliferation at that moment, and (c) minimal inflammation are required. This cascade of events occurring simultaneously is exceedingly uncommon and probably explains the rarity of these cases. Posttraumatic cysts are usually symptomless and may not be associated in the patient’s mind with any specific injury, such injury possibly having occurred many years earlier, as was also noted in our case.
Schneider et al. [9] in 1978 reported the first case of epidermoid cyst of the buccal mucosa. Rajayogeswaran et al. [1] in 1989 reported a large epidermoid cyst within the buccal mucosa. Recently, Fatih Ozan et al. [10] in 2007 have reported a case of epidermoid cyst of buccal mucosa in a 38-year-old female. They all have presented rare examples of a typical epidermoid cyst of the buccal mucosa with findings closely resembling our case.
The differential diagnosis should include a broad variety of conditions which can be classified as developmental, neoplastic and infectious processes. Infectious processes like swellings on the face which are odontogenic in origin, buccal space infections and massetric space infections can be ruled out in our case as the associated clinical symptoms were absent. Neoplastic conditions can also be excluded due to the benign appearance of the lesion and lack of nodal involvement. Other benign swellings to be considered are: lipoid, salivary, and vascular lesions. Careful physical examination and investigative procedures like Fine needle aspiration cytology and ultrasonography performed helped us rule out these conditions.
In the developmental category an oral lymphoepithelial cyst can be considered. However, this cyst is usually associated with or adjacent to the Waldeyer’s ring, is lesser than 1 cm in dimension and is characteristically a smooth, whitish yellow, firm and painless mass. Absence of these positive findings helped us to rule out the lymphoepithelial cyst in our case. Epivatianos et al. [11] have reported a case with a coexistence of lymphoepithelial and epidermoid cysts on the floor of the mouth. Gutmann and co-workers [12] have also reported a case of an intradermal nevus associated with epidermoid cyst in the mucous membrane of the cheek.
Dermoid and epidermoid cysts often remain asymptomatic for years until they reach a size that interferes with mastication, speech and very rarely breathing. However, they also can become acutely symptomatic, if they are secondarily infected. Cortezzi et al. [13] in 1994 reported an epidermoid cyst of the floor of the mouth that reached a huge proportion and caused a life threatening situation because of secondary infection. Ikeda et al. [14] described a patient with basal cell carcinoma arising from the walls of an epidermoid cyst. Lopez-Rios et al. [15] described a patient with squamous cell carcinoma arising in the wall of an otherwise conventional epidermoid cyst. Devine et al. [16] reported a carcinomatous transformation of a sublingual dermoid cyst. Most patients have only one or few epidermoid cysts, however in Gardner’s syndrome, numerous epidermoid cysts occur, especially on the face and scalp [17].
To summarize, the diagnosis of dermoid or epidermoid cysts should be reached only after ruling out various developmental, neoplastic, infectious and traumatic lesions. If ever a malignancy is confirmed, appropriate evaluation for a primary needs to be carried out followed by the definitive management. The epidermoid cysts are best treated by enucleation after histopathological confirmation of the diagnosis.
References
- 1.Rajayogeswaran V, Eveson JW. Epidermoid cyst of the buccal mucosa. Oral Surg Oral Med Oral Pathol. 1989;67:181–184. doi: 10.1016/0030-4220(89)90326-5. [DOI] [PubMed] [Google Scholar]
- 2.Worley CM, Laskin DM. Coincidental sublingual and sub mental epidermoid cysts. J Oral Maxillofac Surg. 1993;51:787–790. doi: 10.1016/S0278-2391(10)80424-0. [DOI] [PubMed] [Google Scholar]
- 3.Shear M. Cysts of the oral regions. 2. Bristol: Wright PSG; 1983. p. 104. [Google Scholar]
- 4.Ettinger RL, Manderson RD. Implantation keratinizing epidermoid cysts. Oral Surg. 1973;26:225–230. doi: 10.1016/0030-4220(73)90242-9. [DOI] [PubMed] [Google Scholar]
- 5.New GB, Erich JB. Dermoid cysts of head and neck. Surg Gynecol Obstet. 1937;65:48–55. [Google Scholar]
- 6.Valtonen H, Nuutinen J, Karja T, Collan Y. Congenital dermoid cysts of the tongue. J Laryngol Otol. 1986;100:965. doi: 10.1017/S0022215100100416. [DOI] [PubMed] [Google Scholar]
- 7.Flom GS, Donovan TJ, Landgraf JR. Congenital dermoid cyst of the anterior tongue. Otolaryngol Head Neck Surg. 1989;101:8. doi: 10.1177/019459988910100313. [DOI] [PubMed] [Google Scholar]
- 8.Mathur SK, Menon PRN. Dermoid cyst of the tongue. Report of a case. Oral Surg Oral Med Oral Pathol. 1980;50:217–218. doi: 10.1016/0030-4220(80)90371-0. [DOI] [PubMed] [Google Scholar]
- 9.Schneider LC, Mesa ML. Epidermoid cysts of the buccal mucosa. Q Natl Dent Assoc. 1978;36:39–42. [PubMed] [Google Scholar]
- 10.Ozan F, Polat HB, Sinan Ay, Goze F. Epidermoid cyst of buccal mucosa. J Contemp Dent Pract. 2007;8:90–96. [PubMed] [Google Scholar]
- 11.Epivationos A, Zaraboukos T, Antoniades D. Coexistance of lymphoepithelial and epidermoid cysts on the floor of the mouth: report of a case. Oral Dis. 2005;11:330–333. doi: 10.1111/j.1601-0825.2005.01121.x. [DOI] [PubMed] [Google Scholar]
- 12.Gutmann J, Cifuentes C, Gandulfo P, Guesalaga F. Intradermal nevus associated with epidermoid cysts in the cheek. Oral Surg Oral Med Oral Pathol. 1978;45:76–82. doi: 10.1016/0030-4220(78)90226-8. [DOI] [PubMed] [Google Scholar]
- 13.Cortezzi W, De Albuquerque EB. Secondarily infected epidermoid cyst in the floor of the mouth causing a life-threatening situation: report of a case. J Oral Maxillofac Surg. 1994;52:762–764. doi: 10.1016/0278-2391(94)90496-0. [DOI] [PubMed] [Google Scholar]
- 14.Ikeda I, Ono T. Basal cell carcinoma originating from an epidermoid cyst. J Dermatol. 1990;17:643–646. doi: 10.1111/j.1346-8138.1990.tb01709.x. [DOI] [PubMed] [Google Scholar]
- 15.Lopez-Rios F, Rodriguez-Peralto JL, Castano E, Benito A. Squamous cell carcinoma arising in a cutaneous epidermal cyst: case report and literature review. Am J Dermatopathol. 1999;21:174–177. doi: 10.1097/00000372-199904000-00012. [DOI] [PubMed] [Google Scholar]
- 16.Devine JC, Jones DC. Carcinomatous transformation of a sublingual dermoid cyst-a case report. Int J Oral Maxillofac Surg. 2000;29:126–127. doi: 10.1016/S0901-5027(00)80009-0. [DOI] [PubMed] [Google Scholar]
- 17.Shafer WG, Hine MK, Levy BM. A textbook of oral pathology. 4. Philadelphia: WB Saunders; 1983. pp. 78–79. [Google Scholar]