

Abstract
Anomalous origin of a coronary artery is rare and does not generally lead to myocardial infarction and paroxysmal supraventricular tachycardia (PSVT). We report an uncommon case of anomalous origin of the right coronary artery (RCA) originating from the left sinus of Valsalva with PSVT and myocardial ischemia. A 58-year-old man presented with PSVT. After arrhythmia subsided, electrocardiogram showed ST and T wave abnormalities, and transient cardiac enzymes were found to be elevated. Coronary CT angiography confirmed that there was anomalous origin of the RCA originating from the left sinus of Valsalva and no intracoronary stenotic lesion. He was managed with conservative treatment, having no symptoms on clinical follow-up for 4 years.
Keywords: Coronary vessel anomalies; Tachycardia, paroxysmal; Myocardial ischemia; Multidetector computed tomography
Introduction
Most coronary artery anomalies are incidentally detected during coronary angiography. The prevalence varies between 0.6% and 1.3% in various series.1),2) Anomalous origin of a coronary artery from the opposite sinus of Valsalva represents small fraction of these anomalies.3) Although most instances of anomalous origin of the coronary artery are unlikely to have any clinical sequelae, a few are potentially significant and trigger sudden death and myocardial ischemia4),5) because position or orientation may lead to coronary flow compromise.5) We report an uncommon case of anomalous origin of the right coronary artery (RCA) originating from the left sinus of Valsalva with paroxysmal supraventricular tachycardia (PSVT) and myocardial ischemia.
Case
A 58-year-old man presented with chest pain and palpitation for 2 hours at rest. He had no previous chest pain or palpitation. He had 40-pack-year smoking and daily alcoholic drink. On admission his blood pressure was 130/90 mm Hg, pulse rate 196 beats per minute, respiratory rate 20 per minute and body temperature 36.6℃. The electrocardiogram showed PSVT with pulse rate 190 bpm (Fig. 1A). The patient was treated with adenosine 6 mg twice and his symptoms subsided. Follow-up electrocardiography displayed ST change and T inversion in leads II, III, aVF and V 4-6 (Fig. 1B and C). Blood pressure was 150/100 mm Hg with heart rate of 80 bpm. Cardiac enzyme showed transient increase; creatine kinase-MB 5.8 ng/mL (normal <5 ng/mL), myoglobin 154 ng/mL (normal <110 ng/mL), troponin T 0.3 ng/mL (normal <0.1 ng/mL). He had no other abnormal laboratory findings. Echocardiogram exhibited preserved left ventricle (LV) systolic function and concentric LV hypertrophy. But mild hypokinesia in septum and anterior wall of LV was noted. He was diagnosed with PSVT and temporary acute myocardial injury. After the acute episode terminated, he was treated with aspirin, lipid lowering agent, angiotension II receptor blocker and intravenous heparin. We performed multidetector computed tomography. Coronary CT angiography revealed that the RCA arose from the left sinus of Valsalva with acute angle of the ostium and course between the right ventricular outflow tract and the aorta (Figs. 2 and 3). Other intracoronary atherosclerotic lesion was not observed. The treadmill test was done with good exercise performance and the result showed ST depression in leads III, aVF. 24 hours holter monitoring showed one episode of non-sustained ventricular tachycardia for 0.8 seconds. We continued medical treatment including ATII receptor blocker, bisoprolol and aspirin and recommended life style modification.
Fig. 1.

Variable changes of ECG. A: ECG show paroxysmal supraventricular tachycardia with pulse rate 190. B: ECG show ST elevation in leads V 1-3 and T inversion in leads II, III, aVF and V 4-6. C: electrocardiogram show T wave inversion in leads II, III, aVF and V 3-6. ECG: electrocardiogram.
Fig. 2.

Anomalous orgin of the right coronary artery with CT coronary angiography. A: multiplanar reformatted image from a multi-detector CT coronary angiogram confirms that the right coronary artery was arising from the left sinus Valsalva with acute angle of the ostium (arrow). B: axial reconstruction anomaly coronary artery takes a course between the right ventricular outflow tract and the aorta (arrow) on axial image.
Fig. 3.
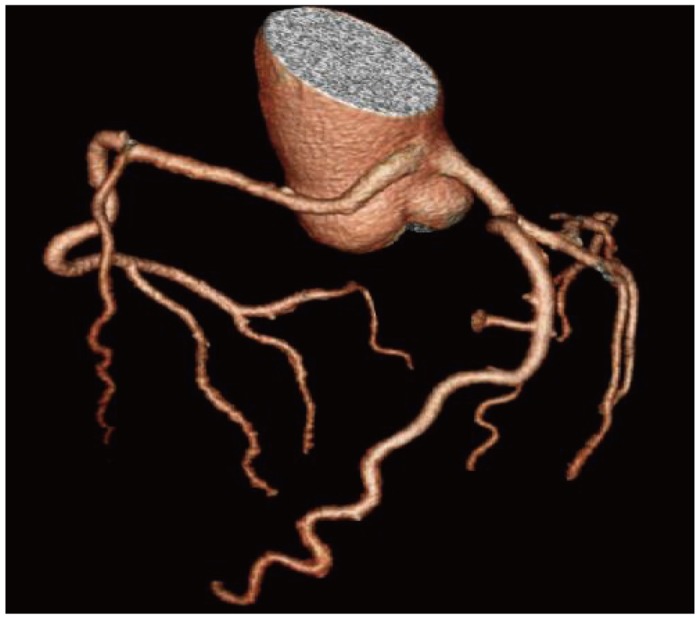
3D volume rendered multi-detector CT image of the coronary arteries show that there is no stenosis of any coronary artery.
Discussion
Coronary artery anomalies, after hypertrophic cardiomyopathy, are the second most common cause of exercise-related sudden cardiac deaths. These anomalies have been associated with myocardial ischemia, arrhythmia and sudden death during exercise.6),7) The prevalence of coronary artery anomalies has been reported between 0.6 to 1.3% in angiographic series and 0.3% in autopsy series.1-4),7) Anomalous origin of the RCA from the left sinus of Valsalva represents a small fraction less than 3% of total coronary anomalies.5) Mechanisms of the restricted coronary blood flow suggest that the acute angle of ostium, slit-like orifice limit the flow of coronary artery.5),8) Also, possible mechanisms are compression of the intramural segment by the aortic valve commissure and compression between the aorta and pulmonary artery.8) In case of interarterial course between aorta and pulmonary artery, luminal compression of the coronary artery is related to the pressure of the aorta because the pressure of the pulmonary artery was much lower than that of the aorta.8) On that account, anomalous coronary artery stemming from opposite sinus of Valsalva can trigger syncope, myocardial ischemia and sudden death in the absence of critically fixed stenosis.5)
The methods for evaluation of anomalous origin of coronary artery include angiography, intravascular ultrasound, transthoracic and transesophageal echocardiogram, coronary CT angiography, and MRI.8) Coronary angiography is limited for evaluation of coronary anomalies since it is sometimes difficult to cannulate the orifice and the complex three dimensional structure of the arteries is displayed in a two dimensional plane.8) Coronary CT angiography is a non-invasive diagnostic modality which provides much higher spatial resolution and three dimensional images.8),9) Understanding ischemic mechanisms in anomalous origin of the RCA is attributed to excellent information about the origin and the course of the anomalous coronary artery from multidetector CT images.10) In the case of our patient, the axial image showed an acute-angled take off of the RCA from the ascending aorta and a small orifice of the RCA which was thought to be one of the mechanisms for the ischemia.
Recent recommendations have favored surgical management of all symptomatic patients.11-13) Nevertheless, there is concern about risk of surgical procedure.12)
We believed that sudden arrhythmias such as PSVT are brought about by hemodynamic changes, widening of aortic root and coronary artery luminal compression between the aorta and the pulmonary artery limiting the coronary artery flow. Our patient performed a treadmill test and the result showed ischemic changes. ST change in EKG and elevated troponin T could be explained as a response to pacing induced stress as well as a response to myocardial ishemia.14) In our patient, myocardial ischemia induced by the coronary anomaly is more likely because of mild hypokinesia of septum and anterior wall of LV, and ischemic change of treadmill test was confirmed. It is a limitation of this case report that the cause of PSVT, whether atrio-ventricular nodal reentry or accessory pathway, was not evaluated by cardiac electrophysiologic study. The electrophysiologic study could help to clarify the relation between coronary anomaly and PSVT.
In our patient, coronary CT angiography showed that the anomalous RCA with inter-arterial pathway and the whole coronary tree was free of any stenotic lesion. We managed him with medications and recommended he avoid intense physical activities. The patient remains clinically well.
Footnotes
The authors have no financial conflicts of interest.
References
- 1.Kimbiris D, Iskandrian AS, Segal BL, Bemis CE. Anomalous aortic origin of coronary arteries. Circulation. 1978;58:606–615. doi: 10.1161/01.cir.58.4.606. [DOI] [PubMed] [Google Scholar]
- 2.Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990;21:28–40. doi: 10.1002/ccd.1810210110. [DOI] [PubMed] [Google Scholar]
- 3.Angelini P, Velasco JA, Flamm S. Coronary anomalies: incidence, pathophysiology, and clinical relevance. Circulation. 2002;105:2449–2454. doi: 10.1161/01.cir.0000016175.49835.57. [DOI] [PubMed] [Google Scholar]
- 4.Kim JS, Lee JM, Yoon HJ, et al. A case of coronary vessel anomaly of the left circumflex artery originating from the right coronary artery with variant angina. Korean Circ J. 2004;34:711–714. [Google Scholar]
- 5.Vincelj J, Todorović N, Marusić P, Puksić S. Anomalous origin of the left coronary artery from the right sinus of Valsalva in a 62-year-old woman with unstable angina pectoris: a case report. Int J Cardiol. 2010;142:e35–e37. doi: 10.1016/j.ijcard.2008.11.182. [DOI] [PubMed] [Google Scholar]
- 6.Basso C, Maron BJ, Corrado D, Thiene G. Clinical profile of congenital coronary artery anomalies with origin from the wrong aortic sinus leading to sudden death in young competitive athletes. J Am Coll Cardiol. 2000;35:1493–1501. doi: 10.1016/s0735-1097(00)00566-0. [DOI] [PubMed] [Google Scholar]
- 7.Dogan SM, Gursurer M, Aydin M, Gocer H, Cabuk M, Dursun A. Myocardial ischemia caused by a coronary anomaly left anterior descending coronary artery arising from right sinus of Valsalva. Int J Cardiol. 2006;112:e57–e59. doi: 10.1016/j.ijcard.2006.03.063. [DOI] [PubMed] [Google Scholar]
- 8.Lee BY. Anomalous right coronary artery from the left coronary sinus with an interarterial course: is it really dangerous? Korean Circ J. 2009;39:175–179. doi: 10.4070/kcj.2009.39.5.175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Park CS, Kim W, Hong SB, Hwang SH, Kim W, An BH. Anomalous origin of the right coronary artery from the main pulmonary artery presenting as angina pectoris in an adult. Korean Circ J. 2008;38:627–629. [Google Scholar]
- 10.Tariq R, Kureshi SB, Siddiqui UT, Ahmed R. Congenital anomalies of coronary arteries: diagnosis with 64 slice multidetector CT. Eur J Radiol. 2012;81:1790–1797. doi: 10.1016/j.ejrad.2011.05.034. [DOI] [PubMed] [Google Scholar]
- 11.Earls JP. Coronary artery anomalies. Tech Vasc Interv Radiol. 2006;9:210–217. doi: 10.1053/j.tvir.2007.03.007. [DOI] [PubMed] [Google Scholar]
- 12.Mirchandani S, Phoon CK. Management of anomalous coronary arteries from the contralateral sinus. Int J Cardiol. 2005;102:383–389. doi: 10.1016/j.ijcard.2004.10.010. [DOI] [PubMed] [Google Scholar]
- 13.Reul RM, Cooley DA, Hallman GL, Reul GJ. Surgical treatment of coronary artery anomalies: report of a 37 1/2-year experience at the Texas Heart Institute. Tex Heart Inst J. 2002;29:299–307. [PMC free article] [PubMed] [Google Scholar]
- 14.Turer AT, Addo TA, Martin JL, et al. Myocardial ischemia induced by rapid atrial pacing causes troponin T release detectable by a highly sensitive assay: insights from a coronary sinus sampling study. J Am Coll Cardiol. 2011;57:2398–2405. doi: 10.1016/j.jacc.2010.11.066. [DOI] [PMC free article] [PubMed] [Google Scholar]