

Abstract
Dentigerous cysts are always associated with an embedded or unerupted tooth; involvement of more than one permanent tooth in a single cyst follicle is exceedingly rare and only a few such cases can be found in the literature. The cysts reported in the literature involving multiple teeth typically consist of mesiodens or odontomas. Here we report a rare case of dentigerous cyst associated with two permanent teeth causing displacement of maxillary canine into the osteo meatal complex and maxillary premolar to lateral nasal wall. The possible etiopathogenesis of such cases is also discussed here.
Keywords: Dentigerous cyst, multiple teeth, tooth displacement
INTRODUCTION
Dentigerous cysts are the second most common odontogenic cysts after radicular cysts and are associated with the crown of an unerupted tooth. These cysts may involve impacted, unerupted permanent teeth, supernumerary teeth, odontomas, and rarely, deciduous teeth.[1] According to pathogenesis dentigerous cyst can be of two types: the first is developmental in origin and occurs in mature teeth usually as a result of impaction. The second type is inflammatory in origin and occurs in immature teeth as a result of inflammation from a nonvital deciduous tooth follicle.[2] Dentigerous cysts are often asymptomatic and are usually diagnosed during routine radiographic examination; however they can enlarge, causing bone expansion, erosion, pathologic fractures or may become secondarily infected. Metaplastic and dysplastic changes may also occur. Surgical excision and pathologic analysis of the lesion is essential for the definitive diagnosis.[1]
Dentigerous cyst most often develop in association with impacted third molars, less frequently with impacted maxillary canines or other teeth. Cases of dentigerous cyst associated with supernumerary teeth and odontomas have also been reported frequently. Medline search shows only three cases of a single dentigerous cyst involving multiple permanent teeth. Here we present a rare case of a maxillary dentigerous cyst associated with two permanent teeth and aim to discuss the etiopathogenesis of multiple teeth in a single follicle.
What exactly initiates the presence of more than one tooth in a single cystic lining is a perplexity and can only be speculated.
CASE REPORT
A 40-year-old female reported at our center with the complaint of swelling in the right cheek and palate since 7–8 months which was gradually increasing in size.
Extraoral examination revealed right maxillary expansion. The swelling had displaced the lateral nasal wall and the nasal floor. Intraorally, the swelling had extended onto the maxillary alveolar process and adjoining right palatal region extending up to midline. The patient did not report of any pain or paresthesia. Except for the facial asymmetry, physical examination was unremarkable, and routine laboratory tests were within normal limits.
Lateral skull radiograph showed a large radiolucent region occupying the whole maxillary sinus region with thinning of the maxillary walls and elevation of the orbital floor. The right permanent maxillary canine was displaced to the osteo meatal complex and the permanent premolar to the right nasal wall [Figure 1]. Computed tomography (CT) scan-PNS showed a large expansile bone lesion of 3.5 × 4.4 cm dimension in the right maxilla obliterating the right maxillary antrum and involving the right alveolar margin with an unerupted tooth visible in the osteo meatal complex and a second unerupted tooth in lateral nasal wall in different coronal sections of CT, suggestive of dentigerous cyst associated with two teeth [Figures 2 and 3].
Figure 1.

Lateral skull radiograph showing both teeth
Figure 2.

CT scan coronal view, showing canine displaced in osteo meatal complex
Figure 3.
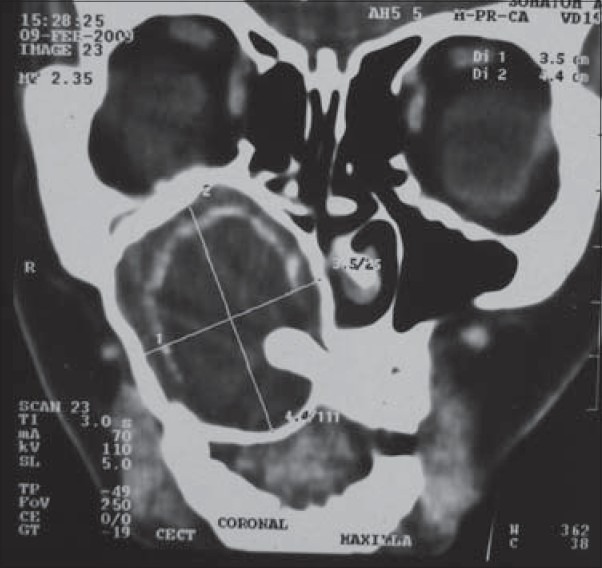
CT scan coronal view, showing premolar displaced in lateral nasal wall
A provisional diagnosis of dentigerous cyst was made and the patient was operated under general anaesthesia by the Caldwell-Luc approach. The cyst was enucleated completely and both the teeth were removed, and the lining epithelium was found attached to the crown of both the teeth [Figure 4].
Figure 4.
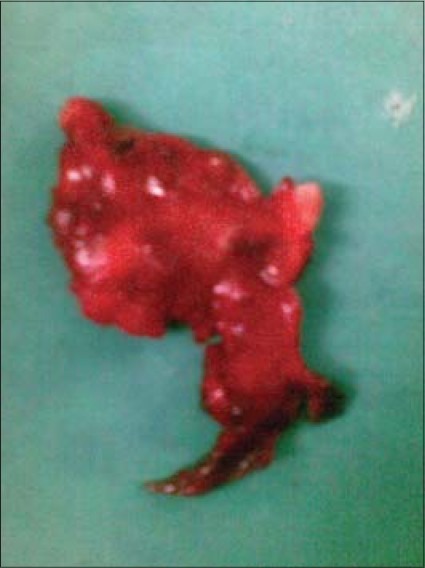
Excised cyst lining with attached teeth
On histopathological examination, a thin fibrous wall lined by nonkeratinized stratified squamous epithelium and connective tissue with inflammatory cell infiltrate was seen. The clinical and histological findings were consistent with the diagnosis of dentigerous cyst.
Postoperatively, the facial and palatal swelling subsided gradually and the patient has been asymptomatic over a 1-year follow-up period.
DISCUSSION
The word dentigerous means “tooth bearing” which describes the cyst appropriately. Dentigerous cyst develops only after the tooth crown is mostly formed, and the precise sequence of events leading to its origin is uncertain. It has been suggested that dentigerous cyst may develop by fluid accumulation either between the reduced enamel epithelium and the enamel or alternatively between individual layers of the reduced enamel epithelium.[3] This fluid accumulation occurs due to pressure exerted by an erupting tooth on an impacted follicle, obstructing the venous outflow and inducing rapid transudation of serum across the capillary wall.[4] Toller stated the origin of dentigerous cyst is breakdown of proliferating cells of the follicle after impeded eruption. These breakdown products result in increased osmotic tension and hence cyst formation.[5] An inflammatory etiology has also been proposed in the pathogenesis of some dentigerous cysts. Bloch suggested that periapical inflammation from the overlying deciduous tooth spreads to involve the permanent successor, due to which inflammatory exudates ensues and results in dentigerous cyst formation.[6] The crowns of permanent teeth may erupt into radicular cysts or other periapical inflammatory lesions at the apices of its deciduous predecessors.
In either of the situations, the question arises as to what circumstances lead to the presence of more than one tooth in a single follicle. Two possible theories have been speculated to explain this, one is a fusion between two adjacent dentigerous cyst linings and the other is a fusion between the lining of one preexisting cyst and the lining of reduced enamel epithelium surrounding the adjacent tooth.[7,8]
Another possibility that we would like to hypothesize is that the tooth pushed ectopically further away from the alveolus (due to the expansion of the cyst) tends to erupt in the cyst lining in the same fashion as it erupts in the oral mucosa, somewhat in the similar manner as Altini and Cohen had suggested that a tooth might erupt into a preexisting keratocyst cavity as it erupts into the oral mucosa.[6] A prerequisite for this kind of cyst to develop is that the size of the cyst should be significantly large to displace the surrounding teeth from their natural eruption path. This appears to hold true in all such cases reported in the literature[9,10] supporting this hypothesis and also explains the presence of multiple teeth in a single dentigerous cyst. Further studies specific to such cases are required to verify this proposed theory.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Ustuner E, Fitoz S, Atasoy C, Erden I, Akyar S. Bilateral maxillary dentigerous cysts. A case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;95:632–5. doi: 10.1067/moe.2003.123. [DOI] [PubMed] [Google Scholar]
- 2.Benn A, Altini M. Dentigerous cysts of inflammatory origin: A clinicopathologic study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996;81:203–9. doi: 10.1016/s1079-2104(96)80416-1. [DOI] [PubMed] [Google Scholar]
- 3.Shear M. Developmental odontogenic cysts. An update. J Oral Pathol Med. 1994;23:1–11. doi: 10.1111/j.1600-0714.1994.tb00246.x. [DOI] [PubMed] [Google Scholar]
- 4.Main DM. The enlargement of epithelial jaw cyst. Odontol Revy. 1970;212:1–9. [PubMed] [Google Scholar]
- 5.Toller PA. The osmolarity of fluid from the cyst of jaw. Br Dent J. 1970;129:275–8. doi: 10.1038/sj.bdj.4802570. [DOI] [PubMed] [Google Scholar]
- 6.Bloch JK. Dentigerous cyst. Dent Cosm. 1928;70:708–11. [Google Scholar]
- 7.Nishikawa S, Cheng J, Koyano Y, Irie T, Nomura T, Kato T, et al. Dentigerous cyst involving two impacted molars: Report of a Case. Oral Med Pathol. 1996;1:60–2. [Google Scholar]
- 8.Altini M, Cohen M. The follicular primordial cyst odontogenic keratocyst. Int J Oral Surg. 1982;11:175–82. doi: 10.1016/s0300-9785(82)80005-7. [DOI] [PubMed] [Google Scholar]
- 9.Sumer M, Bas S, Yildiz L. Inferior alveolar nerve paresthesia caused by a dentigerous cyst associated with three teeth. Med Oral Patol Oral Cir Bucal. 2007;12:E388–90. [PubMed] [Google Scholar]
- 10.Ertas U, Yavuz MS. Interesting eruption of 4 teeth associated with a large dentigerous cyst in mandible by only marsupialization. J Oral Maxillofac Surg. 2003;61:728–30. doi: 10.1053/joms.2003.50145. [DOI] [PubMed] [Google Scholar]