

Abstract
We report the 23rd case of the world of one of the rare congenital anomalies, supernumerary nostril. The disease has a variable presentation and more than half of the reported cases are from Asian continent. This patient had a supernumerary nostril in the form of a accessory blind tract above the left ala. The tract was excised and raw areas approximated with a bolster dressing.
Keywords: Congenital, rare, supernumerary nostril
INTRODUCTION
Supernumerary nostril or accessory nostril is one of the rarest congenital nasal deformities with severe cosmetic ramifications. An extensive search of literature revealed 22 reported cases with an Indian predominance of 7 afflicted children (including the one described). The geographical and environmental factors could be the risk factors for developing such an anomaly as of the reported cases more than half are from Asia.
CASE REPORT
A 6-month-old male infant presented to the Outpatient Department of Plastic Surgery and Burns of Dayanand Medical College and Hospital at Ludhiana with nasal deformity [Figure 1]. He was the first born male child to a mother aged 26 years and father aged 29 years, both agriculturists. He was born through a full-term normal vaginal delivery.
Figure 1.

Preoperative view
There was no history of such similar deformity or any facial cleft and or deformity in the paternal and maternal side of the family for three known generations. On examination, a supernumerary nostril was located above the left nostril with a smaller but similar contour of the nostril. The internal and external diameter of the accessory nostril was 2 and 5 mm and ended blindly at 2 mm depth. The underlying ala was depressed, but the normal nostrils were of equal diameter and projection. There was no flaring or expansive effect on crying in the supernumerary nostril. There were no other congenital malformations.
Infant was taken up for surgery under general anesthesia. Incision was marked all along the inner circumference of the supernumerary nostril [Figure 2] and the blind ending nasal tract was circumferentially excised [Figure 3]. There was no communication between the supernumerary and normal nostril. The skin margins were sutured with 5-0 nylon with an additional excision of 1 mm skin on medial aspect to avoid dog ear formation. A full-thickness (through and through) suture was passed 3 mm posterior to the suture line to compress the excessive bulge and to collapse the dead space [Figure 4]. The histopathology of the excised tract showed covering of stratified squamous epithelium with presence of skin appendages in the dermis [Figure 5].
Figure 2.

Incision marked
Figure 3.

Intraoperative view after excision
Figure 4.

Primary closure done
Figure 5.
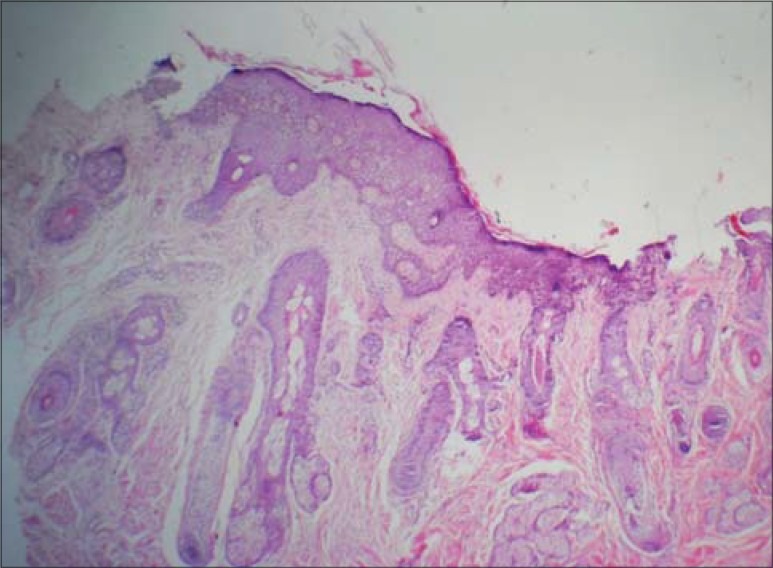
Histopathology of excised tract showing stratified squamous epithelium with dermal appendages (H&E stain, 10×)
Postoperative period was uneventful. Patient has mild bulge in the involved nostril region which is expected to settle down over a period of time [Figure 6].
Figure 6.

Postoperative view
DISCUSSION
Supernumerary nostril is among the rare congenital deformities of the nose,[1–3] with Indian newborns forming the majority (30.44%) among the reported cases in world literature. Similar temporal association can be applied to the fact that Asians form more than half the cases of supernumerary nostril.[4]
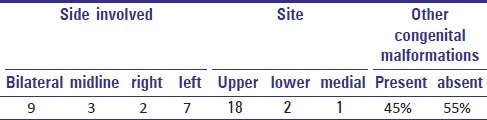
The first reported case of bilateral supernumerary nostrils was published by Lindsay[1] in 1906. It was described to be different from the double nose with two septae and four nostrils and nasal cavities.[5] The etiology cannot be accurately determined, but the varied presentations [Table 1] can be hypothesized from the development of the embryo. According to Erich, during the course of the evolution of the nasal placode, four nasal pits appeared horizontally, each became a nasal sac, and the medial two which were interposed between the two nasal laminae, prevented the laminae from fusing into one nasal septum. This resulted in double nose.[6] Supernumerary nostril is formed when the accessory nasal pit is located so laterally to the nasal lamina that the accessory nostrils are formed above the natural nostril and thus do not disturb the fusion of the nasal laminae.[6] Nakamura hypothesized that during the proliferation of mesenchymal cells in the lateral nasal process, a concavity or fissure appears in this area accidentally, and thus this lateral nasal process is divided into two segments, resulting in two nostrils and two alae on one side.[2] This hypothesis can extrapolate the appearance of accessory nostril either above or lateral (as in our case) to the natural nostril or medially, depending on the position of change in the lateral nasal process.
Table 1.
Presentation of supernumerary nostrils
We followed the surgical technique as suggested by Diogo Franco[4] in which whole of the tract is circumferentially excised and the raw areas approximated. It is important to resect the entire fistulous tract and restore the shape and grooving of the normal nostril.[7]
Timing of surgery is as important as the planning of the incision. Excision performed at an early age, similar to cleft lip treatment, avoids any serious impact on the nasal cartilages due to the fistula, deformation of the adjacent structures, psychological effects that might ensue, and reduces anaesthetic complications.[3,8]
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Lindsay B. A nose with supernumerary nostrils. Trans Pathol Soc Lond. 1906;57:329–36. [Google Scholar]
- 2.Nakamura K, Onizuka T. A case of supernumerary nostril. Plastic Recontr Surg. 1987;80:436–41. doi: 10.1097/00006534-198709000-00018. [DOI] [PubMed] [Google Scholar]
- 3.Reddy KA, Rao AK. Tripple nostrils: A case report and review. Br J Plast Surg. 1987;40:651–2. doi: 10.1016/0007-1226(87)90164-0. [DOI] [PubMed] [Google Scholar]
- 4.Franco D, Medeiros J, Faveret P, Franco T. Supernumeray nostril: Case report and review of literature. J Plast Reconstr Aesth Surg. 2008;61:442–46. doi: 10.1016/j.bjps.2006.04.007. [DOI] [PubMed] [Google Scholar]
- 5.Onizuka T, Tai Y. Supernumerary nostril. Plast Reconstr Surg. 1972;50:403–5. doi: 10.1097/00006534-197210000-00025. [DOI] [PubMed] [Google Scholar]
- 6.Erich JB. Nasal duplication: Report of case of a patient with two noses. Plast Reconstr Surg. 1962;29:159. [PubMed] [Google Scholar]
- 7.Deshpande SN. Congenital duplication of nostril. Indian J Plast Surg. 1995;28:39–41. [Google Scholar]
- 8.Hallak A, Jamjoom H, Hosseinzadeh T. Supernumerary nostrils: A case report and review. Aesthetic Plast Surg. 2001;25:241–3. doi: 10.1007/s002660010127. [DOI] [PubMed] [Google Scholar]