

Abstract
Background:
Multiple sclerosis (MS) is a chronic and progressive disease of the central nervous system with debilitating symptoms and complications. Therefore, education and appropriate interventions, including self-care education, are necessary to increase the quality of life in these patients. The purpose of this study was to determine the influence of self-care education on quality of life in MS patients affiliated to Iranian MS Association.
Materials and Methods:
This quasi-experimental study assessed a single group of MS patients before and after training. Totally, 50 MS patients were selected non-randomly from the patients referring to Iranian MS Association. A two-part questionnaire was used to collect data. The first part included demographic information and the second part consisted of a quality of life questionnaire (MSQOL-54) including 54 items in 3 sections and 14 subgroups. The scores ranges from zero to a hundred in each subgroup. The reliability of the questionnaire has been confirmed (Cronbach's alpha = 0.96). The questionnaires were filled out by the patients before training. After at least six 50-minute training sessions during three months, the same questionnaire was again completed by the participants. Statistical analyses, including absolute and relative frequency tables and mean and standard deviation for descriptive analysis, and t-test and Pearson correlation for descriptive analysis, were performed by SPSS.
Findings:
The mean values of quality of life in physical health, pain, fatigue, health conception, changes in health status, sexual activities, as well as overall quality of life scores differed significantly after training. Moreover, except for cognitive activity, there were significant differences in values of mental health before and after training.
Conclusions:
Designing and applying the self-care programs based on the educational needs of MS patients has a positive effect on physical and psychological aspects of their quality of life.
Keywords: Multiple sclerosis, self-care, patient education, quality of life
INTRODUCTION
Multiple sclerosis (MS) is the most common disabling disease of young adults. It occurs due to the inflammatory process of demineralization of the central nervous system.[1] It is the third most common cause of disability among 20 to 40 year-old people[2,3] with two and a half million people worldwide suffering from the disease. There are about forty thousand MS patients in Iran. Currently there are 12 thousand people who have cases in the Iranian MS Society. The prevalence of MS has been reported as approximately 20 people in every hundred thousand people in Iran.[4] This disease will affect all aspects of the patients’ life, including physical ability, emotional and psychological status, employment, family life, social activities and finally the quality of life.[5] MS, as a chronic disease, makes adverse effects on the quality of life. In addition, disability, pain and suffering will impose direct and indirect costs to the society,[2,6] which in turn affects the ability of the patient to perform self-care.[7] Lack of awareness and self-care deficit are among the reasons leading to frequent hospitalizations of MS patients. Thus, self-care training has an important role since it will prevent frequent hospitalizations, reduce frustration and increase confidence in MS patients.[8,9] For such training should focus on training the patients’ physical, emotional, psychological, social and economical needs. Main goals of care, such as controlling the disease, improving personal performance and reducing side effects,[10–12] should be determined in self-care training. Considering the significant impacts the abovementioned problems have on the quality of life among patients with MS, the present study has been conducted to determine the effects of self-care training on the quality of life in patients with MS.
MATERIALS AND METHODS
The present quas i-experimental study evaluated a single group of 53 MS patients before and after an intervention. Due to the limited number of patients satisfying the inclusion criteria, the subjects were not selected randomly. The inclusion criteria were membership in the Iranian MS Society, aging between 20 and 50 years, willingness to participate in the study, confirming the existence of the disease by the physician, not having psychological diseases, no severe physical symptoms, not having drug addiction, and not participating in training sessions of the MS Society. The data was collected using a two-part questionnaire. The first part was about the demographic characteristics of the patients and involved age, gender, education level, marital status, duration of illness and type of MS. The second part consisted of the quality of life questionnaire (MSQOL-54) including 54 questions in 3 sections and 14 subgroups. Three main sections of the questionnaire were physical quality of life, psychological quality of life and overall quality of life. Each subgroup could be scored between zero and one hundred. The questionnaire was translated, standardized and has been used for several times. The reliability of the questionnaire was approved by a Cronbach's alpha coefficient of 0.96.
The 3-month training program involved at least six 50-minute training sessions. During the sessions, simple questions regarding underlying diseases and their causes, self-care skills in mobility, skills in reducing physical symptoms (fatigue, sexual satisfaction, and improving nutrition), and skills in reducing emotional and psychological symptoms were answered. In addition, training pamphlets on all physical, emotional, psychological and social aspects of MS were distributed. The researchers called and followed the subjects each month. The patients were re-evaluated with the same questionnaire, 45 days after the last training session. Due to mental health problems and lack of cooperation, 3 patients were excluded from the research and the study was continued with the remaining 50. Data analyses were performed by SPSS. Absolute and relative frequency tables, mean and standard deviation were used for descriptive analysis, while t-test and Pearson correlation coefficient were used for inferential statistics.
FINDINGS
This study evaluated 50 patients in two stages, before and after training. Demographic data showed 62% of the subjects were single and 38% married. Most participants aged 20 to 30 years and had at least a high school diploma. The disease was present for 1 to 5 years in 50% of the subjects and for over 5 years among the others. The t-test results showed significant differences in physical quality of life and overall quality of life scores (p < 0.05) in the following areas: physical health, pain, fatigue, perceived health and changes in health and marital satisfaction. The quality of life scores increased after the intervention in all cases. There was not a statistically significant difference (between before and after training) in the areas of energy changing and the ability to improve work and social activities (p > 0.05) (Table 1). Except for cognitive activity (p = 0.001), there were statistically significant differences in emotional and psychological health after the training. The most and least changes in the psychological aspects of quality of life were attributable to total mental health scores (p < 0.001) and mental health (p < 0.04), respectively. The most and least changes in physical aspects of quality of life were observed in physical health (0.32), (p < 0.004) and pain and energy fields (0.02) (p > 0.05), respectively (Table 2). It is noteworthy that self-care training involved and improved all domains of quality of life. The differences were significant in both physical and mental domains and the overall quality of life scores (p < 0.001). In the emotional and psychological domains, there were statistically significant relations between gender and emotional and psychological reasons to do things, as well as between quality of life in patient's perspective and marital status and education (p < 0.05). There was a significant correlation between the quality of life in the patient's perspective and the recurrence of the disease (p < 0.05). In addition, in physical aspects, the study findings showed significant correlations between marital status and social activities and also between education and the two areas of physical quality of life sexual activity (p = 0.04) and perceived health (p = 0.03) (p < 0.05). Spearman correlation test revealed a linear relationship between duration of the disease and the variables of cognitive activity (r = 0.27) and a feeling of well-being (r = 0.21). The results of Spearman correlation test also indicated an inverse linear relationship between age and the physical health variables (r = - 0.68), perceived health (r = -0.43) and overall physical health (r = -0.039).
Table 1.
Evaluating of the physical domain of quality of life among the participants before and after training
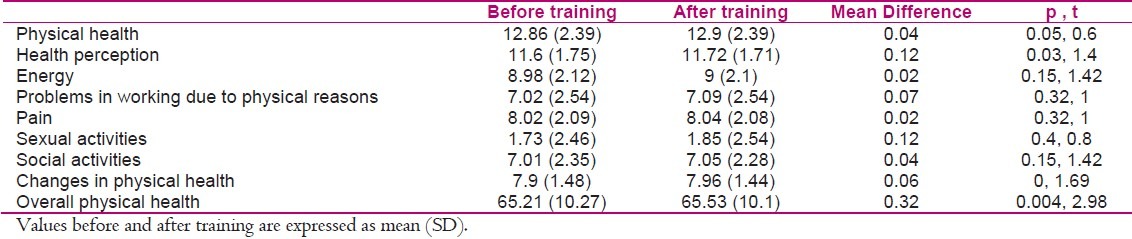
Table 2.
Evaluating the in emotional and psychological domains of quality of life among the participants before and after training

DISCUSSION
Based on our results, quality of life after the training improved in most domains. There was a statistically significant difference in overall physical health (p = 0.004) which shows the efficiency of the training program in this field. Similarly, Montel and Bungener studied 135 patients with MS in France in 2007 and found a significant difference in overall physical health after training (p = 0.002).[11] Twork et al. performed a study entitled “Living conditions, quality of life and adjustment in patients with MS” and suggested training as effective on physical health improvement (p = 0.003).[13]
In the present study, a statistically significant difference was seen in the values of health perception before and after the training (p = 0.03) which can indicate the training to be effective on improving health perception. Likewise, Twork et al. performed a study in 2008 in Hungary and obtained the same result as we did (p = 0.001).[13]
A previous study did not find a significant difference between energy levels and improvement in ability to work before and after training (p = 0.15).[14] Similarly, Solari and Radice did not observe a statistically significant improvement in energy levels or problems in working due to physical reasons as a result of training (p = 0.32).[15] Our results indicated that no statistically significant improvement has been obtained in social activities after training (p = 0.15). Ennis et al. conducted a survey in 2008 and reported the same results (p = 0.22).[16]
We observed a statistically significant difference in the physical area after training (p = 0.001). Training was also found to improve physical health. On the contrary, Twork et al. suggested training not to be effective on physical health and its improvement (p > 0.05).[13]
Our results indicated a statistically significant change in overall psychological health after training (p = 0.001). Likewise, Montel and Bungener reported training as effective on improving the overall emotional health.[11] In addition, our findings suggested training to cause a significant change in the field of problems in working due to emotional and psychological reasons (p = 0.003). However, Twork et al. did not find a significant difference in the field of cognitive activity.[13] Moreover, Samgelaji et al. studied the effects of rehabilitation services on the quality of life among people with MS and reported similar results (p > 0.05).[17]
The present study revealed training to be effective on well-being and quality of life from the patient's perspective (p = 0.001), i.e. a significant difference was seen after the training. However, Solari and Radice concluded that training had no effects on quality of life from the patient's perspective (p > 0.05).[15]
We also found a significant relationship between gender and problems in working due to emotional and psychological reasons (p = 0.05), i.e. higher averages in this area were observed among females and therefore, problems in working due to emotional and psychological reasons declined in women after training. In addition, statistically significant relationships existed between marital status and social activities in the physical area (p = 0.05). In fact, the average in single people was higher than married people which means the social activities of single people were higher after training. There was also a statistically significant relationship between marital status and quality of life from the patient's perspective in the emotional and psychological field (p = 0.002). Due to the higher average, we concluded that training married subjects improved the quality of life from the patient's perspective (p > 0.05). In contrast, Pekmezovic showed that there was no significant relationship between marital status and quality of life (p > 0.05).[19]
The results of this study indicated a significant relationship between education and the two areas of physical quality of life, namely sexual activity (p = 0.001) and perception of health (p = 0.03). There were also significant relationships between education and quality of life from the patient's perspective in the emotional area (p = 0.001), i.e. the average score was more in people with an education level above high school diploma. Thus, training could improve the mentioned areas more in people with higher education. Similarly, Zohrevand suggested training as more effective in people with college degrees.[18]
According to our findings, there was a significant correlation among a number of areas of physical quality of life and the duration of the disease. Spearman correlation test showed inverse linear relationships between the duration of the disease and the variables of physical health (r = 0.04), sexual activities (r = 0.36), social activities (r = 0.05), overall health (r = 0.11), cognitive activities (r = -0.27), and feeling of well-being (r = -0.21). In other words, the value of the variables reduced as the duration of MS increased. There was a direct linear relationship between problems in working due to physical reasons (r = 0.22) and disease duration, i.e. patients with longer periods of MS had increased problems in working due to physical reasons. However, Pekmezovic did not find significant correlation coefficients between disease duration, gender, and marital status (p > 0.05).[19] This contrast might be related to the fact that patients in the study of Pekmezovic enjoyed higher levels of social and economic support than our patients did.
Spearman correlation test revealed an inverse linear relationship between quality of life from patient's perspective (r = 0.2) and number of disease recurrences. Therefore, quality of life from patient's perspective reduced as the frequency of disease recurrence increased. Somers also found that patients with higher recurrence rates had a lower quality of life.[20]
Moreover, Spearman correlation test showed inverse linear relationships between age and physical health (r = 0.68), perception of health (r = 0.43) and overall physical health (r = 0.039). As a result, higher ages were associated with lower physical health, perception of health and overall physical health. Likewise, Patti et al. reported a linear relationship between age and overall physical health.[21] According to the findings of this study, and considering the impact of MS on physical, emotional and psychological aspects of life among patients, their quality of life can be promoted through proper training. We found self-care training to be effective on physical, emotional and psychological domains of quality of life in patients with MS. Therefore, educational planners in the various health centers and the authorities of MS Society are recommended to consider trainings in order to enhance the quality of life among these patients. Trainings would make MS patients feel good and be more efficient. An independent self-care program is particularly important since it is a non-pharmacological, noninvasive, and inexpensive method in controlling physical and psychological problems associated with MS.
ACKNOWLEDGMENT
The authors express their thanks and appreciation to the members and authorities of the Iranian MS Society
Footnotes
Source of Support: Iranian MS Society
Conflict of Interest: None declared
REFERENCES
- 1.Fauci AS, Eugene B, Hauser SL, Longo DL, Loscalzo Joseph JL. Harrison's principles of internal medicine. 17th ed. New York: McGraw-Hill; 2008. pp. 375–7. [Google Scholar]
- 2.Smeltzer SC. Textbook of Medical-Surgical Nursing. 9th ed. Philadelphia: Lippincott Williams & Wilkins; 2008. [Google Scholar]
- 3.Soltan Zadeh A. Principle of Neurology. 2nd ed. Tehran: Jafari Publication; 2004. pp. 215–7. [Google Scholar]
- 4.Ropper AH, Adams RD, Samuels MA, Victor M. 7th ed. New York: McGraw-Hill Prof Med/Tech; 2005. Adams and Victor's principles of neurology; pp. 954–83. [Google Scholar]
- 5.Draper P. Nursing perspectives on quality of life. 1st ed. London: Routledge; 1997. [Google Scholar]
- 6.Mathiowetz V, Matuska KM, Murphy ME. Efficacy of an energy conservation course for persons with multiple sclerosis. Arch Phys Med Rehabil. 2001;82(4):449–56. doi: 10.1053/apmr.2001.22192. [DOI] [PubMed] [Google Scholar]
- 7.Simpson RL. Developing IT relief for chronic illness. Nurs Manage. 2000;31(2):10–1. doi: 10.1097/00006247-200002000-00009. [DOI] [PubMed] [Google Scholar]
- 8.McGuinness SD, Peters S. The diagnosis of multiple sclerosis: Peplau's Interpersonal Relations Model in practice. Rehabil Nurs. 1999;24(1):30–3. doi: 10.1002/j.2048-7940.1999.tb01828.x. [DOI] [PubMed] [Google Scholar]
- 9.Sahebalzamani M, Rashvand F. The study of training demands of patients afflicted with MS, members to Iran's MS Society and presenting a proper training model for these patients. Medical Science Journal of Islamic Azad Univesity Tehran Medical Branch. 2008;18(3):195–200. [Google Scholar]
- 10.Rashvand F, Aliloo L, Sahebalzamani M, Rahmani A. Educational, Psycho Mental and Socio economical needs of an Iranian Cohort with Multiple Sclerosis. Oman Medical journal. 2010;25(1):22–5. doi: 10.5001/omj.2010.6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Montel SR, Bungener C. Coping and quality of life in one hundred and thirty five subjects with multiple sclerosis. Mult Scler. 2007;13(3):393–401. doi: 10.1177/1352458506071170. [DOI] [PubMed] [Google Scholar]
- 12.Sutherland G, Andersen MB, Morris T. Relaxation and health-related quality of life in multiple sclerosis: the example of autogenic training. J Behav Med. 2005;28(3):249–56. doi: 10.1007/s10865-005-4661-2. [DOI] [PubMed] [Google Scholar]
- 13.Twork S, Wirtz M, Schipper S, Klewer J, Bergmann A, Kugler J. Chronical illness and maternity: life conditions, quality of life and coping in women with multiple sclerosis. Qual Life Res. 2007;16(10):1587–94. doi: 10.1007/s11136-007-9268-3. [DOI] [PubMed] [Google Scholar]
- 14.Hamidi Zadeh S, Masoudi R, Ahmadi F, Mohamadi E. Haidizadeh M The Influence of Orem Self Care Training on Physical Quality of life in Patients with Multiple Sclerosis. Journal of Shaeed Sdoughi University of Medical Sciences Yazd. 2009;17(2):20–9. [Google Scholar]
- 15.Solari A, Radice D. Health status of people with multiple sclerosis: a community mail survey. Neurol Sci. 2001;22(4):307–15. doi: 10.1007/s10072-001-8173-8. [DOI] [PubMed] [Google Scholar]
- 16.Ennis M, Thain J, Boggild M, Baker GA, Young CA. A randomized controlled trial of a health promotion education programme for people with multiple sclerosis. Clin Rehabil. 2006;20(9):783–92. doi: 10.1177/0269215506070805. [DOI] [PubMed] [Google Scholar]
- 17.Samgelaji B, Hatami Zadeh N, Rashvand F, Kazem Nejad A. The effect of rehabilitation on quality of life of people with MS. Journal of Nursing & Midwifery, Shahid Beheshti University of Medical Sciences and Health Services. 2010;20(71):36–41. [Google Scholar]
- 18.Zohrevand P. Multiple Sclerosis and Education: a demographic study. Proceedings of the 2nd International Congress on multiple sclerosis; 2005 Nov 20; Isfahan, Iran. 2005:32–8. [Google Scholar]
- 19.Pekmezovic T, Kisic Tepavcevic D, Kostic J, Drulovic J. Validation and cross-cultural adaptation of the disease-specific questionnaire MSQOL-54 in Serbian multiple sclerosis patients sample. Qual Life Res. 2007;16(8):1383–7. doi: 10.1007/s11136-007-9234-0. [DOI] [PubMed] [Google Scholar]
- 20.Somers S. Group therapy for people with multiple sclerosis improves complain Exercise program. Way Ahead. 2002;5(3):33. [Google Scholar]
- 21.Patti F, Ciancio MR, Cacopardo M, Reggio E, Fiorilla T, Palermo F, et al. Effects of a short outpatient rehabilitation treatment on disability of multiple sclerosis patients-a randomised controlled trial. J Neurol. 2003;250(7):861–6. doi: 10.1007/s00415-003-1097-x. [DOI] [PubMed] [Google Scholar]