

Abstract
Purpose
Findings from cross-sectional studies of knee angle development in Nigerian children vary in values and in the age at which the varus angle changes to the valgus angle. This study was conducted to describe knee angle development and to determine the age when the knee angle changes from the varus to the valgus angle.
Methods
This was a longitudinal survey of 152 Nigerian children recruited within 3 weeks of life and followed up monthly until age 3 years. Their knee angle was measured using clinical methods.
Results
The mean tibio-femoral/varus knee angle (13.2 ± 3.8°) at birth–3 weeks of life decreased sharply to 5.6 ± 0.7° at 9 months, increased slightly to 6.3 ± 1.1° at 13 months, and then decreased again up to age 18 months (0.3 ± 2.1°). The mean valgus knee angle increased from −2.4 ± 2.5° at 19 months of life to −8.5 ± 2.5° at 27 months and then decreased to −7.7 ± 2.2° at 36 months. Intercondylar/intermalleolar distances (ICD/IMD) showed a similar pattern, changing from an extreme varus knee (ICD) at birth–3 weeks of life (2.5 ± 0.7 cm), decreasing to 0.6 ± 0.2 cm at 9 months, increasing to 0.8 ± 0.5 cm at 12 months, and decreasing to 0.1 ± 0.4 cm at 15 months. The mean IMD increased from −0.1 ± 0.8 cm at 16 months of life to −2.0 ± 1.5 cm at 29 months and then decreased up to 36 months. Our tri-modal analysis showed that the transition from the varus to the valgus angle was between 18 and 19 months.
Conclusion
Our findings suggest that the developmental pattern of the knee angle in Nigerian children is at maximal varus at birth, neutral at 18 months of life, and valgus at 19 months, with the valgus angle continuing to increase up to 36 months.
Keywords: Knee angle, Tibio-femoral angle, Intercondylar distance, Intermalleolar distance, Nigerian children
Introduction
Healthcare providers are frequently asked to assess children for excessive bowing of the lower limb [1]. Such an assessment focuses on differentiating physiological bowing from abnormal bowing and is facilitated by a good knowledge of the developmental pattern and age-reference values of the knee/tibio-femoral angle (TFA) for a specific population. Children generally present with a varus knee angle at birth [2–4]. However, the results from previous studies on TFA developmental patterns and values suggest that racial differences are present [2, 4–7].
The developmental pattern of the TFA in Nigerian children has been reported in three cross-sectional studies [3, 8, 9]. However, the TFA patterns reported for Nigerian children in these studies vary, likely because the studies relied only on single measurements and differed with respect to the age of the study cohorts. It has been suggested that longitudinal studies on TFA would provide more reliable data than cross-sectional studies [4, 10]. However, to date no longitudinal studies have been carried out on TFA in Nigerian children, although a preliminary study of the developmental pattern of TFA in Nigerian children during the first 12 months of life has been published [11]. The aims of the study reported here were to describe the developmental pattern of TFA during the first 3 years of life and to determine the age when the TFA changes from the varus angle to the valgus knee angle in a cohort of Nigerian children.
Methods
The study was approved by the research ethics committee of the Olabisi Onabanjo University Teaching Hospital, Sagamu. Prior to data collection, a standard equation was used to determine the sample size using the standard deviations (SD) of previous studies carried out on Nigerian children with a 95 % confidence interval (CI); the width of confidence interval set at 2 [3, 8, 12]. The calculated minimum sample size was determined to be 96 to power the study. To allow for attrition, we recruited a total of 152 healthy infants (71 males, 81 females) without any obvious congenital deformity within 3 weeks of life from three infant welfare clinics in Sagamu town using a consecutive sampling technique. The parents gave informed consent. The children were followed up monthly from birth/within 3 weeks of life through to 36 months of age to assess their knee angle development.
Measurements
All measurements were carried out by the first author to minimize inter-observer variations, and measurements were repeated on 16 children in order to ascertain intra-tester reliability. Clinical methods were used to measure TFA directly using a universal goniometer and indirectly by measuring the intercondylar distance (ICD) or intermalleolar distance (IMD). Earlier studies have reported that ICD and IMD values can be used as indices of the varus knee angle and valgus knee angle, respectively [2, 6, 9]. The goniometric measurement of TFA was taken with each child placed supine in anatomical position, as reported previously [11]. The acute angle sustained between the femoral shaft and the tibia shaft on the goniometer was recorded as the TFA in degrees. The angles were assigned a positive value for the varus knee angle and a negative value for the valgus knee angle.
The ICD and IMD were measured with a non-elastic tape ruler (Butterfly Brand, China). The measurements were taken with each child supine in an anatomical position with the medial malleolus (ICD) or medial tibial condyle (IMD) just touching and the pelvic square, with the hip and knees in maximal extension [8]. The measurement was made to the nearest 0.1 cm.
Data analysis
The data were analyzed with Statistical Package for Social Sciences (SPSS) ver. 16 (SPSS, Chicago, IL). Intra-tester reliability was analyzed using the intra-class correlation (ICC). Data were summarized using the mean and SD, and graphs were plotted to describe the TFA developmental pattern. Tri-modal analysis was performed to determine the age at which the varus angle transitioned into the valgus angle. The 95 % CI (2SD) was used to determine reference/normal values of TFA and ICD/IMD. Pearson’s correlation was used to determine the relationship between the ICD/IMD and TFA, and the t test was used to determine differences in the measured parameters according to sex.
Results
The ICC for repeated measurements on 16 of the children was high for both the goniometry (ICC 0.98, 95 % CI 0.95–0.99) and ICD/IMD (ICC 0.99, 95 % CI 0.98–1.00) measurements. Of the 152 healthy children recruited for the study, 68 were recruited at age 0–7 days, 46 at age 8–14 days, and 38 at age 15–24 days. The attendance of the participants at the monthly measurement follow-up is shown in Fig. 1. Eighty-six children were seen 37 times, 32 children were seen 30–36 times, 12 children were seen 10–25 times, eight children were seen three to six times, and 14 were seen only at initial contact. By the end of the 36-month study period, 39 children had defaulted, which is an attrition rate of 25.7 %. Attrition resulted from death (3 children), withdrawal from the study (1 child), untraceable address (13 children), and relocation of family to another town (parents of 22 children).
Fig. 1.
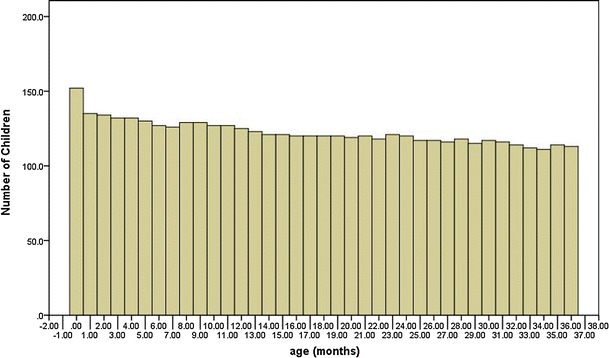
Attendance of children at monthly measurement sessions according to age
The left and right knee angles were very highly correlated (r = 0.992, p = 0.01), and we therefore calculated the average of both limbs for each child and used this value for further analysis. There were no significant differences in the values of TFA determined by goniometry according to sex (t = 0.88, p = 0.38) and ICD/IMD (t = 0.16, p = 0.88). Therefore, the data of both boys and girls were pooled for further analysis. There was significantly high correlation between TFA and ICD/IMD (r = 0.77, p = 0.01).
The children had a maximum varus knee angle at birth–3 weeks of life (range 5–25°). The mean varus knee angle during the first 3 weeks of life was 13.2 ± 3.8°; this decreased sharply to 6.7 ± 1.4° at 3 months, then more slowly to 5.6 ± 0.7° at 9 months. The varus angle increased slightly to 6.3 ± 1.1° at 13 months of life and thereafter decreased until 18 months (0.3 ± 2.1°) (Fig. 2). The tri-modal analysis showed that at age 18 months, the majority (65.8 %) of the children had a neutral knee angle (0°), 24 (20.0 %) children had a varus knee angle, and 17 (14.2 %) children had a valgus knee angle (Fig. 3). At age 19 months, the TFA of 102 (85 %) children had changed to a valgus knee angle. Of the 18 children whose knee angle remained at a varus knee angle or at a neutral knee angle at 19 months, ten had a family history of genu varus deformity. All but six children had changed to a valgus knee angle by age 25 months. In four of these six children whose TFA pattern remained varus beyond age 25 months, the varus pattern persisted on only one of the lower limbs. The varus angle spontaneously had changed to valgus in all of these six children by age 33 months. The mean valgus knee angle increased steadily from −2.4 ± 2.5° at 19 months of life to −8.5 ± 2.5° at 27 months and then decreased slightly to −7.7 ± 2.2° at age 36 months (Fig. 2).
Fig. 2.
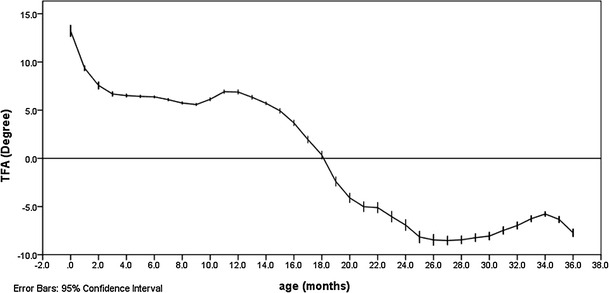
Knee/tibio-femoral angle (TFA) according to age
Fig. 3.
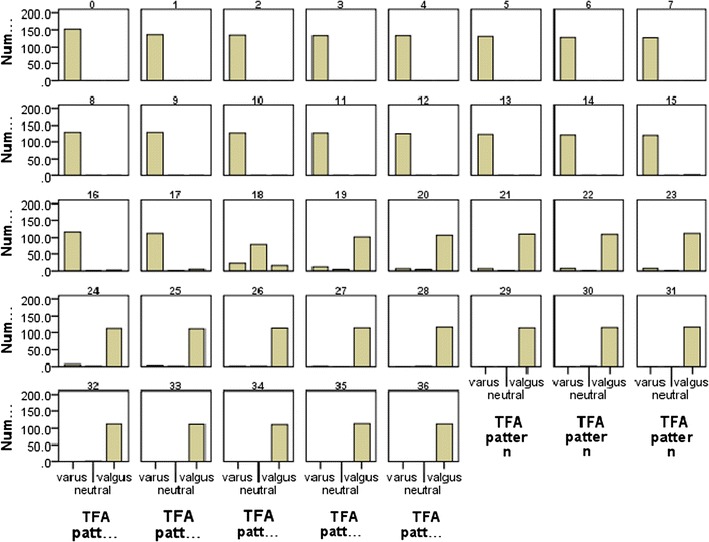
Frequency distributions of knee angle (TFA) in infants during development according to age (months)
The ICD/IMD depicted a course of TFA development similar to that shown by the goniometric measurement: an extreme varus knee pattern (ICD) during first 3 weeks of life (2.5 ± 0.7 cm), which decreased gradually to 0.6 ± 0.2 cm at age 9 months (Fig. 4). The ICD increased slightly to 0.8 ± 0.5 cm at age 12 months, then decreased to 0.1 ± 0.4 cm by age 15 months. The tri-modal analysis showed that half of the children (50.4 %) had a neutral knee pattern (0 cm) at age 15 months (Fig. 5). At age 16 months, the knee pattern was predominantly valgus, with 60 % of the children showing an IMD pattern, 16.7 % showing a ICD (varus) pattern, and 23.3 % showing 0 cm (neutral knee pattern). By age 19 months, the knee pattern in the majority (90 %) of the children was valgus. Of the 12 children who retained a varus or neutral knee angle at 19 months, seven had a family history of genu varus. All but six children had changed to a IMD/valgus knee angle by age 25 months. The mean IMD increased gradually from −0.1 ± 0.8 cm at age 16 months, to −2.0 ± 1.5 cm at age 29 months, and thereafter decreased to −1.9 cm at 36 months.
Fig. 4.
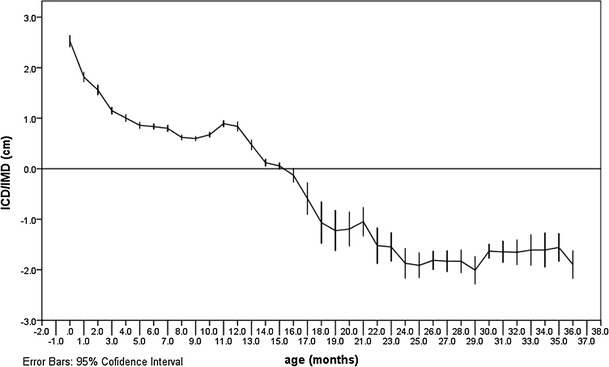
Intercondylar/intermalleolar distances (ICD/IMD) according to age
Fig. 5.

Frequency distribution of knee angle (ICD/IMD) in infants during development according to age (months)
Table 1 shows the TFA reference values generated in this study.
Table 1.
Reference values for knee/tibio-femoral angle and intercondylar/intermalleolar distances for the study cohort
| Age (months) | Tibio-femoral angle | ICD/IMD | ||||
|---|---|---|---|---|---|---|
| Mean | −2SD | +2SD | Mean | −2SD | +2SD | |
| 0 | 13.23 | 12.63 | 13.83 | 2.53 | 2.44 | 2.64 |
| 1–3 | 7.88 | 7.67 | 8.08 | 1.51 | 1.45 | 1.57 |
| 4–6 | 6.44 | 6.36 | 6.52 | 0.90 | 0.86 | 0.94 |
| 7–9 | 5.80 | 5.72 | 5.87 | 0.67 | 0.64 | 0.70 |
| 10–12 | 6.64 | 6.53 | 6.75 | 0.80 | 0.76 | 0.84 |
| 13–15 | 5.66 | 5.54 | 5.79 | 0.22 | 0.17 | 0.27 |
| 16–18 | 1.99 | 1.75 | 2.23 | −0.59 | −0.78 | −0.41 |
| 19–21 | −3.84 | −4.14 | −3.54 | −1.16 | −1.35 | −0.96 |
| 22–24 | −6.03 | −6.36 | −5.71 | −1.65 | −1.83 | −1.47 |
| 25–27 | −8.38 | −8.70 | −8.07 | −1.85 | −1.98 | −1.73 |
| 28–30 | −8.25 | −8.49 | −8.02 | −1.82 | −1.95 | −1.70 |
| 31–33 | −6.91 | −7.13 | −6.69 | −1.64 | −1.78 | −1.49 |
| 34–36 | −6.62 | −6.83 | −6.40 | −1.69 | −1.86 | −1.52 |
ICD/IMD Intercondylar/intermalleoli distances, SD standard deviation
Discussion
Of the children enrolled in our study (age range 0–36 months), those in the birth–3 weeks of life group had the highest value of TFA, suggesting that most Nigerian children are born with an extreme varus knee angle. This finding is similar to those reported in previous studies [2, 3, 5]. In most of the children in our study, the initial extreme varus knee angle became neutral (0°) at age 18 months and became valgus by age 19 months. The valgus angle continued to increase from age 20 months up to age 36 months (end of study period). Although the majority of children in our study were of the Yoruba tribe, the other major tribes in the country were also represented. It is likely that if this study were to be conducted in other parts of the country, the same findings would be obtained. The age of transition from the varus to the valgus angle determined in our study, 18–19 months, is younger than that (21–23 months) reported for Nigerian children in a previous study [3], possibly because in the previous study only one measurement was taken whereas in our longitudinal study, we took repeated measurements on the same group of children. The age of transition from the varus to the valgus obtained in our study also differs from that (12–24 months) reported for Pakistani children [13]. Our results corroborate those of previous studies which reported a neutral knee angle at age 18 months [2, 4, 5]. The outcomes of this study indicate that the TFA developmental pattern in Nigerian children during the first 3 years of life may be described in three phases: phase 1 (birth to 15 months) or the phase of the varus angle; phase 2 (16–19 months) or the phase of transition from the varus to the valgus angle; phase 3 (20–36 months) or the phase of increased valgus. The slight increase in the values of TFA at age 10 months is noteworthy as many of these children had started walking with assistance around this age. It has been suggested that the duration of this period of ‘dependent walking’ correlates with the knee angle in children [14]. The average age at which our participants attained the ability to walk independently was 12 months, which is much earlier than the age of knee angle transition from the varus to the valgus knee pattern and may imply that the transition from the varus to the valgus knee pattern is not related to the age when children attain the ability to walk independently. However, a slight increase in the varus angle value at age 12 months was noted, and this corroborates the values reported in a previous study from Nigeria [3]. None of the infants involved in our study presented a valgus knee angle before age 15 months, suggesting that a measurable valgus knee angle in a Nigerian child before age 15 months may be regarded as unusual. Of the 18 children whose knee angle remained varus or neutral at age 19 months, ten had family history of genu varus deformity, possibly indicating that any delay in the knee pattern changing from the varus to the valgus may be associated with the development of genu varus deformity in life. However, such speculation is beyond the scope of our study which covers infancy to age 3 years. In addition, the knee angle spontaneously changed to the valgus pattern in all the children before age 3 years.
A comparison of knee angle values obtained in this study with those of a number of previous studies is difficult because of differences in the age intervals of the children for whom the values are presented. The mean TFA value for the children aged from birth to 3 weeks in our study (13.2°) fell within the range of values (12–16.5°) reported for Korean, Finnish and American children at 6 months [2, 4, 5]. However, the mean TFA value for those children age 6 months in our study (6.4°) is lower than the values reported from these same studies. These slight differences may be due to differences in the manner the data were presented in our study and the other studies. We present data collected at monthly intervals while some of the previous studies present data collected at 6-month intervals.
The finding that the age of peak valgus knee angle during the study period (3 years) was 27 months is close to the age of 36 months reported in previous studies [3, 6, 15]. The peak valgus knee angle (8.5°) is similar to that of American, Korean and Indian children at ages 4 and 6 years [2, 4, 10]. Although the use of different techniques to estimate the knee angles might be responsible for variations in observations in the different studies, it is more likely that these variations are due to possible ethnic and racial differences between different population groups.
The measurement of ICD/IMD in our study showed a similar pattern of development to that of the goniometric measurement in children, with an extreme varus knee at birth that decreased with age until 15 months. By age 16 months the children in our study had predominantly a valgus knee angle. The varus knee angle did not disappear in our population until age 19 months. A similar pattern was also reported in previous studies [2, 9, 16]. Few previous studies that measured ICD/IMD reported values for age groups rather than specific ages [2, 16]. This makes it difficult to compare the values from these previous studies with the mean values for specific ages in our study. However, the mean ICD value (2.5 cm) at birth in our study is similar to that of American children (2.6 cm) and Pakistan children (2.96 cm) at 6 months [2, 16]. The mean ICD value at age 6 months (0.83 cm) in our study is lower than that of these previous studies [2, 16]. This difference in the observed values may be due to racial differences. All of the newborns had a varus knee angle with a mean ICD of 2.5 cm (range 0.5–4.0 cm), decreasing to a mean of 0.1 cm at age 15 months. This is similar to that of Chinese children who have been reported to have a maximum varus knee at birth (3.0 cm) (range 0–5.5 cm), decreasing to 0 cm at age 12 months [6]. In Nigerian children, the medial condyles touch late (15 months) compared with Chinese and American children (12 months) [2, 6]. In our study, the children had a peak valgus knee angle (−2.0 cm) at age 29 months, which is similar to that of Chinese (−2.8 cm), American (−3.5), and Pakistani (−3.96 cm) children, but Nigerian children peak earlier [2, 6, 16].
The high correlation between ICD/IMD and TFA implies that ICD/IMD are good indices of TFA. Thus, any of the two measures can be used to monitor the progress of knee angle of children. The lack of significant sex differences in the TFA and ICD/IMD patterns and values implies that the same reference can be used for both sexes. Our results indicate that TFA developmental pattern and values are the same for both limbs. Thus, any obvious discrepancy between the limbs may be pathological. The age-reference values established in our study may be useful for assisting healthcare providers in their screening of Nigerian children for abnormalities in TFA. It may also help clinicians or surgeons to differentiate between physiological bowing and Blount’s disease.
Conclusion
The chronological development of knee angle in Nigerian children is a maximal varus knee angle at birth, a neutral knee at age 18 months, changes to the valgus knee by age 19 months, and increases up to age 3 years. Both goniometric and ICD/IMD measurements are reliable and can be used in the clinic. We recommend using the age-referenced values generated in this study for practical evaluation of Nigerian children when evaluating lower limb alignment.
References
- 1.Davids JR, Blackhurst DW, Allen BL. Radiographic evaluation of bowed legs in children. J Pediatr Orthop. 2001;21:257–263. [PubMed] [Google Scholar]
- 2.Heath CH, Staheli LT. Normal limits of knee angle in white children—genu varum and genu valgum. J Pediatr Orthop. 1993;13:259–262. [PubMed] [Google Scholar]
- 3.Oginni LM, Badru OS, Sharp CA, Davie MWJ, Worsfold M. Knee angles and rickets in Nigerian children. J Pediatr Orthop. 2004;24:403–407. doi: 10.1097/01241398-200407000-00011. [DOI] [PubMed] [Google Scholar]
- 4.Yoo JH, Choi IH, Cho T, Chung CY, Yoo WJ. Development of tibiofemoral angle in Korean children. J Korean Med Sci. 2008;23:714–717. doi: 10.3346/jkms.2008.23.4.714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Salenius P, Vankka E. The development of the tibiofemoral angle in children. J Bone Joint Surg Am. 1975;57:259–261. [PubMed] [Google Scholar]
- 6.Cheng JC, Chan PS, Chiang SC, Hui PW. Angular and rotational profile of the lower limb in 2,630 Chinese children. J Pediatr Orthop. 1991;11:154–161. doi: 10.1097/01241398-199103000-00003. [DOI] [PubMed] [Google Scholar]
- 7.Arazi M, Ogun TC, Memik R. Normal development of the tibiofemoral angle in children: a clinical study of 590 normal subjects from 3 to 17 years of age. J Pediatr Orthop. 2001;21:264–267. [PubMed] [Google Scholar]
- 8.Omololu B, Tella A, Ogunlade SO, Adeyemo AA, Adebisi A, Alonge TO, Salawu SA, Akinpelu AO. Normal values of knee angle, intercondylar and intermalleolar distances in Nigerian children. West Afr J Med. 2003;22:301–304. doi: 10.4314/wajm.v22i4.28051. [DOI] [PubMed] [Google Scholar]
- 9.Ezeuko VC, Owah S, Ukoima HS, Ejimofor OC, Aligwekwe AU, Bankole L. Clinical study of the chronological changes in knee alignment pattern in normal south-east Nigerian children aged between 0 and 5 years. Electron J Biomed. 2010;1:16–21. [Google Scholar]
- 10.Saini UC, Bali K, Sheth B, Gahlot N, Gahlot A. Normal development of the knee angle in healthy Indian children: a clinical study of 215 children. J Child Orthop. 2010;4:579–586. doi: 10.1007/s11832-010-0297-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Oyewole OO, Akinpelu AO (2011) Developmental pattern of tibio-femoral angle in a cohort of Nigerian children: a preliminary report. Internet J Allied Health Sci Pract 9(4):1–6
- 12.Eng J. Sample size estimation: how many individuals should be studied? Radiology. 2003;227:309–313. doi: 10.1148/radiol.2272012051. [DOI] [PubMed] [Google Scholar]
- 13.Qureshi MA, Soomro MB, Jokhio IA. Normal limits of knee angle in Pakistani children; a photographic study of genu varum and genu valgum. Professional. 2000;7:221–226. [Google Scholar]
- 14.Lin C, Lin S, Huang W, Ho C, Chou Y. Physiological knock-knee in preschool children: prevalence, correlating factors, gait analysis, and clinical significance. J Pediatr Orthop. 1999;19:650. [PubMed] [Google Scholar]
- 15.Abdel Rahman SA, Badhdah WA. Normal development of the tibiofemoral angle in Saudi children from 2 to 15 years of age. World Appl Sci J. 2011;12:1353–1361. [Google Scholar]
- 16.Qureshi MA, Soomro MB, Jokhio IA. Knee angle development in Karachi children. A clinical assessment by measuring tibial length and intercondylar or intermalleolar distance. Professional. 2000;7:482–491. [Google Scholar]