

Abstract
Hydatid disease caused by Echinococcus granulosus is a common parasitic infection of the liver. Disseminated intra-abdominal hydatid disease may occur following a rupture of the hydatid cyst into the peritoneal cavity producing secondary echinococcosis. Rarely, the cyst may develop de novo in the peritoneal cavity without the involvement of any other intra-abdominal organ. We present a unique case of a 57-year-old man with a primary intra-abdominal hydatid cyst.
KEYWORDS: Hydatid disease, primary intra-abdominal hydatid cyst
INTRODUCTION
Echinococcosis is zoonosis characterized by worldwide distribution. It is caused by the larval stage of Echinococcus granulosus. Humans are the accidental intermediate host by ingestion of eggs, which develop into cysts causing complications and even mortality (4%).[1,2] Common sites include liver (75%) and lung (15%).[1] Peritoneal echinococcosis (13%) is usually secondary. Primary peritoneal echinococcosis is rare.[2] Presentation in the form of disseminated intraperitoneal hydatid disease is extremely rare finding. We report such a presentation where the abdominal cavity is seen to contain multiple hydatid cysts.
CASE REPORT
A 57-year-old nonalcoholic, nondiabetic Muslim male presented with progressively increasing abdominal distension [Figure 1] for 3 months prior to admission along with weight loss and anorexia. On examination, he was vitally stable with pale pallor. Abdominal examination revealed a soft mass of 10 × 8 cm which was tender, mobile, and cystic in consistency and was palpable in the epigastrium and right hypochondrium. Soft irregular masses were also felt in the umbilical and hypogastric region. There was presence of fluid thrill but no shifting dullness or organomegaly could be elicited. Hematological tests showed a slight anemia and a mild increase in the eosinophil count (3%). All other laboratory tests including liver function tests were within normal limits except for a positive test for antibodies against E. granulosus. The contrast enhanced computed tomography (CECT) scan of the abdomen revealed multiple well-defined septate cysts throughout the abdomen [Figure 2a]. Ultrasonography of the abdomen showed a normal liver with multiple intraperitoneal cysts [Figure 2b]. There was no contrast enhancement and pericystic invasion of cysts. No other lesion was demonstrable in any organ system. The patient underwent operation. Operative findings included multiple hydatid cysts [Figure 3] of about 1–2 cm in diameter in the whole abdominal and pelvic cavity. The mother cyst was seen in the transverse colon. Postoperatively, he received praziquantel and albendazole for 2 weeks and albendazole was continued for 6 months. On 1-year follow-up, he was fine without any sequelae.
Figure 1.

Patient presenting with generalized abdominal swelling
Figure 2.
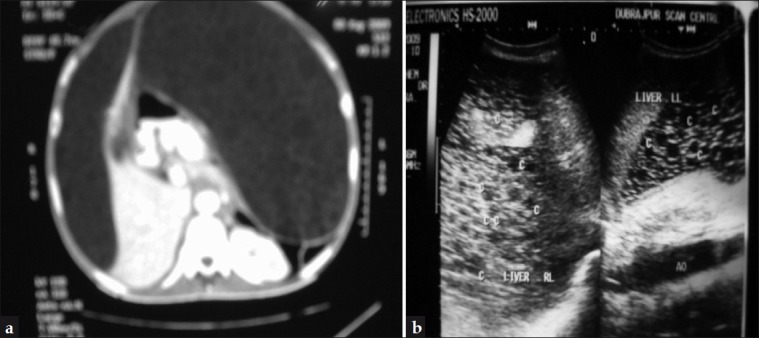
(a) Contrast-enhanced computed tomography scan of the abdomen showing a normal liver, spleen with the whole of the peritoneal cavity replaced by multiple hydatid cysts. (b) Ultrasonography showing a normal liver with multiple intraperitoneal cysts
Figure 3.

Excised hydatid cysts
DISCUSSION
Although hydatid cysts are known to affect the liver and lung commonly, they can also be seen in the peritoneal cavity. Cysts in the peritoneal cavity account for 10–16% of the cases in the literature and mainly result from the rupture of concomitant liver cysts.[3] Primary peritoneal echinococcosis accounts for 2% of all abdominal hydatidosis.[2] Dissemination occurs either by lymphatic[4] or systemic circulations.[5] Clinical manifestations are due to the mass effect of the enlarging abdominal cysts. Diagnosis is confirmed by radioimaging studies (abdominal sonography/computed tomography) complemented with serological tests (complement fixation tests, indirect hemagglutination test and ELISA).[6,7] The principle treatment of hydatid cysts is surgical. However, pre- and postoperative courses of albendazole and praziquantel should be considered in order to sterilize the cyst, decrease the chance of anaphylaxis, and to reduce the recurrence risk postoperatively and to decrease the tension in the cyst wall thus reducing the risk of spillage during surgery.[8,9] The surgical procedure should be customized to each patient depending on the size, location, and complications of each cyst. Intraoperatively, the use of hypertonic saline or 0.5% silver nitrate before opening the cavities tends to kill the daughter cysts and therefore prevent further spread and anaphylactic reaction.[8,9]
A recurrence rate of 2%[9] and survival rate of 95% have been reported in patients undergoing operative intervention.[9] The efficacy of albendazole as the sole medical therapy results in successful treatment in upto 40% of cases.[8,9]
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Babu KS, Goel D, Prayaga A, Rao IS, Kumar A. Intraabdominal hydatid cyst: a case report. Acta Cytol. 2008;52:464–6. doi: 10.1159/000325554. [DOI] [PubMed] [Google Scholar]
- 2.Singh RK. A case of disseminated abdominal hydatidosis. J Assoc Physicians India. 2008;56:55. [PubMed] [Google Scholar]
- 3.Prousalidis J, Tzardinoglou K, Sgouradis L, Katsohis C, Aletras H. Uncommon sites of hydatid disease. World J Surg. 1998;22:17–22. doi: 10.1007/s002689900343. [DOI] [PubMed] [Google Scholar]
- 4.Iuliano L, Gurgo A, Polettini E, Gualdi G, De Marzio P. Musculoskeletal and adipose tissue hydatidosis based on the iatrogenic spreading of cystic fluid during surgery: Report of a case. Surg Today. 2000;30:947–9. doi: 10.1007/s005950070052. [DOI] [PubMed] [Google Scholar]
- 5.Astarcioglu H, Kocdor MA, Topalak O, Terzi C, Sokmen S, Ozer E. Isolated mesosigmoidal hydatid cyst as an unusual cause of colonic obstruction: Report of a case. Surg Today. 2001;31:920–2. doi: 10.1007/s005950170036. [DOI] [PubMed] [Google Scholar]
- 6.Lim JH. Parasitic diseases in the abdomen: imaging findings. Abdom Imaging. 2008;33:130–2. doi: 10.1007/s00261-007-9323-0. [DOI] [PubMed] [Google Scholar]
- 7.Yang YR, Craig PS, Vuitton DA, Williams GM, Sun T, Liu TX, et al. Serological prevalence of echinococcosis and risk factors for infection among children in rural communities of southern Ningxia, China. Trop Med Int Health. 2008;13:1086–94. doi: 10.1111/j.1365-3156.2008.02101.x. [DOI] [PubMed] [Google Scholar]
- 8.Guidelines for treatment of cystic and alveolar echniococcosis in humans. WHO Informal Working Group on Echinococcosis. Bull World Health Organ. 1996;74:231–42. [PMC free article] [PubMed] [Google Scholar]
- 9.Gourgiotis S, Stratopoulos C, Moustafellos P, Dimopoulos N, Papaxoinis G, Vougas V, et al. Surgical techniques and treatment for hepatic hydatid cysts. Surg Today. 2007;37:389–95. doi: 10.1007/s00595-006-3398-z. [DOI] [PubMed] [Google Scholar]