

Abstract
Given the documented association between paternal alcoholism and negative parenting behaviors, the purpose of this study was to examine longitudinally whether marital satisfaction mediates this relationship. Participants consisted of 197 families (102 without an alcoholic father, 95 with an alcoholic father) who were assessed at three time points: when children were 12, 24, and 36 months old. Results indicated that paternal alcoholism at 12 months was associated with decreased marital satisfaction at 24 months for both mothers and fathers. Marital satisfaction at 24 months in turn was associated with decreases in parental warmth and sensitivity at 36 months. Furthermore, marital satisfaction mediated the association between paternal alcoholism and parental warmth and sensitivity for both mothers and fathers. The implications of these findings for interventions for alcoholic families are discussed.
Keywords: Paternal alcoholism, Parenting, Marital satisfaction
1. Introduction
Research on children of alcoholic fathers has shown that they are at an increased risk for a number of problems including attentional difficulties, impulsivity, and conduct problems during childhood, as well as antisocial behavior and alcohol abuse in adolescence and adulthood (e.g., Chassin, Rogosch, & Barrera, 1991; Johnson, Leonard, & Jacob, 1989; West & Prinz, 1987). Theoretical models of the etiology of alcoholism have discussed the important role that family factors play in linking problematic parental alcohol use to negative child outcomes (e.g., Zucker, 1979; Zucker & Gomberg, 1986). Parental alcoholism is believed to result in disruptions in the family environment, including increased marital conflict, financial strain, social isolation, and overall family system disturbance. This negative family environment in turn is hypothesized to contribute to the development of behavior problems in children and alcohol abuse later on (Jacob & Leonard, 1994).
Parental alcoholism is also believed to negatively affect the quality and quantity of parenting behavior (Jacob & Leonard, 1994). Such inadequate parenting behaviors include lack of affection, high levels of criticism and hostility, lax or inconsistent discipline and a general lack of involvement. Research provides support for these assertions: studies have shown that paternal alcoholism is associated with higher levels of parental aggravation, parent–child conflict, and negative affect as well as lower parental sensitivity, positive affect, and verbalizations with young children (e.g., Chassin, Curran, Hussong & Colder, 1996; Chassin, Pillow, Curran, Molina, & Barrera, 1993; Eiden, Chavez, & Leonard, 1999; Eiden & Leonard, 2000; Eiden, Leonard, Hoyle, & Chavez, 2004; El-Sheikh & Flanagan, 2001). Paternal alcoholism also affects expressions of warmth and sensitivity. For example, Eiden et al. (1999) found that father's alcoholism was associated with lower paternal sensitivity and positive affect cross-sectionally in a sample of 12-month old infants. They also found that father's alcoholism was associated with lower verbalizations and higher negative affect among fathers. Furthermore, Eiden, Edwards, and Leonard (2007) found that paternal alcohol use when children were 12 months old predicted lower maternal and paternal warmth and sensitivity when children were 2 years of age. That paternal alcoholism is associated with lower levels of parental warmth and sensitivity is important given that these behaviors are believed to be central to competent parenting and have important implications for child development (Grych, 2002). Research has shown that parental warmth longitudinally predicts children's effortful control (a temperamental characteristic contributing to emotion regulation) which in turn predicts low levels of externalizing behaviors (Eisenberg, Zhou, Spinrad, Valiente, Fabes, & Liew, 2005). Furthermore, warm sensitive parenting is also important for the development of emotional expressivity (Eisenberg, Zhou, Losoya, Fabes, & Shepard, 2003).
Why might paternal alcohol use be associated with lower parental warmth and sensitivity? One reason could be because it negatively affects the relationship between mothers and fathers. According to Jacob and Leonard (1994), the marital relationship is one pathway linking paternal alcoholism to negative parenting behaviors. Partner alcoholism is believed to result in increases in marital conflict and overall marital dissatisfaction and research provides support for this. Studies have shown that men who are frequently drunk are more likely to be verbally and physically violent towards their partners (Coleman & Straus, 1986; Hutchinson, 1999; Kantor Kaufman & Straus, 1989). In addition, clinical outcome research has shown that treatment for alcohol dependence is associated with decreases in intimate partner violence (O'Farrell & Choquette, 1991; Stuart, Ramsey, Moore, Kahler, & Farrell, 2003). Other studies examining marital satisfaction among alcoholics and their partners have shown that partner alcoholism is associated with decreased marital satisfaction for both husbands and wives (e.g., Jacob & Leonard, 1992; Leonard & Jacob, 1997; McLeod, 1993; O'Farrell & Birchler, 1987; Tubman, 1991). For example, O'Farrell and Birchler (1987) compared couples with an alcoholic husband, maritally conflicted couples, and normal control couples. Findings showed that alcoholic couples had significantly lower levels of marital satisfaction compared to happily married couples. Furthermore, alcoholic couples did not differ significantly from maritally distressed couples in marital satisfaction. Studies using continuous measures of alcohol consumption and alcohol problems have also found significant negative correlations between alcohol problems or heavy use and marital satisfaction (e.g., Leonard & Roberts, 1998, Leonard & Senchak, 1993; Zweben, 1986). That the marital relationship can be negatively affected by a partner's alcohol use has important implications for the quality of parent–child interactions (Belsky, 1984; Erel & Burman, 1995; Grych, 2002).
When parents are in satisfying and supportive marital relationships, it is believed that they will be more available and respond more sensitively to the needs of their children. Alternatively, when partners are dissatisfied with their relationship, the resulting negativity may transfer to relationships with their children (Erel & Burman, 1995; Grych, 2002). Support for this `spillover hypothesis' comes from studies which have shown that increased marital quality is associated with positive parenting behaviors, including parental warmth and sensitivity (Bond & McMahon, 1984; Bonds & Gondoli, 2007; Cox, Owen, Lewis, & Henderson, 1989; Easterbrooks & Emde, 1988; Goldberg & Easterbrooks,1984; Harrist & Ainslie, 1998; Jouriles, Pfiffner, & O'Leary, 1988). For example, Cox et al. (1989) examined marital adjustment and parenting in a sample of couples with a 3-month old infant. Results showed that mothers in close and confiding relationships with their partners were warmer and more sensitive with their children and fathers in close and confiding relationships held more positive attitudes toward their infants. These effects were found even after controlling for parents' psychological adjustment. In another study, Easterbrooks and Emde (1988) found that observed harmony between parents was associated with positive affect sharing, physical affection and expressions of approval during interactions with their children. Importantly, these researchers noted that the marital relationship may be particularly important during challenging developmental periods such as the transition to parenthood and early toddlerhood. As such, any disruptions in marital quality that result from parental drinking may be important to document during these critical stages of development.
Given that paternal alcoholism is associated with decreased relationship quality for both husbands and wives, which in turn is associated with lower parental warmth and sensitivity, might relationship quality mediate the association between paternal alcoholism and parenting? Recent research has begun to examine this. Keller, Cummings, Davies, and Mitchell (2008) examined the association between parental problem drinking, family functioning and child development longitudinally in a community sample of families with kindergarten aged children. Results showed that paternal problem drinking was associated with greater marital conflict one year later, which in turn was associated with decreased parental warmth. Marital conflict was also associated with increased parental psychological control. This study is noteworthy in that it documents the important mediating role that the marital relationship plays in linking parental drinking to negative parenting behaviors. Moreover, it examined these pathways longitudinally and focused on more complex family processes than previous research studies. However, the parenting measures were aggregated across mothers and fathers. Thus, the individual effects of paternal alcoholism on parenting could not be determined for each parent separately. Doing so would be important given that paternal alcoholism may affect mothers' and fathers' parenting behaviors in different ways. Moreover, some evidence suggests that the association between marital satisfaction and parenting may be stronger for fathers than for mothers (Belsky, Gilstrap, & Rovine, 1984; Belsky & Volling, 1987). Another limitation of the Keller et al. (2008) study is that it did not control for parents' co-occurring psychopathology, in particular depressive symptomatology, which is known to be positively associated with parental alcoholism (e.g., Eiden & Leonard, 2000; Homish, Leonard, & Kearns-Bodkin, 2006; Roberts & Leonard, 1998) and negatively associated with marital satisfaction (see Beach, Sandeen, & O'Leary, 1990) and positive parenting behaviors (e.g., Jameson, Gelfand, Kulcsar, & Teti,1997; Lyons-Ruth, Wolfe, Lyubchik, & Steingard, 2002; Rosenblum, Mazet, & Benony, 1997).
The current study examined the longitudinal association between paternal alcoholism and parental warmth and sensitivity and the role of marital satisfaction as a potential mediator of this relationship in a sample of parents and their infant children. This study addressed some of the aforementioned limitations by examining these associations separately for mothers and fathers while controlling for parental symptoms of depression. Families in which the father met the criteria for alcohol abuse and/or dependence and families in which neither partner met such criteria were assessed at three time periods one year apart: when infants were 12, 24, and 36 months old. It was hypothesized that fathers' diagnostic status (alcoholic vs. not) at 12 months would be longitudinally predictive of decreased marital satisfaction at 24 months and that this in turn would be predictive of decreased warmth and sensitivity at 36 months. Furthermore, it was believed that these associations would continue to be significant after controlling for prior levels of parental depression (see Fig. 1).
Fig. 1.
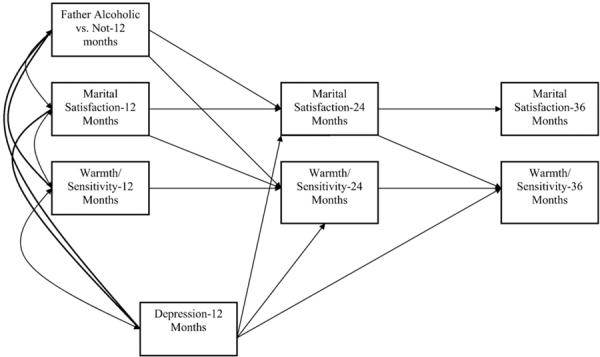
Hypothesized path model predicting marital satisfaction at 24 months as a mediator between paternal alcoholism at 12 months and warmth/sensitivity at 36 months.
2. Method
2.1. Participants
The participants were 197 families with 12 month old infants at recruitment (96 girls and 101 boys) who volunteered for an ongoing longitudinal study of parenting and infant development. Families were classified as being in one of two major groups: the nonalcoholic group consisting of parents with no or few current alcohol problems (n=102), and the father alcoholic group (n=95). Ninety-five percent of the mothers were Caucasian, 4% were African-American, and 2% were Hispanic or Native-American. Similarly, 90% of fathers were Caucasian, 7% were African-American, and 3% were Hispanic or Native-American. The majority of the mothers had a post high school education such as an associate or vocational degree (29%) or were college graduates (27%). Two percent had not graduated from high school. The educational level of the fathers was similar, with 26% receiving a college degree and 21% receiving some post high school education. Only 3% had not graduated from high school. All of the mothers were residing with the father of the infant in the study at the time of recruitment. Eighty-eight percent of the participants were married to each other, 10% had never been married, and 2% had previously been married. Mothers' ages ranged from 20 to 41 years (M=30.8, SD=4.40) and fathers' ages ranged from 21 to 58 years (M=33.09, SD=5.89). Average family income for participating families was about US $43,000.
2.2. Procedures
The names and addresses of these families were obtained from New York State birth records for Erie County. These birth records were pre-selected to exclude families with premature (gestational age of 35 weeks or lower), or low birth weight infants (birth weight of less than 2500 g), maternal age of less than 19 or greater than 40 at the time of the infant's birth, plural births (e.g., twins), and infants with congenital anomalies, palsies, or drug withdrawal symptoms. Introductory letters were sent to a large number of families (n=9457) who met these basic eligibility criteria. Each letter included a form that all families were asked to complete and return. Approximately 25% of these families completed the form and of these, 2285 replies (96%) indicated an interest in the study. Respondents were compared to the overall population with respect to information collected on the birth records. These analyses indicated a slight tendency for infants of responders to have higher Apgar1 scores (M=8.97 vs. 8.94 on a scale ranging from 1 to 10), higher birth weight (M=3516 vs. 3460 g), and a higher number of prenatal visits (M=10.50 vs.10.31). Responders were also more likely to be Caucasian (88% of total births vs. 91% of responders), have higher educational levels, and have a female infant. These differences were significant given the very large sample size, even though the size of the differences was generally small (Cohen's d>.22 in all analyses).
Parents who indicated an interest in the study were screened by telephone with regard to sociodemographic characteristics and further eligibility criteria. Initial inclusion criteria required that both parents were cohabiting since the infant's birth, the target infant was the youngest child in the family and did not have any major medical problems, the mother was not pregnant at the time of recruitment, there were no mother-infant separations of over a week's time, and the biological parents were the primary caregivers. These criteria were important to control because each of these has the potential to markedly alter parent-infant interactions. Additional inclusion criteria were utilized to minimize the possibility that any observed infant behaviors could be the result of prenatal exposure to drugs or heavy alcohol use. These additional criteria were that there could be no maternal drug use during pregnancy or the past year except for mild marijuana use (no more than twice during pregnancy), the mother's average daily ethanol consumption was.50 oz or less and she did not engage in binge drinking (5 or more drinks per occasion) during pregnancy. During the phone screen, mothers were administered the Family History Research Diagnostic Criteria for alcoholism with regard to their partners' drinking (RDC; Andreasen, Rice, Endicott, Reich, & Coryell, 1986) and fathers and mothers were screened with regard to their alcohol use, problems, and treatment.
Families meeting the basic inclusion criteria were provisionally assigned to one of two groups (nonalcoholic and father alcoholic) on the basis of parental phone screens, with final group status assigned on the basis of both the phone screen and questionnaires administered after the family began the study. Mothers in the nonalcoholic group scored below 3 on an alcohol screening measure (TWEAK; Chan, Welte, & Russell, 1993), were not heavy drinkers (average daily ethanol consumption<1.00 oz), did not acknowledge binge drinking, and did not meet DSM-IV criteria for abuse or dependence. Fathers in the nonalcoholic group did not meet RDC criteria for alcoholism according to maternal report, did not acknowledge having a problem with alcohol, had never been in treatment, and had alcohol related problems (e.g., work, family, legal) in fewer than two areas in the past year and three areas in their lifetime (according to responses on a screening interview based on the University of Michigan Composite Diagnostic Index, UM-CIDI; Anthony, Warner, & Kessler, 1994). A family could be classified in the father alcoholic group if the mothers met nonalcoholic status and the father met any one of the following three criteria: (1) the father met RDC criteria for alcoholism according to maternal report; (2) he acknowledged having a problem with alcohol or having been in treatment for alcoholism, was currently drinking, and had at least one alcohol-related problem in the past year; or (3) he indicated having alcohol-related problems in three or more areas in the past year or met DSM-IV criteria for abuse or dependence in the past year.
Families were assessed at multiple time points (12, 18, 24, and 36 months). At each age, extensive observational assessments with both parents were conducted. Parents also completed a battery of self-report questionnaires. Assessments were conducted over the course of three visits at each age with mother-infant observations conducted at the first visit followed by a developmental assessment at the second visit, then father-infant observations at the third visit. The current study focused on the 12, 24, and 36 month assessments. Families were paid for their participation: $150 for the 12 month assessment, $200 for the 24 month assessment, and $250 for the 36 month assessment.
2.3. Measures
2.3.1. Parental alcohol group status
Although parental alcohol abuse and dependence problems were partially assessed from the screening interview, self-report versions with more detailed questions were used to enhance the alcohol data and check for consistent reporting. The UM-CIDI interview (Anthony et al., 1994; Kessler, McGonagle, Zhao, Nelson, & Hughes, 1994) was used to assess alcohol abuse and dependence. Several questions were reworded to inquire as to “how many times” a problem had been experienced, as opposed to whether it happened “very often.” DSM-IV criteria for alcohol abuse and dependence diagnoses for current alcohol problems (in the past year) were used to assign final diagnostic group status. For abuse criteria, recurrent alcohol problems were described as those occurring at least 3–5 times in the past year or 1–2 times in three or more problem areas. The UM-CIDI was also used to derive continuous measures of the number of alcohol-related abuse and dependence symptoms in the past year. We used a quantity-frequency index (QFI) of alcohol use adapted from Cahalan, Cisin, and Crossley (1969) to obtain a measure of average daily ethanol intake for both parents. Finally, two measures of heavy drinking were obtained. The first indicated the frequency of getting drunk, the second indicated the frequency of drinking 5 or more drinks on a single occasion. As described above, families were placed in one of two groups on the basis of phone screen and questionnaire data: (1) the nonalcoholic group and (2) the father alcoholic group.
2.3.2. Marital satisfaction
Marital satisfaction was assessed using the Marital Adjustment Test (MAT; Locke & Wallace, 1959). The MAT is a widely used measure of marital satisfaction. It has been found to discriminate distressed from non-distressed marriages in numerous studies and has well-established concurrent and predictive validities (O'Leary & Turkewitz, 1978). Scores on the MAT for all three assessments for the entire sample ranged from 7–149 (mothers: M=100.87, SD=26.44 at 12 months; M=99.58, SD=28.93 at 24 months; M=99.56, SD=30.07 at 36 months; fathers: M=102.33, SD=24.08 at 12 months; M=103.56, SD=25.84 at 24 months; M=103.25, SD=27.96 at 36 months). Internal consistency (Cronbach's alpha) in the present study was .77 for mothers and .72 for fathers.
2.3.3. Parental warmth and sensitivity
At each of the three assessments, parents were asked to interact with their children as they normally would at home for 10 min in a room filled with toys. Mother–child and father–child interactions were conducted separately. At the 12 and 24 month assessments, the free-play interactions were coded using a collection of global five-point rating scales developed by Clark, Musick, Scott, and Klehr (1980). These scales have been found to be applicable for children ranging in age from 2 months to 5 years (Clark, 1999; Clark et al., 1980). Composite measures of maternal and paternal warmth/sensitivity were derived from these scales, yielding two composite scales, one for mothers and one for fathers at each age. The warmth/sensitivity composite included items such as expressed positive affect, positive involvement, responsiveness, reading child cues, flexibility, low intrusiveness, and consistency/predictability. Higher scores on these scales indicated high warmth/sensitivity. The internal consistency (Cronbach's alpha) for these composite scales ranged from .90 to .93 for mothers' warmth/sensitivity and .90 to .95 for father's warmth/sensitivity at the 12 and 24 month assessments respectively.
The 36 month parent–infant interactions were coded using the Iowa Family Interaction Rating Scales (Melby, Conger, Book, Rueter, & Lucy, 1998), a global rating system designed to measure the behavioral characteristics of individual parents and children and the quality of behavioral exchanges directed from parent to child and vice versa. The rating scales are designed to measure both verbal and non-verbal behaviors as well as affective aspects of the interaction. The warmth/sensitivity composite at 36 months included items such as positive reinforcement, sensitive child centered behaviors, humor, positive mood, warmth-support, prosocial behaviors, and physical affection. The internal consistency (Cronbach's alpha) for these composite scales was .89 for both mothers and fathers.
Two individuals coded parenting behavior. These individuals held Bachelor's level degrees and had extensive experience in the study of child development and in observational coding of parent–child assessments. The coding of maternal and paternal behavior was alternated between the two coders so that the coder who coded one parent did not code the other parent. The coders were trained on the Clark scales and the Iowa Family Interaction Rating Scales by the second author until they achieved at least 80% reliability. The coders were unaware of group membership and all other data. A minimum of 15% of the observations were selected at random for inter-rater reliability checks. For parent–infant interactions at 12 and 24 months, inter-rater reliability was calculated for 17% of the sample (n=38) and was high, with intraclass correlation coefficients ranging from .80 to .92. Inter-rater reliability was calculated for 15% of the sample with complete observational data at 36 months (n=24)2. Intraclass correlation coefficient was .97 for mothers' warmth/sensitivity and .96 for fathers' warmth/sensitivity.
2.3.4. Parents' depression
Parents' depression was assessed with the Center for Epidemiological Studies Depression Inventory (CESD; Radloff, 1977), a scale designed to measure depressive symptoms in community populations. The CESD is a widely used, self-report, four-point Likert type measure. Parents were asked to report how often they experienced 20 depressive symptoms (e.g., poor appetite, feeling sad, inability to concentrate) during the past week with responses including rarely or none, some or a little of the time (1–2 days), occasionally or a moderate amount of the time (3–4 days), or most or all of the time (5–7 days). The scale has high internal consistency (Radloff, 1977), and strong test–retest reliability (Boyd, Weissman, Thompson, & Myers, 1982; Ensel, 1982). Internal consistency in the present study was .90 for mothers and .87 for fathers. Scores on the CES-D ranged from 0 to 37 for both parents (M=7.62, SD=6.87 for fathers, M=8.35, SD=7.22 for mothers).
3. Results
3.1. Missing data and data analytic approach
As would be expected of longitudinal studies involving multiple family members, there were incomplete data for some participants at one or more of the three assessments. Although all 197 families provided complete self-report data at the 12 month assessment, 7 families had missing data for the observational indices of parenting (2 mothers and 5 fathers), primarily due to technical difficulties with the recording equipment. One-hundred eighty-eight mothers and 185 fathers provided complete data at the 24 month visit. One-hundred seventy mothers and 166 fathers provided complete data at the 36 month visit. There were no group differences between families with missing vs. complete data on the parenting variables. There were group differences between families with missing vs. complete data at the 24 and 36 month assessments on marital satisfaction. Mothers who had missing data at the 24 month assessment had lower marital satisfaction scores compared to mothers who had complete data at this assessment (M=85.56, SD=26.07 and M=102.23, SD=26.11 respectively); fathers who had missing data at the 24 month assessment had lower marital satisfaction scores compared to fathers who had complete data at this assessment (M=90.62, SD=17.45 and M=103.37, SD=24.35 respectively). Fathers who had missing data at the 36 month assessment also had lower marital satisfaction scores compared to fathers who had complete data at this assessment (M=94.85, SD=26.34 and M=103.95, SD=23.34 respectively). Mothers who had missing data at 36 months had higher depression scores compared to mothers who had complete data at this assessment (M=10.89, SD=8.72 and M=7.80, SD=6.76 respectively). Finally, mothers who had missing data at 36 months had higher scores on the quantity/frequency index of alcohol use compared to mothers who had complete data at this assessment (M=.15, SD=.21 and M=.08, SD=.11 respectively). Therefore, those who completed the follow up assessments at 24 and 36 months tended to be more satisfied in their marriages compared to those who did not complete the follow up assessments. Also, wives with complete data at the 36 month assessment tended to be less depressed and had lower alcohol use compared to wives who had missing data at this assessment.
Structural equation modeling (SEM) was used to test the conceptual model depicted in Fig. 1. SEM is a collection of statistical techniques that allows researchers the ability to examine a set of relationships between one or more independent variables and one or more dependent variables. Independent variables can be either continuous, discrete or both (Ullman, 2001). SEM is similar to multiple regression, but with SEM more complex and multidimensional relationships can be examined. Furthermore, SEM is the only analysis that allows complete testing of all the hypothesized relationships simultaneously. For this reason, SEM was chosen as the analytic strategy for the current investigation (for a comprehensive discussion of SEM see Hoyle, 1995; Kline, 1998).
All SEM analyses were conducted using Mplus (Verson 4.0; Muthén & Muthén, 1998–2006). Several different fit indices were included to evaluate model fit, including the comparative fit index (CFI), the root mean square error of approximation (RMSEA), the Tucker-Lewis index (TLI), and the standardized root mean square residual (SRMR). Fit indices were evaluated based on the recommendations made by Hu and Bentler (1999); specifically cutoff values close to .95 for the TLI and CFI, cutoff values close to .06 for the RMSEA, and cutoff values close to .08 for the SRMR indicate good fitting models. Full-information maximum likelihood (FIML) was used to estimate parameters in model testing to reach an analysis sample size of 197 for the 12, 24, and 36 month data. Indirect effects for the hypothesized association between parents' alcohol diagnosis and warm/sensitive parenting were calculated using the delta method (Sobel, 1982).
3.2. Demographics and descriptive information
We first examined the associations between marital satisfaction and warm/sensitive parenting and the following demographic variables at 12 months of age: parental education, ethnicity, age, and income. Paternal education was consistently associated with paternal parenting across time, with correlations ranging from r=.16 to r=.21. Paternal education was also associated with maternal parenting at 36 months (r=.23, p<.05). Maternal age was associated with paternal warmth at 36 months (r=.17, p<.05) and maternal warmth at 12 (r=.20, p<.05) and 36 months (r=.20, p<.05). Paternal age was associated with maternal marital adjustment at 36 months (r=−.18, p<.05). Income was associated with paternal warmth at 24 (r=.15, p<.05) and 36 (r=.18, p<.05) months. A series of analyses were then conducted to determine whether there were any significant differences between the father-alcoholic and the non-alcoholic groups on education, ethnicity, age, and income. There were no significant differences between the two groups on any of these demographic variables. As such, we did not include any of the demographic variables as covariates in our analyses.
Additional analyses comparing the two groups on the dependent variables showed that fathers in the alcoholic group consumed more alcohol and had higher numbers of alcohol symptoms compared to fathers in the non-alcoholic group (see Table 1). Mothers in the alcoholic group did not differ from mothers in the non-alcoholic group in alcohol consumption3. In addition, fathers and mothers in the alcoholic group were significantly more depressed and had lower marital satisfaction at 12, 24, and 36 months compared to fathers and mothers in the non-alcoholic group. Fathers in the alcoholic group displayed less warmth/sensitivity with their children at 24 months than fathers in the non-alcoholic group while mothers in the alcoholic group displayed less warmth/sensitivity with their children at 24 and 36 months compared to mothers in the non-alcoholic group.
Table 1.
Means and standard deviations of major study variables for father alcoholic and non-alcoholic families.
| Variable | Non-alcoholic (n = 102) |
Father-alcoholic (n = 95) |
||
|---|---|---|---|---|
| M | SD | M | SD | |
| Father | ||||
| QFI | .28a | .54 | 1.47b | 1.20 |
| No. of alcohol symptoms | .15a | .40 | 10.92b | 17.23 |
| Depression | 6.35a | 6.25 | 8.97b | 7.27 |
| Marital satisfaction T1 | 107.04a | 23.68 | 97.28b | 23.61 |
| Marital satisfaction T2 | 111.34a | 21.98 | 95.00b | 27.16 |
| Marital satisfaction T3 | 107.83a | 26.45 | 97.86b | 28.88 |
| Warmth/sensitivity T1 | 3.86a | .71 | 3.43a | .77 |
| Warmth/sensitivity T2 | 4.63a | .50 | 4.00b | .76 |
| Warmth/sensitivity T3 | 6.17a | 1.49 | 6.09a | 1.54 |
| Mother | ||||
| QFI | .08a | .12 | .11a | .15 |
| No. of alcohol symptoms | .10a | .53 | .28b | .65 |
| Depression | 7.09a | 6.16 | 9.71b | 8.02 |
| Marital satisfaction T1 | 108.26a | 23.00 | 92.94b | 27.69 |
| Marital satisfaction T2 | 109.64a | 23.61 | 88.97b | 30.33 |
| Marital satisfaction T3 | 109.89a | 22.75 | 87.60b | 33.07 |
| Warmth/sensitivity T1 | 3.80a | .75 | 3.89a | .62 |
| Warmth/sensitivity T2 | 4.58a | .59 | 4.24b | .63 |
| Warmth/sensitivity T3 | 6.47a | 1.54 | 5.98b | 1.49 |
Note: Means with different subscripts are significantly different from each other at the p<.05 level. QFI = quantity/frequency index; Alcohol symptoms = number of alcohol symptoms in the past year. T1 = 12 months, T2 = 24 months, T3 = 36 months.
3.3. Correlational analyses
Zero-order correlations for all variables for mothers and fathers are summarized in Table 2. Father's alcohol diagnosis at 12 months was associated with higher depressive symptoms for both mothers and fathers at 12 months. Father's alcohol diagnosis at 12 months was also associated with lower marital satisfaction for both mothers and fathers at 12, 24, and 36 months. Father's alcohol diagnosis was associated with lower maternal warmth/sensitivity at 24 and 36 months and lower paternal warmth/sensitivityat 12 and 24 months. For mothers, higher depressive symptoms were associated with lower marital satisfaction at 12, 24, and 36 months as well as lower warmth/sensitivity at 12 and 36 months. Higher marital satisfaction at 12 months was associated with higher maternal warmth/sensitivity at 36 months; higher marital satisfaction at 24 months was associated with higher maternal warmth/sensitivity at 24 and 36 months. For fathers, higher depressive symptoms at 12 months were associated with lower marital satisfaction at 12, 24, and 36 months and lower warmth/sensitivity at 12 and 36 months. Higher marital satisfaction at 12 months was associated with higher paternal warmth/sensitivity at 12 and 36 months; higher marital satisfaction at 24 months was associated with higher paternal warmth/sensitivity at 24 and 36 months.
Table 2.
Zero-order correlations of study variables for fathers (top) and mothers (bottom).
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| 1. Paternal alcoholism | .19** | −.20** | −.32** | −.18* | −.23** | −.40** | −.03 | |
| 2. Depression T1 | .18* | −.43** | −.34** | −.37** | −.22** | −.12 | −.17* | |
| 3. Marital satisfaction T1 | −.29** | −.38** | .67** | .66** | .19** | .10 | .18* | |
| 4. Marital satisfaction T2 | −.36** | −.32** | .75** | .66** | .20** | .20** | .21** | |
| 5. Marital satisfaction T3 | −.37* | −.27** | .62** | .70** | .20** | .14 | .23** | |
| 6. Warmth/sensitivity T1 | .02 | −.20** | .10 | .08 | .11 | .32** | .43** | |
| 7. Warmth/sensitivity T2 | −.33** | −.09 | .08 | .23** | .23** | .21** | .43** | |
| 8. Warmth/sensitivity T3 | −.16* | −.21** | .20** | .35** | .28** | .36** | .40** |
Note: T1 = 12 months, T2 = 24 months, T3 = 36 months.
p<.05
p<.01.
3.4. Model testing
Models were tested separately for mothers and fathers. The baseline structural model for mothers included dummy-coded variables for group status (father alcoholic vs. not), marital satisfaction, warmth/sensitivity during parent–infant interactions and depression. In order to examine the longitudinal associations, marital satisfaction and parental warmth/sensitivity were included at each of the three time points (12, 24, and 36 months) to control for concurrent associations among the variables. Given the temporal stability of paternal alcoholism and depression over the three time points these variables were included in the analyses only at Time 1. The baseline model included covariances between exogenous predictors (alcohol diagnosis, marital satisfaction, warm/sensitive parenting and depression). Direct paths were also included from alcohol group status, marital satisfaction and depression at 12 months to marital satisfaction and warmth/sensitivity at 24 months and paths from marital satisfaction and warmth/sensitivityat 24 months to warmth/sensitivityat 36 months. A direct path from depression at 12 months to parenting at 36 months was also included (see Fig. 1).
Results indicated that for mothers this baseline model did not adequately fit the data (χ2 (9)=31.10, p=.00, RMSEA=.11, CFI=.95, TLI=.79, SRMR=.05). Although we hypothesized that marital satisfaction would mediate the association between paternal alcoholism and warm/sensitive parenting, it was possible that paternal alcoholism would still have a direct effect on maternal parenting behavior, which is consistent with theoretical formulations of the etiology of alcoholism and prior research. Thus, a direct path was added from alcohol group status at 12 months to warmth/sensitivity at 36 months to see if this would improve the fit of the model. Results indicated that this modification did not result in an improved fit: χ2difference (1)=.52, p>.05. As such, this path was dropped from the model. Modification indices suggested the addition of a direct path from warm/sensitive parenting at 12 months to warm/sensitive parenting at 36 months would improve model fit. We then ran a third model which included this path and dropped the non-significant paths from marital satisfaction at 12 months to warm/sensitive parenting at 24 months and from depression at 12 months to marital satisfaction at 24 months and warm/sensitive parenting at 24 and 36 months. This model resulted in an improvement in model fit: χ2difference (3)=12.10, p<.05, and fit the data adequately: χ2 (12)=19.00, p=.09, RMSEA=.06, CFI=.98, TLI=.95, SRMR=.03 (see Fig. 2).
Fig. 2.
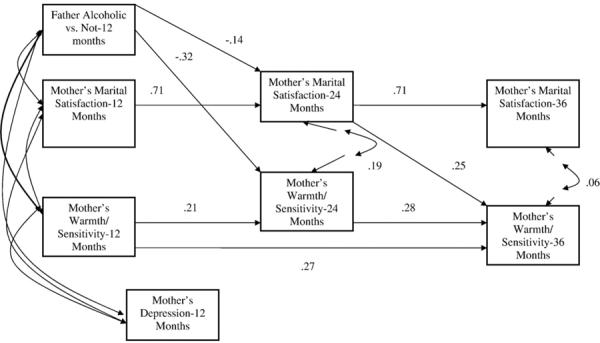
Structural model for mothers. Note: Numbers are beta weights. All beta weights significant at p<.05; χ2 (12)=19.00, p=.09, RMSEA=.06, CFI=.98.
Paternal alcohol diagnosis at 12 months was predictive of mothers' lower marital satisfaction (β=−.14, p<.05) and warmth and sensitivity at 24 months (β=−.32, p<.05). Higher marital satisfaction at 24 months was predictive of higher warmth and sensitivity at 36 months (β=.25, p<.05). Finally, calculation of the indirect effects with standard errors calculated using the delta method (Sobel, 1982) showed that marital satisfaction at 24 months mediated the association between paternal alcoholism at 12 months and warm/sensitive parenting at 36 months (z=−2.37, p<.05).
We evaluated the structural model for fathers in a similar fashion. The initial baseline was identical to that tested initially for mothers (see Fig. 1). Results indicated that for fathers this baseline model did not adequately fit the data: χ2 (9)=58.04, p=.00, RMSEA=.17, CFI=.88, TLI=.51, SRMR=.06. Although we hypothesized that marital satisfaction would mediate the association between paternal alcoholism and warm/sensitive parenting, it was possible that paternal alcoholism would still have a direct effect on maternal parenting behavior, which is consistent with theoretical formulations of the etiology of alcoholism and prior research. Thus, similar to the models tested for mothers, we added a direct path from alcohol group status at 12 months to warmth/sensitivity at 36 months. There was a significant improvement in model fit: χ2difference (1)=8.41, p<.05, although several of the overall fit indices were still inadequate (RMSEA=.16; CFI=.90; TLI=.51). Modification indices suggested the addition of a direct path from marital satisfaction at 12 months to marital satisfaction at 36 months. The addition of this path (and the deletion of the following non-significant paths: from marital satisfaction at 12 months to warm/sensitive parenting at 24 months and from depression at 12 months to marital satisfaction at 24 months and warm/sensitive parenting at 24 and 36 months) resulted in a significant improvement in model fit: χ2difference (4)=36.66, p<.05. Moreover, this model adequately fit the data: χ2 (11)=21.38, p=.03, RMSEA=.07, CFI=.97, TLI=.92, SRMR=.05 (see Fig. 3).
Fig. 3.
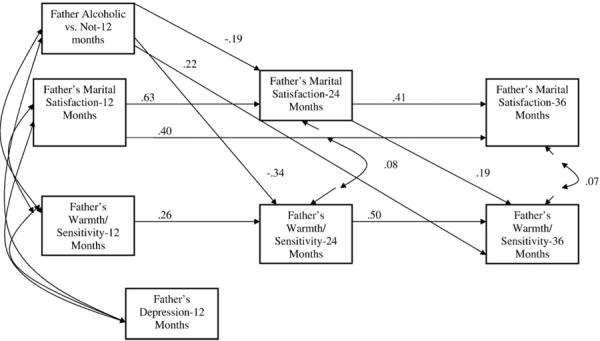
Structural model for fathers. Note: Numbers are beta weights. All beta weights significant at p<.05. χ2 (11)=21.38, p=.03, RMSEA=.07, CFI=.97.
Paternal alcohol diagnosis at 12 months was predictive of fathers' lower marital satisfaction (β=−.19, p<.05) and warmth and sensitivity at 24 months (β=−.34, p<.05). Paternal alcohol diagnosis was also associated with warmth and sensitivity at 36 months, although in the direction opposite to what was expected; paternal alcohol diagnosis was predictive of higher warmth and sensitivity at 36 months (β=.22, p<.05). Higher marital satisfaction at 24 months was predictive of higher warmth and sensitivity at 36 months (β=.19, p<.05). Finally, using the formula proposed by Sobel (1982), results indicated that the indirect effect of paternal alcoholism at 12 months and parenting at 36 months through marital satisfaction at 24 months was significant (z=−2.15, p<.05).
4. Discussion
Given the documented association between paternal alcoholism and parental warmth and sensitivity, the purpose of the current study was to examine one possible mechanism linking the two. To date, no studies have examined these variables longitudinally in a younger sample of children of alcoholics. Such research would be important as it would advance the growing literature on paternal alcoholism and negative parenting during the earliest stages of child development by providing one possible explanation for the association between the two. Findings showed that one pathway is via marital satisfaction: for both fathers and mothers, paternal alcoholism at 12 months was associated with lower levels of marital satisfaction at 24 months which in turn was associated with lower parental warmth and sensitivity at 36 months. The current findings add to the literature on paternal alcoholism and negative parenting by highlighting the important role that the marital relationship can play.
Consistent with theoretical accounts and previous research studies, paternal alcoholism was associated with decreased marital satisfaction for both husbands and wives. This may be because of the stresses of husband's alcoholism on his wife. However, because wives were not heavy drinkers, this might also reflect the impact of incongruent drinking patterns (i.e., patterns in which one partner drinks and the other does not, Homish & Leonard, 2005, 2007). Taken together, these findings provide additional support to the growing literature on the negative effects that partner alcoholism can have on the marital relationship.
Overall, marital dissatisfaction was associated with less warm and sensitive parenting, cross-sectionally and longitudinally for both mothers and fathers. These findings provide support for the `spillover hypothesis' in that negative mood, affect or behavior experienced in the marital relationship transfers to the parent–child relationship. The decreased satisfaction parents experience shifts to the parent–child relationship, resulting in inconsistent discipline strategies and less optimal parenting techniques (Easterbrooks & Emde, 1988). Interestingly, previous research has found a positive association between marital interaction and parental involvement when children were 3 months and 9 months old for fathers, but not for mothers (Belsky et al., 1984). Consistent with these findings, in the current study marital satisfaction was associated with warm/sensitive parenting at each time point (12, 24, and 36 months of child age) for fathers. However, for mothers marital satisfaction was associated with warm/sensitive parenting only at the 24 and 36 month assessments. This suggests that the marital relationship may become more relevant for parenting for mothers as children get older and the developmental demands placed on parents increase. During such times, additional partner support is necessary in order to deal with these demands. Whether the marital relationship continues to be important for parenting as children get older should be explored in future research.
For mothers, the indirect effect of paternal alcoholism on warmth and sensitivity through marital satisfaction was significant. When the direct effect of father's alcoholism on 36 month maternal warmth and sensitivity was included in the model, the fit of the model did not improve. Furthermore, this path was not significant. Thus, marital satisfaction mediated the association between paternal alcoholism and warmth and sensitivity. For fathers, the indirect effect of paternal alcoholism on warmth and sensitivity through marital satisfaction was also significant. However, when the direct effect of paternal alcoholism on warmth and sensitivity was included in the model, the fit of the model significantly improved. Thus, marital satisfaction partially mediated the association between father's alcoholism and negative parenting. Interestingly, the association between father's alcoholism and warmth and sensitivity was significant and in the opposite direction to what was predicted: paternal alcoholism predicted increases in paternal warmth and sensitivity at 36 months. However at the correlational level paternal alcoholism was not associated with negative parenting at 36 months. Thus, it is likely that a suppression effect was occurring with fathers.
It is interesting to note that for mothers, improvement in the model fit was obtained when a direct path was included from warm/sensitive parenting at 12 months to warm/sensitive parenting at 36 months. A similar pattern was obtained for fathers, but for marital satisfaction instead of warm/sensitive parenting (inclusion of a direct path from marital satisfaction at 12 months to marital satisfaction at 36 months improved model fit). One reason for this could be because of developmental changes that tend to occur in parenting and child behavior during the second year of life (e.g., Demick, 2002; Kopp, 1992). The 2 year mark is seen as a time of intense parent–child conflict and negotiation; a period when there is a shift in parenting from caretaking and nurturing to handling of authority issues and limit-setting. In addition, during this time temper tantrums tend to peak and then decline between the ages 2 and 3 (Kopp, 1992). The changes that occur in the parent–child relationship likely affect the marital relationship as well. Such changes may explain why warm/sensitive parenting and marital satisfaction at 24 months did not fully account for the variance of warm/sensitive parenting and marital satisfaction for mothers and fathers respectively at 36 months.
The current findings were obtained even after controlling for parental depression. Depression has consistently been shown to be associated with parental alcoholism (e.g., Eiden & Leonard, 2000; Homish et al., 2006), marital satisfaction (e.g., Beach et al., 1990), and parenting (e.g., Jameson et al., 1997; Rosenblum et al., 1997). Consistent with these previous research findings, at the correlational level depression was associated with paternal alcoholism, lower marital satisfaction and lower warmth/sensitive parenting for both mothers and fathers. However, at the multivariate level, depression did not predict marital satisfaction at 24 months or parenting at 24 or 36 months for both mothers and fathers. Such findings are similar to other studies conducted with this sample (e.g., Eiden et al., 2007; Eiden, Leonard, Hoyle, & Chavez, 2004). One possible reason for this could be because of the largely sub-clinical nature of depression reported in the current sample. Studies that have reported strong associations between parental depression and parenting behavior have recruited participants with high levels of depression (e.g., Jameson et al.,1997). In the current investigation, depression levels for both alcoholic and non-alcoholic groups were relatively low. Given these low levels, it is not surprising that depression did not have any longitudinal associations with parenting and marital functioning.
Knowing that marital satisfaction acts as a mediator for mothers and as a partial mediator for fathers between paternal alcoholism and warm/sensitive parenting has important clinical implications. Interventions that target the marital dyad can help offset the negative impact that fathers' drinking can have on parent–child relationships. Indeed, researchers and clinicians have implemented behavioral couple therapy (BCT) with substance abusing individuals. A great deal of research has been conducted documenting its effectiveness (see Fals-Stewart, O' Farrell, Birchler, Cordova, & Kelley, 2005); findings from these studies have shown that BCT reduces substance use and improves overall family functioning. Moreover, studies have also found that BCT is effective in improving overall relationship functioning (e.g., O'Farrell, Murphy, Stephan, Fals-Stewart, & Murphy, 2004). Other researchers have incorporated parent skills training as an adjunct to treatment for substance abusing parents (e.g., Catalano, Haggerty, Gainey, & Hoppe,1997; Catalano, Haggerty, Fleming, Brewer, & Gainey, 2002). Findings show that such programs improve parenting behaviors and decrease parental substance use, which in turn may help to decrease delinquent behavior in children. The results from the current investigation provide support for incorporating treatments that focus on the marital and parental dyad into interventions for alcoholism. By improving parental functioning either directly or through decreased alcohol use and improved marital quality, the potential risk for negative child outcomes resulting from decreases in warmth and sensitivity, such as externalizing problems, may be lowered.
Although the findings from the current study fill an important gap in the literature, there are several limitations that should be noted. First, the response rate to our open letter of recruitment was slightly above 25%. This raises the possibility that respondents to our recruitment may not have been representative of families with 12-month old infants. Our comparison of respondents with the entire population of birth records suggested that the differences were small with respect to the variables that we could examine. However there could have been significant differences in variables that we could not assess. Thus, although generating our sample from birth records has important advantages over newspaper or clinic-based samples, generalizability of results may be limited to the population of higher functioning families, who may be more likely to respond to open letters of recruitment about participation in research. A second potential limitation was that we chose to focus exclusively on marital satisfaction as our intervening or mediating variable. However, other variables particularly for fathers may also act as additional mechanisms through which paternal alcoholism exerts its effects on negative parenting behaviors. For example, other family effects have been hypothesized to play a role linking parental alcohol problems and disrupted parenting, including sibling interactions, financial strain, social isolation and disruption in normal family routines due to external stresses (Jacob & Leonard, 1994; Zucker & Gomberg, 1986). In addition, other aspects of the marital relationship might also be considered, such as marital conflict and aggression and/or the kinds of disagreements parents have with each other (e.g., child-rearing disagreements, financial disagreements). Future research might explore these additional factors, so that a more comprehensive model of parental alcoholism, family functioning and parenting can be examined.
In addition to examining additional mediators of the paternal alcoholism-warm/sensitive parenting association, future research might also examine whether marital satisfaction still plays a significant role among older children of alcoholics. Also, although the current study focused on paternal alcoholism, future research might also examine alcoholic mothers and whether the same pattern of results holds for couples where the wife is an alcoholic and the husband is not. Another future direction would be to compare the parenting behaviors of couples where both partners are alcoholic with couples who do not engage in problematic alcohol use. Given that patterns of congruent drinking behavior (i.e., where neither partner drinks and/or where both partners engage in problematic drinking behavior) have been shown to be associated with increases in marital satisfaction (e.g., Homish & Leonard, 2007), future research might examine if such increases in marital satisfaction are in turn associated with positive parenting behaviors or if the marital satisfaction-positive parenting association only occurs when neither parent drinks.
The current investigation provides critical new information on the role that the marital relationship plays for families with an alcoholic father. Given the importance of parenting for child development, particularly during infancy and toddlerhood, it becomes essential to delineate how it may be affected by parental alcohol use and marital functioning. The current findings bring us one step closer to fully understanding the negative affects of paternal alcoholism on families.
Acknowledgements
Lorig K. Kachadourian, Research Institute on Addictions, University at Buffalo, State University of New York; Rina D. Eiden, Research Institute on Addictions and Department of Pediatrics, University at Buffalo, State University of New York; Kenneth E. Leonard, Departments of Pediatrics and Psychiatry, University at Buffalo, State University of New York.
This study was made possible by the National Institute on Alcohol Abuse and Alcoholism Grant 1RO1 AA 10042-01A1 and National Institute on Drug Abuse Grant 1 K21DA00231-01A1. We thank parents and children who participated in the study and the research staff who were responsible for conducting and coding numerous assessments with these families.
Footnotes
Apgar tests are typically given within minutes of a baby's delivery. The test is designed to quickly evaluate a newborn's physical condition and to determine whether there is any immediate need for extra medical or emergency care. Scores range from 1–10, with scores higher than 7 indicating that the baby is in relatively good health.
While we followed the common procedures in randomly selecting a minimum of 15% of observations for calculating reliability, a few additional parent–child interactions at 12 and 24 months were inadvertently rated.
Although mothers in the alcoholic group had significantly more alcohol symptoms in the past year compared to mothers in the non-alcoholic group, the overall means for both groups were relatively small and not clinically meaningful.
References
- Andreasen NC, Rice J, Endicott J, Reich T, Coryell W. The family history approach to diagnosis: How useful is it? Archives of General Psychiatry. 1986;43:421–429. doi: 10.1001/archpsyc.1986.01800050019002. [DOI] [PubMed] [Google Scholar]
- Anthony JC, Warner LA, Kessler RC. Comparative epidemiology of dependence on tobacco, alcohol, controlled substances, and inhalants: Basic findings from the National Comorbidity Survey. Experimental and Clinical Psychopharmacology. 1994;2:244–268. [Google Scholar]
- Beach SRH, Sandeen EE, O'Leary KD. Depression in marriage: A model for etiology and treatment. Guilford Press; New York: 1990. [Google Scholar]
- Belsky J. The determinants of parenting: A process model. Child Development. 1984;55:83–96. doi: 10.1111/j.1467-8624.1984.tb00275.x. [DOI] [PubMed] [Google Scholar]
- Belsky J, Gilstrap B, Rovine M. The Pennsylvania Infant and Family Development Project, I: Stability and change in mother–infant and father–infant interaction in a family setting at one, three, and nine months. Child Development. 1984;55:692–705. [PubMed] [Google Scholar]
- Belsky J, Volling BL. Mothering, fathering, and marital interaction in the family triad during infancy: Exploring family system's processes. In: Berman PW, Pedersen FA, editors. Men's transitions to parenthood: Longitudinal studies of early family experience. Lawrence Erlbaum Associates; Hillsdale, NJ: 1987. pp. 37–63. [Google Scholar]
- Bond CR, McMahon RJ. Relationships between marital distress and child behavior problems, maternal personal adjustment, maternal personality, and maternal parenting behavior. Journal of Abnormal Psychology. 1984;93:348–351. doi: 10.1037//0021-843x.93.3.348. [DOI] [PubMed] [Google Scholar]
- Bonds DD, Gondoli DM. Examining the process by which marital adjustment affects maternal warmth: The role of coparenting support as a mediator. Journal of Family Psychology. 2007;21:288–296. doi: 10.1037/0893-3200.21.2.288. [DOI] [PubMed] [Google Scholar]
- Boyd JH, Weissman MM, Thompson WD, Myers JK. Screening for depression in a community sample: Understanding the discrepancies between depression syndrome and diagnostic scales. Archives of General Psychiatry. 1982;39:1195–1200. doi: 10.1001/archpsyc.1982.04290100059010. [DOI] [PubMed] [Google Scholar]
- Cahalan D, Cisin IH, Crossley H. American drinking practices: A national study of drinking, behavior and attitudes [Monograph No.1] Rutgers Center of Alcohol Studies; New Brunswick, NJ: 1969. [Google Scholar]
- Catalano RF, Haggerty KP, Fleming CB, Brewer DD, Gainey RR. Children of substance-abusing parents: Current findings from the Focus on Families project. In: McMahon RJ, Peters R, editors. The effects of parental dysfunction on children. Kluwer Academic/Plenum Publishers; New York: 2002. pp. 179–204. [Google Scholar]
- Catalano RF, Haggerty KP, Gainey RR, Hoppe MJ. Reducing parental risk factors for children's substance misuse: Preliminary outcomes with opiate-addicted parents. Substance Use & Misuse. 1997;32:699–721. doi: 10.3109/10826089709039371. [DOI] [PubMed] [Google Scholar]
- Chan AWK, Welte JW, Russell MAH. Screening for heavy drinking/alcoholism by the TWEAK test. Alcoholism, Clinical and Experimental Research. 1993;17:463. doi: 10.1111/j.1530-0277.1993.tb05226.x. [DOI] [PubMed] [Google Scholar]
- Chassin L, Curran PJ, Hussong AM, Colder CR. The relation of parent alcoholism to adolescent substance use: A longitudinal follow-up study. Journal of Abnormal Psychology. 1996;105:70–80. doi: 10.1037//0021-843x.105.1.70. [DOI] [PubMed] [Google Scholar]
- Chassin L, Pillow DR, Curran PJ, Molina BS, Barrera M. Relation of parental alcoholism to early adolescent substance use: A test of three mediating mechanisms. Journal of Abnormal Psychology. 1993;102:3–19. doi: 10.1037//0021-843x.102.1.3. [DOI] [PubMed] [Google Scholar]
- Chassin L, Rogosch F, Barrera M. Substance use and symptomatology among adolescent children of alcoholics. Journal of Abnormal Psychology. 1991;100:449–463. doi: 10.1037//0021-843x.100.4.449. [DOI] [PubMed] [Google Scholar]
- Clark R. The parent–child early relational assessment: A factorial validity study. Educational and Psychological Measurement. 1999;59:821–846. [Google Scholar]
- Clark R, Musick J, Scott F, Klehr K. The Mothers' Project Rating Scale of Mother–Child Interaction. 1980 Unpublished manuscript. [Google Scholar]
- Coleman DH, Straus MA. Marital power, conflict, and violence in a nationally representative sample of American couples. Violence and Victims. 1986;1:141–157. [PubMed] [Google Scholar]
- Cox MJ, Owen MT, Lewis JM, Henderson BK. Marriage, adult adjustment, and early parenting. Child Development. 1989;60:1015–1024. doi: 10.1111/j.1467-8624.1989.tb03532.x. [DOI] [PubMed] [Google Scholar]
- Demick J. Stages of parental development. In: Bornstein MH, editor. Handbook of parenting, 2nd ed. Being and becoming a parent. vol. 3. Lawrence Erlbaum Publishers; Mahwah, NJ: 2002. pp. 389–413. [Google Scholar]
- Easterbrooks MS, Emde RN. Marital and parent–child relationships: The role of affect in the family system. In: Hinde R, Stevenson-Hinde J, editors. Relationships within families. Oxford University Press; Oxford, England: 1988. pp. 83–103. [Google Scholar]
- Eiden RD, Chavez F, Leonard KE. Parent–infant interactions in alcoholic and control families. Development and Psychopathology. 1999;11:745–762. doi: 10.1017/s0954579499002308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eiden RD, Edwards EP, Leonard KE. A conceptual model for the development of externalizing behavior problems among kindergarten children of alcoholic families: Role of parenting and children's self-regulation. Developmental Psychology. 2007;43:1187–1201. doi: 10.1037/0012-1649.43.5.1187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eiden RD, Leonard KE. Paternal alcoholism, parental psychopathology, and aggravation with infants. Journal of Substance Abuse. 2000;11:17–29. doi: 10.1016/s0899-3289(99)00016-4. [DOI] [PubMed] [Google Scholar]
- Eiden RD, Leonard KE, Hoyle RH, Chavez F. A transactional model of parent–infant interactions in alcoholic families. Psychology of Addictive Behaviors. 2004;18:350–361. doi: 10.1037/0893-164X.18.4.350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eisenberg N, Zhou Q, Losoya SH, Fabes RA, Shepard SA, Murphy BC, et al. The relations of parenting, effortful control and ego control to children's emotional expressivity. Child Development. 2003;74:875–895. doi: 10.1111/1467-8624.00573. [DOI] [PubMed] [Google Scholar]
- Eisenberg N, Zhou Q, Spinrad TL, Valiente C, Fabes RA, Liew J. Relations among positive parenting, children's effortful control, and externalizing problems: A three-wave longitudinal study. Child Development. 2005;76:1055–1071. doi: 10.1111/j.1467-8624.2005.00897.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- El-Sheikh M, Flanagan E. Parental problem drinking and children's adjustment: Family conflict and parental depression as mediators and moderators of risk. Journal of Abnormal Child Psychology. 2001;29:417–432. doi: 10.1023/a:1010447503252. [DOI] [PubMed] [Google Scholar]
- Ensel WM. The role of age in the relationship of gender and marital status to depression. Journal of Nervous and Mental Disease. 1982;170:536–543. doi: 10.1097/00005053-198209000-00004. [DOI] [PubMed] [Google Scholar]
- Erel O, Burman B. Interrelatedness of marital relations and parent–child relations: A meta-analytic review. Psychological Bulletin. 1995;118:108–132. doi: 10.1037/0033-2909.118.1.108. [DOI] [PubMed] [Google Scholar]
- Fals-Stewart W, O'Farrell TJ, Birchler GR, Cordova J, Kelley ML. Behavioral couples therapy for alcoholism and drug abuse: Where we've been, where we are, and where we're going. Journal of Cognitive Psychotherapy. 2005;19:229–246. [Google Scholar]
- Goldberg WA, Easterbrooks MS. Role of marital quality in toddler development. Developmental Psychology. 1984;20:504–514. [Google Scholar]
- Grych JH. Marital relationships and parenting. In: Bornstein MH, editor. Handbook of parenting, 2nd ed. Social conditions and applied parenting. vol. 4. Lawrence Erlbaum Associates; Mahwah, NJ: 2002. pp. 203–225. [Google Scholar]
- Harrist AW, Ainslie RC. Marital discord and child behavior problems: Parent–child relationship quality and child interpersonal awareness as mediators. Journal of Family Issues. 1998;19:140–163. [Google Scholar]
- Homish GG, Leonard KE. Marital quality and congruent drinking. Journal of Studies on Alcohol. 2005;66:488–496. doi: 10.15288/jsa.2005.66.488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Homish GG, Leonard KE. The drinking partnership and marital satisfaction: The longitudinal influence of discrepant drinking. Journal of Consulting and Clinical Psychology. 2007;75:43–51. doi: 10.1037/0022-006X.75.1.43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Homish GG, Leonard KE, Kearns-Bodkin JN. Alcohol use, alcohol problems, and depressive symptomatology among newly married couples. Drug and Alcohol Dependence. 2006;83:185–192. doi: 10.1016/j.drugalcdep.2005.10.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoyle RH. Structural equation modeling: Concepts, issues and applications. Sage; Thousand Oaks, CA: 1995. [Google Scholar]
- Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling. 1999;6:1–55. [Google Scholar]
- Hutchinson IW. Alcohol, fear, and woman abuse. Sex Roles. 1999;40:893–920. [Google Scholar]
- Jacob T, Leonard KE. Sequential analysis of marital interactions involving alcoholic, depressed, and nondistressed men. Journal of Abnormal Psychology. 1992;101:647–656. doi: 10.1037//0021-843x.101.4.647. [DOI] [PubMed] [Google Scholar]
- Jacob T, Leonard KE. Family and peer influences in the development of adolescent alcohol abuse. In: Zucker R, Boyd G, Howard J, editors. Development of alcohol problems: Exploring the bio-psychosocial matrix of riskNIAAA Monograph No. 26. National Institute on Alcohol Abuse and Alcoholism; Rockville, MD: 1994. pp. 123–156. [Google Scholar]
- Jameson PB, Gelfand DM, Kulcsar E, Teti DM. Mother–toddler interaction patterns associated with maternal depression. Developmental Psychopathology. 1997;9:557–590. [PubMed] [Google Scholar]
- Johnson S, Leonard KE, Jacob T. Drinking, drinking styles, and drug use in children of alcoholics, depressives, and controls. Journal of Studies on Alcohol. 1989;50:427–431. doi: 10.15288/jsa.1989.50.427. [DOI] [PubMed] [Google Scholar]
- Jouriles EN, Pffifner LJ, O'Leary SG. Marital conflict, parenting, and toddler conduct problems. Journal of Abnormal Child Psychology. 1988;16:197–206. doi: 10.1007/BF00913595. [DOI] [PubMed] [Google Scholar]
- Kantor Kaufman G, Straus MA. Substance abuse as a precipitant of wife abuse victimizations. American Journal of Drug and Alcohol Abuse. 1989;15:173–189. doi: 10.3109/00952998909092719. [DOI] [PubMed] [Google Scholar]
- Keller PS, Cummings EM, Davies PT, Mitchell PM. Longitudinal relations between parental drinking problems, family functioning, and child adjustment. Developmental Psychopathology. 2008;20:195–212. doi: 10.1017/S0954579408000096. [DOI] [PubMed] [Google Scholar]
- Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, et al. Lifetime and 12 month prevalence of DSM-III-R psychiatric disorders in the United States: Results from the National Comorbidity Survey. Archives of General Psychiatry. 1994;51:8–19. doi: 10.1001/archpsyc.1994.03950010008002. [DOI] [PubMed] [Google Scholar]
- Kline RB. Structural equation modeling. The Guilford Press; New York: 1998. [Google Scholar]
- Kopp CB. Emotional distress and control in young children. In: Eisenberg N, Fabes RA, editors. Emotion and its regulation in early development. Jossey-Bass; San Francisco: 1992. pp. 41–56. [DOI] [PubMed] [Google Scholar]
- Leonard KE, Jacob T. Sequential interactions among episodic and steady alcoholics and their wives. Psychology of Addictive Behaviors. 1997;11:18–25. [Google Scholar]
- Leonard KE, Roberts LJ. Marital aggression, quality, and stability in the first year of marriage: Findings from the Buffalo Newlywed Study. In: Bradbury T, editor. The developmental course of marital dysfunction. Cambridge University; New York: 1998. pp. 44–73. [Google Scholar]
- Leonard KE, Senchak M. Alcohol and premarital aggression among newlywed couples. Journal of Studies on Alcohol. 1993;11:96–108. doi: 10.15288/jsas.1993.s11.96. [DOI] [PubMed] [Google Scholar]
- Locke HJ, Wallace KM. Short marital-adjustment and prediction tests: Their reliability and validity. Marriage & Family Living. 1959;21:251–255. [Google Scholar]
- Lyons-Ruth K, Wolfe R, Lyubchik A, Steingard R. Depressive symptoms in parents of children under age 3: Sociodemographic predictors, current correlates, and associated parenting behaviors. In: Halfon N, McLearn KT, Schuster MA, editors. Child rearing in America: Challenges facing parents with young children. Cambridge University Press; New York: 2002. pp. 217–259. [Google Scholar]
- McLeod JD. Spouse concordance for alcohol dependence and heavy drinking: Evidence from a community sample. Alcoholism, Clinical and Experimental Research. 1993;6:1146–1155. doi: 10.1111/j.1530-0277.1993.tb05220.x. [DOI] [PubMed] [Google Scholar]
- Melby JN, Conger RD, Book R, Rueter M, Lucy L, Repinski D, et al. The Iowa Family Interaction Rating Scales. 5th edition. Institute for Social & Behavioral Research, Iowa State University; Ames: 1998. Unpublished manuscript. [Google Scholar]
- Muthén LK, Muthén BO. Mplus user's guide. Muthén & Muthén; Los Angeles: 1998–2006. [Google Scholar]
- O'Farrell TJ, Birchler GR. Marital relationships of alcoholic, conflicted and nonconflicted couples. Journal of Marital and Family Therapy. 1987;13:259–274. [Google Scholar]
- O'Farrell TJ, Choquette K. Marital violence in the year before and after spouse-involved alcoholism treatment. Family Dynamics of Addiction Quarterly. 1991;1:32–40. [Google Scholar]
- O'Farrell TJ, Murphy CM, Stephan SH, Fals-Stewart W, Murphy M. Partner violence before and after couples based alcoholism treatment for male alcoholic patients. Journal of Consulting and Clinical Psychology. 2004;72:202–217. doi: 10.1037/0022-006X.72.2.202. [DOI] [PubMed] [Google Scholar]
- O'Leary KD, Turkewitz H. Methodological errors in marital and child treatment research. Journal of Consulting and Clinical Psychology. 1978;46:747–758. doi: 10.1037//0022-006x.46.4.747. [DOI] [PubMed] [Google Scholar]
- Radloff LS. The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;1:385–401. [Google Scholar]
- Roberts LJ, Leonard KE. An empirical typology of drinking partnerships and their relationship to marital functioning and drinking consequences. Journal of Marriage and The Family. 1998;60:515–526. [Google Scholar]
- Rosenblum O, Mazet P, Benony H. Mother and infant affective involvement states and maternal depression. Infant Mental Health Journal. 1997;15:350–363. [Google Scholar]
- Sobel ME. Asymptotic confidence intervals for indirect effects in structural equation models. In: Leinhardt S, editor. Sociological methodology. American Sociological Association; Washington, DC: 1982. pp. 290–312. [Google Scholar]
- Stuart GL, Ramsey SE, Moore TM, Kahler CW, Farrell LE, Recupero PR, et al. Reductions in marital violence following treatment for alcohol dependence. Journal of Interpersonal Violence. 2003;18:1113–1131. doi: 10.1177/0886260503255550. [DOI] [PubMed] [Google Scholar]
- Tubman JG. A pilot study of family life among school-age children of problem drinking men: Child, mother and family comparisons. Family Dynamics of Addiction Quarterly. 1991;1:10–20. [Google Scholar]
- Ullman JB. Structural equation modeling. In: Tabachnick BG, Fidell LS, editors. Using multivariate statistics. 4th ed. Allyn & Bacon; Needham Heights, MA: 2001. pp. 653–771. [Google Scholar]
- West MO, Prinz RJ. Parental alcoholism and childhood psychopathology. Psychological Bulletin. 1987;102:204–218. [PubMed] [Google Scholar]
- Zucker RA. Developmental aspects of drinking through the young adult years. In: Blane HT, Chafetz ME, editors. Youth, alcohol, and social policy. Plenum Press; New York: 1979. [Google Scholar]
- Zucker RA, Gomberg ESL. Etiology of alcoholism reconsidered: The case for a biopsychosocial process. American Psychologist. 1986;41:783–793. doi: 10.1037//0003-066x.41.7.783. [DOI] [PubMed] [Google Scholar]
- Zweben A. Problem drinking and marital adjustment. Journal of Studies on Alcohol. 1986;47:167–172. doi: 10.15288/jsa.1986.47.167. [DOI] [PubMed] [Google Scholar]