

Abstract
Background
Strongyloidiasis is commonly a clinically unapparent, chronic infection, but immuno suppressed subjects can develop fatal disease. We carried out a review of literature on hyperinfection syndrome (HS) and disseminated strongyloidiasis (DS), in order to describe the most challenging aspects of severe strongyloidiasis.
Methods
We conducted a structured search using PubMed to collect case reports and short case series on HS/DS published from 1991 to 2011. We restricted search to papers in English, Spanish, Italian and French. Case reports were classified as HS/DS according to given definitions.
Results
Records screened were 821, and 311 were excluded through titles and abstract evaluation. Of 510 full-text articles assessed for eligibility, 213 were included in qualitative analysis. As some of them were short case series, eventually the number of cases analyzed was 244.
Steroids represented the main trigger predisposing to HS and DS (67% cases): they were mostly administered to treat underlying conditions (e.g. lymphomas, rheumatic diseases). However, sometimes steroids were empirically prescribed to treat signs and symptoms caused by unsuspected/unrecognized strongyloidiasis. Diagnosis was obtained by microscopy examination in 100% cases, while serology was done in a few cases (6.5%). Only in 3/29 cases of solid organ/bone marrow transplantation there is mention of pre-transplant serological screening. Therapeutic regimens were different in terms of drugs selection and combination, administration route and duration. Similar fatality rate was observed between patients with DS (68.5%) and HS (60%).
Conclusions
Proper screening (which must include serology) is mandatory in high - risk patients, for instance candidates to immunosuppressive medications, currently or previously living in endemic countries. In some cases, presumptive treatment might be justified. Ivermectin is the gold standard for treatment, although the optimal dosage is not clearly defined in case of HS/DS.
Keywords: Strongyloidiasis, Strongyloides, Hyperinfection, Disseminated strongyloidiasis, Review
Background
Strongyloidiasis is a neglected condition caused by Strongyloides stercoralis, a soil – transmitted helminth mainly diffused in tropical and subtropical regions, but also present in small areas of low endemicity in temperate climates [1]. Most infected individuals are asymptomatic or may present intermittent symptoms, mostly affecting intestine (from mild abdominal pain, intermittent or persistent diarrhea to more severe conditions that can mimic inflammatory bowel disease), lungs (cough, wheezing and asthma, chronic bronchitis) and skin (pruritus, rash). Systemic symptoms such as weight loss and cachexia may also occur [2]. Immune suppressed subjects tend to develop hyperinfection syndrome (HS) and disseminated strongyloidiasis (DS), that are potentially fatal [3]. Therefore, it is mandatory to diagnose and treat the chronic infection, in order to prevent the life-threatening form. Unfortunately, the index of suspicion of health care providers seems to be low, especially in non-endemic countries [4]. Moreover, there are still gaps in knowledge regarding many aspects of the infection, such as diagnosis and treatment response [2].
Our aim was to systematically review case reports of severe strongyloidiasis, in order to outline the main features of hyperinfection and disseminated strongyloidiasis and the difficulties in their management.
Methods
We carried out a systematic review of case reports/short case series published in PubMed from January 1991 to April 2011. We considered papers available in the following languages: English, Spanish, Italian, French.
The electronic search strategy was as follows: disease (strongyl*, anguillulose) AND severity of cases (disseminat*, hyperinfect*, severe, death, fatal, mortality) OR disease (strongyl*, anguillulose) AND associated conditions (tumor*, cancer, haematolog*, lymphom*, leukem*, leukaem*, neoplas*, malignan*, HTLV*, HIV, AIDS, hypogammaglobulinemia, rheumat*, “biological agents”, diabet*, transplant*, COPD, steroid*, glucocorticoid*, Immunosuppression [MeSH], Immunocompromised Host [MeSH]) and limiting the search to humans. Search was done on March 20th 2011.
Definitions used for case - inclusion [5]: - Dissemination: larvae found in any organ, other than the respiratory and the gastrointestinal tracts. Hyperinfection: infection confined to lungs and gastrointestinal tract, but signs/symptoms of severe diseases in relation to elevated number of larvae; in particular, necessity of intensive care, presence of sepsis/meningitis by enteric bacteria, death (without any other clear underlying cause).
Results
Data synthesis
Our search strategy permitted to identify 821 papers, of which 311 were excluded by title and abstract evaluation. Full-text papers were then assessed for eligibility according to the criteria outlined above. Among the 213 papers included, some were small case series, eventually the number of cases analyzed was 244 (Figure 1).
Figure 1.

PRISMA flow chart: data collection and selection of studies.
Countries
Reports from highly endemic countries were 65/244 (27%), with India ( [6-23]), Argentina ( [24-28]), Brazil ( [29-39]) and Peru ( [40-42]) accounting for more than two thirds. Only four cases were reported from the whole of Africa [43-46], three of which in South Africa, a state where adequate diagnostic facilities are available. We collected 83/244 (34%) reports from North America (USA [47-109] and Canada [110-116]), 58/244 (24%) from Europe (Belgium [40,117], France [118-129], Germany [130,131], Greece [132-134], Italy [135-141], the Netherlands [142-145], Spain [146-155], Switzerland [156], UK [157-164]) and five (2%) from Oceania (Australia [165-168] and New Zealand [169]). In these areas of low/no endemicity, half of the patients were immigrants (70/146, 48%), while a few subjects were veterans (5/146, 3%) who presumably acquired the infection during military service in an endemic country. Other areas of low endemicity where cases have been reported are in Eastern Asia (21 cases, mostly from Japan ( [170-177]) and Taiwan ( [178-182])), the Arabian peninsula (nine cases, mostly from Kuwait ( [183,184]) and Qatar ( [185,186])) and Israel ( [187,188]) (three cases). Countries such as Iran ( [189]), Turkey ( [190]) and Venezuela ( [191]) that might be presumed at medium to high prevalence, account for only one case each.
Triggers for development of HS/DS
According to the case definitions, 171 cases were classified as hyper infection and 73 cases as dissemination.
A high percentage of patients (67%: 164/244) were under corticosteroids: most of them presented clinical conditions causing immune suppression per-se or due to other related therapies (for instance leukemia, rheumatic conditions, transplant), as it is shown in Table 1. On the other hand, a few patients were taking steroids for eosinophilia and/or a specific symptoms caused by S. stercoralis itself (data reported in Table 1 too). A patient even underwent bone marrow transplant because of an unexplained eosinophilia misdiagnosed as “idiopathic hypereosinophilic syndrome” [81]; after receiving steroids and immunosuppressive therapy he developed HS (but only limited autopsy was performed, so we cannot rule out DS) and died.
Table 1.
Patients under steroid treatment: reasons for prescription
| Condition | N (%) | References |
|---|---|---|
| COPD/asthma/lung fibrosis |
30 (18.3) |
[48,49,52,57-59,68,99,101,118,121,123,128,137,146,153,180-183,185,187,188,192-196] |
| Leukemia/lymphoma |
13 (7.9) |
[9,17,23,25,37,47,56,98,111,126,162,186] |
| SLE |
9 (5.5) |
[41,64,66,86,151,176,197,198] |
| Rheumatoid arthtritis |
4 (2.4) |
[83,103,199,200] |
| IBD |
6 (3.6) |
[59,147,148,164,177,201] |
| Sarcoidosis |
2 (1.2) |
[65,132] |
| Cancer |
8 (4.8) |
[30,54,93,97,112,160,169,202] |
| Organ/bone marrow transplant |
25 (15.2) |
[21,25,29,31,39,48,51,54,60,70,71,74,76,81,87,88,90,92,94,142,145,150,184] |
| Glomerulonephritis/CRI |
6 (3.6) |
[16,18,20,129,130,154] |
| “Idiopatic” eosinophilia |
3 (1.8) |
[7] |
| Multiple myeloma/myelodisplasia |
6 (3.6) |
[72,185,203-206] |
| Aspecific symptoms |
2 (1.2) |
[85,166] |
| Other clinical conditions |
46 (28) |
[17,22,34,36,54,59,66,84,89,100,102,110,113,124,125,127,133-135,140,155,159,171-174,207-213] |
| HIV-related opportunistic infections/IRIS | 4 (2.4) | [24,26,36,105] |
Transplant is surely an event that poses the Strongyloides - infected patient at high risk of developing HS/DS. We collected 28/244 (11.5%) cases of HS/DS in transplant patients, of whom 19 (68%) died. A couple of patients who developed hyper infection also had co infection with CMV [21,107]. All the surviving patients received ivermectin, either as single treatment (1 patient) or in combination with albendazole (7) or thiabendazole (1) [29,54,60,71,90,92,94,142,145,150].
HTLV-1 infection is a well known risk factor (sometimes in association with related haematological malignancies), of which we found 24/244 (10%) reports ([214,158,120,159,53,54,143,122,12,111,32,216,77,126,163,114,80,35,164,175,155,116]). Ten of the 24 patients (42%) died. One patient had HTLV-1-HIV co infection [122]; he developed an E. coli meningitis but successfully responded to ivermectin, two doses given some days (not specified how many) apart.
We found 38/244 (15%) reports on HIV-positive patients, 26 (68%) of whom died (Figure 2). Seven HIV patients were also receiving steroids for suspected Pneumocystis jiroveci pneumonia [24,26], immune reconstitution inflammatory syndrome [105], misdiagnosis of asthma [58], Wegener granulomatosis [36], toxoplasmosis encephalitis [36], cerebral TB with vasculitis [124]; six of them died.
Figure 2.
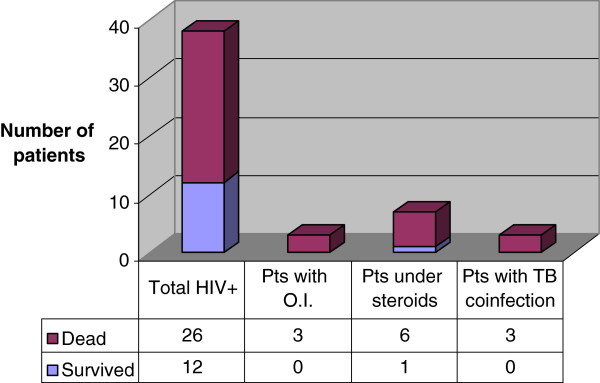
Deaths in the HIV patients subgroup.
A few reports/case series describe severe strongyloidiasis in patients with alcoholism [178,217] and malnutrition [27,171]. An apparently immunocompetent patient developed hyper infection and died two days after having started therapy with thiabendazole [149]. Unfortunately autopsy was denied.
Diagnosis
Eosinophilia was present in 55/244 cases (22.5%) overall, and only in 12/73 cases (16.4%) of dissemination. In all cases S. stercoralis was found at microscopy examination of biological samples. Serology was performed only in 16/244 patients (6.5%) (Table 2). In a couple of organ transplant recipients, an ELISA test was negative pre-transplant, but resulted positive in the deceased donors (test performed retrospectively) [60,145]. In other two cases serology (ELISA) was negative: a HIV-infected person, who had larvae in stool and sputum [165] and a patient with dermatomyositis, under chronic treatment with prednisone and methotrexate, who died from disseminated strongyloidiasis (larvae found at autopsy in skin, lungs, small and large bowel, gall bladder, vessels of meninges and cervical spinal cord) [100].
Table 2.
Patients tested with serology: chronic conditions and corticosteroids therapy
| Year | Chronic condition | Corticosteroids | Serology | Ref. |
|---|---|---|---|---|
| 1991 |
polychondritis |
Yes |
positive |
[89] |
| 1994 |
COPD |
Yes |
positive |
[57] |
| 1996 |
HIV |
No |
negative |
[165] |
| 2001 |
none |
Yes |
positive |
[166] |
| 2004 |
bronchogenic carcinoma |
Yes |
positive |
[160] |
| 2004 |
none |
Yes |
positive |
[183] |
| 2005 |
multiple myeloma |
Yes |
positive |
[72] |
| 2005 |
multiple myeloma |
Yes |
positive |
[204] |
| 2005 |
nephrotic syndrome |
No |
positive |
[204] |
| 2007 |
nephrotic syndrome |
Yes |
positive |
[139] |
| 2008 |
none |
Yes |
positive |
[144] |
| 2008 |
asthma |
Yes |
positive |
[101] |
| 2009 |
heart transplant |
Yes |
negative |
[145] |
| 2009 |
lung transplant |
Yes |
positive |
[92] |
| 2010 |
dermatomyositis |
Yes |
negative |
[100] |
| 2011 | renal transplant | Yes | negative | [60] |
Diagnosis was obtained post mortem in 29 cases (12%).
Therapy
Therapies given were very different in relation to the drugs used and the length of treatment.
In Table 3 we summarize the drugs used. In the “other drugs” group we found mebendazole [9,17,44,48,131,137,181,218], cambendazole [35,36], levamisole [43,199], pyrantel pamoate [75,108], diethylcarbamazine [14].
Table 3.
Treatments
| Drug | Albendazole | Ivermectin | Thiabendazole | Other drugs |
|---|---|---|---|---|
|
Used as single treatment |
34 |
38 |
55 |
6 |
|
Deaths among patients treated with single drug |
25/34 (73%) |
18/38 (47%) |
28/55 (51%) |
5/6 (83%) |
| Total of patients treated (including combination therapy) | 48 | 79 | 60 | 14 |
Albendazole was used as a single drug even in recent case reports; since 2008 we found patients treated with albendazole only in reports from Pakistan [203], Romania [217], Taiwan [182], Israel [187], Kuwait [184], Argentina [25], Malaysia [207], Greece [133], Thailand [208].
In most cases the administration route was oral, but due to severe clinical conditions of patients, administration via nasogastric tube, subcutaneous injection (veterinary formulation) and retention enema were used, too.
A patient who developed disseminated strongyloidiasis after an empiric steroid treatment for pruritic rash was treated with albendazole [166]. Only one dose could be given, as the patient died. After his death, a review of his clinical records showed that he had been previously diagnosed with strongyloidiasis and treated with a 3-day course of albendazole; although serology persisted positive and eosinophilia was still present 6 and 12 months after treatment, the patient did not receive any further therapy. Another patient who died from Strongyloides hyper infection had never been treated previously, despite a positive serology [101].
Outcome
The recorded deaths were 153/244 (62.7%). A similar fatality rate was observed in patients with dissemination (50/73 = 68.5%) and with hyperinfection (102/171 = 60%).
All 42 of 244 patients who did not receive any therapy died. Excluding patients treated with combination therapy, we observe that 25/34 (73%) patients treated with albendazole died, while deaths among patients treated with ivermectin and thiabendazole were 18/38 (47%) and 28/55 (51%), respectively.
Discussion
Considering that a considerable number of case reports are described in non endemic countries, we assume that fatal cases must be quite frequent in endemic countries, although they are not frequently published in the literature.
The main risk factors identified in this review have been reported previously, in particular steroids are frequently the trigger for developing severe strongyloidiasis. Unfortunately it was not possible to extract from the case reports the cumulative dosage and the duration of the corticosteroids treatment. Although the association with steroids should be well known, there are still papers reporting cases of patients under steroids who had not been previously screened for strongyloidiasis. Moreover, we found papers reporting severe strongyloidiasis in patients who were previously diagnosed with the infection but had not received a proper treatment. Once more, the lack of familiarity with strongyloidiasis by health care providers is the weak link in the chain; this is also highlighted by the fact that in 12% of cases the diagnosis was made post mortem. Eosinophil count is often normal in severe strongyloidiasis, hence this test has a limited excluding power.
Serology was not frequently performed. In fact, in case of hyperinfection and dissemination the diagnosis is easily made by direct examination of the biological samples. Serology would be most useful in chronic infections, before hyperinfection and/or dissemination occur, while in patients who are already immune suppressed its sensitivity is probably lower.
Limits in our results are due to incomplete information in the case descriptions. Moreover, cases in which autopsy was not performed sometimes couldn’t allow a proper classification. Actually, in the 65 cases we classified as hyper infections, autopsy was not done, hence it is not possible to rule out dissemination. Moreover, we found the same fatality rate for patients with hyper infection and with dissemination, but a misclassification might have played a role. In fact, we think that from a clinical, practical point of view the distinction between hyper infection and dissemination is not essential, because they’re both severe conditions requiring immediate assessment and care.
In general, the best drug to treat strongyloidiasis is ivermectin which is effective and well tolerated. There are still some concerns about the treatment schedule of the chronic infection, and this is even more debated in case of hyper infection/dissemination. In fact there are no specific guidelines and the case reports we collected outline a Babylon of different therapeutic schemes. Subcutaneous ivermectin (veterinary formulation) has been used on an empiric basis, when intestinal absorption is decreased or the patient cannot swallow tablets. On the other hand, albendazole is still used even as a single drug, although it has been proved to be poorly effective. In some cases, this might be due to the scarce availability of ivermectin in many countries.
Conclusions
The first step to be done to guarantee an adequate management of infected patients is to avoid a delayed diagnosis. Unfortunately, lack of familiarity with strongyloidiasis by health care providers still seems to be the main cause of delay. A better diffusion of the available information is badly needed, and collaboration among different specialists (oncologists, rheumatologists…) is desirable in order to provide common and adequate protocols for screening and treatment of at – risk patients.
It is mandatory to treat patients in the chronic phase, before HS/DS develop. Patients with possible, previous exposure to the parasite should be screened with serology before corticosteroid treatment, chemotherapy or transplant. Considering the high tolerability of ivermectin, it would be probably worth treating high – risk patients irrespective of the result of the screening test, in order to avoid the potential consequences of a possible false negative result.
Ivermectin is currently the gold standard for treatment of strongyloidiasis, so it is simply no more ethical to use any other drug. Moreover, ivermectin is in the WHO model lists of essential medicines [219], so it should be registered and made available everywhere, particularly in endemic countries.
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
DB searched PubMed, analyzed the data and wrote the manuscript. ARM analyzed the data and critically reviewed the manuscript. AA created the search strategy and analyzed the data. JM, FG and JVDE gave intellectual content and critically reviewed the manuscript. ZB conceptualized the review and critically reviewed the manuscript. All authors read and approved the final manuscript.
Authors’ information
Cohemi project study group: Maurizio Bonati, Francesca Severino, Valeria Confalonieri, Chiara Pandolfini, Zeno Bisoffi, Dora Buonfrate, Andrea Angheben, Marco Albonico, Alessandro Bartoloni, Marianne Strohmeyer, Lorenzo Zammarchi, Jose Muñoz, Robert Pool, Ana Requena-Mendez, Maria Roura, Anita Hardon, Christopher Pell, Peter Chiodini, Juan Moreira, Roberto Sempértegui, Mariella Anselmi, Eduardo Gotuzzo, Maria Alejandra Mena, Hector H. Garcia, Javier Bustos, Saul Santiva, Faustino Torrico,Daniel Lozano, Guido Chumiray Rojas, Teresa Hinojosa Cabrera, Javier Ochoa Morón, Ignacio Abapori Cuellar, Jaime Amorós Suarez, Gianni Tognoni, Alessandra Nicoletti, Elisa Bruno
Pre-publication history
The pre-publication history for this paper can be accessed here:
Contributor Information
Dora Buonfrate, Email: dora.buonfrate@sacrocuore.it.
Ana Requena-Mendez, Email: ana.requena@cresib.cat.
Andrea Angheben, Email: andrea.angheben@sacrocuore.it.
Jose Muñoz, Email: jmunoz@clinic.ub.es.
Federico Gobbi, Email: federico.gobbi@sacrocuore.it.
Jef Van Den Ende, Email: jvdende@itg.be.
Zeno Bisoffi, Email: zeno.bisoffi@sacrocuore.it.
Acknowledgements
This work has been supported by the EC within the 7th Framework Program under grant agreement FP7-GA-261495.
References
- WHO. Strongyloidiasis. http://www.who.int/neglected_diseases/diseases/strongyloidiasis/en/
- Olsen A, Van Lieshout L, Marti H, Polderman T, Polman K, Steinmann P, Stothard R, Thybo S, Verweij JJ, Magnussen P. Strongyloidiasis–the most neglected of the neglected tropical diseases? Trans R Soc Trop Med Hyg. 2009;103(10):967–972. doi: 10.1016/j.trstmh.2009.02.013. [DOI] [PubMed] [Google Scholar]
- Marcos LA, Terashima A, Canales M, Gotuzzo E. Update on Strongyloidiasis in the immunocompromised host. Curr Infect Dis Rep. 2011;13:35–46. doi: 10.1007/s11908-010-0150-z. [DOI] [PubMed] [Google Scholar]
- Boulware DR, Stauffer WM, Hendel-Paterson BR, Rocha JL, Seet RC, Summer AP, Nield LS, Supparatpinyo K, Chaiwarith R, Walker PF. Maltreatment of Strongyloides infection: case series and worldwide physicians-in-training survey. Am J Med. 2007;120(6):545. doi: 10.1016/j.amjmed.2006.05.072. e541-548. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keiser PB, Nutman TB. Strongyloides stercoralis in the immunocompromised population. Clin Microbiol Rev. 2004;17(1):208–217. doi: 10.1128/CMR.17.1.208-217.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Agrawal V, Agarwal T, Ghoshal UC. Intestinal strongyloidiasis: a diagnosis frequently missed in the tropics. Trans R Soc Trop Med Hyg. 2009;103(3):242–246. doi: 10.1016/j.trstmh.2008.08.009. [DOI] [PubMed] [Google Scholar]
- Ghosh K. Strongyloides stercoralis septicaemia following steroid therapy for eosinophilia: report of three cases. T Roy Soc Trop Med H. 2007;101(11):1163–1165. doi: 10.1016/j.trstmh.2007.05.021. [DOI] [PubMed] [Google Scholar]
- Das P, Raghu P, Amit Kumar D, Garg P. Strongyloides hyperinfection in rheumatoid arthritis. Int J Surg Pathol. 2007;15(4):391–392. doi: 10.1177/1066896907302241. [DOI] [PubMed] [Google Scholar]
- Ghoshal UC, Saha J, Ghoshal U, Ray BK, Santra A, Naik S, Mazumder DN. Pigmented nails and Strongyloides stercoralis infestation causing clinical worsening in a patient treated for immunoproliferative small intestinal disease: two unusual observations. J Diarrhoeal Dis Res. 1999;17(1):43–45. [PubMed] [Google Scholar]
- Ghoshal UC, Ghoshal U, Jain M, Kumar A, Aggarwal R, Misra A, Ayyagari A, Naik SR. Strongyloides stercoralis infestation associated with septicemia due to intestinal transmural migration of bacteria. J Gastroenterol Hepatol. 2002;17(12):1331–1333. doi: 10.1046/j.1440-1746.2002.02750.x. [DOI] [PubMed] [Google Scholar]
- Ghoshal UC, Alexender G, Ghoshal U, Tripathi S, Krishnani N. Strongyloides stercoralis infestation in a patient with severe ulcerative colitis. Indian J Med Sci. 2006;60(3):106–110. doi: 10.4103/0019-5359.22761. [DOI] [PubMed] [Google Scholar]
- Jeyamani R, Joseph AJ, Chacko A. Severe and treatment resistant strongyloidiasis–indicator of HTLV-I infection. Trop Gastroenterol. 2007;28(4):176–177. [PubMed] [Google Scholar]
- Murali A, Rajendiran G, Ranganathan K, Shanthakumari S. Disseminated infection with Strongyloides stercoralis in a diabetic patient. Indian J Med Microbiol. 2010;28(4):407–408. doi: 10.4103/0255-0857.71854. [DOI] [PubMed] [Google Scholar]
- Patil PL, Salkar HR, Ghodeswar SS, Gawande JP. Parasites (filaria & strongyloides) in malignant pleural effusion. Indian J Med Sci. 2005;59(10):455–456. doi: 10.4103/0019-5359.17053. [DOI] [PubMed] [Google Scholar]
- Premanand R, Prasad GV, Mohan A, Gururajkumar A, Reddy MK. Eosinophilic pleural effusion and presence of filariform larva of Strongyloides stercoralis in a patient with metastatic squamous cell carcinoma deposits in the pleura. Indian J Chest Dis Allied Sci. 2003;45(2):121–124. [PubMed] [Google Scholar]
- Rajapurkar M, Hegde U, Rokhade M, Gang S, Gohel K. Respiratory hyperinfection with Strongyloides stercoralis in a patient with renal failure. Nat Clin Pract Nephrol. 2007;3(10):573–577. doi: 10.1038/ncpneph0598. [DOI] [PubMed] [Google Scholar]
- Reddy IS, Swarnalata G. Fatal disseminated strongyloidiasis in patients on immunosuppressive therapy: report of two cases. Indian J Dermatol Venereol Leprol. 2005;71(1):38–40. doi: 10.4103/0378-6323.13785. [DOI] [PubMed] [Google Scholar]
- Sathe PA, Madiwale CV. Strongyloidiasis hyperinfection in a patient with membranoproliferative glomerulonephritis. J Postgrad Med. 2006;52(3):221–222. [PubMed] [Google Scholar]
- Satyanarayana S, Nema S, Kalghatgi AT, Mehta SR, Rai R, Duggal R, Bhardwaj JR. Disseminated Strongyloides stercoralis in AIDS: a report from India. Indian J Pathol Microbiol. 2005;48(4):472–474. [PubMed] [Google Scholar]
- Sekhar U, Madan M, Ranjitham M, Abraham G, Eapen G. Strongyloides hyperinfection syndrome–an unappreciated opportunistic infection. J Assoc Physicians India. 2000;48(10):1017–1019. [PubMed] [Google Scholar]
- Soman R, Vaideeswar P, Shah H, Almeida AF. A 34-year-old renal transplant recipient with high-grade fever and progressive shortness of breath. J Postgrad Med. 2002;48(3):191–196. [PubMed] [Google Scholar]
- Sreenivas DV, Kumar A, Kumar YR, Bharavi C, Sundaram C, Gayathri K. Intestinal strongyloidiasis–a rare opportunistic infection. Indian J Gastroenterol: J Indian Soc Gastroenterol. 1997;16(3):105–106. [PubMed] [Google Scholar]
- Vigg A, Mantri S, Reddy VA, Biyani V. Acute respiratory distress syndrome due to Strongyloides stercoralis in non-Hodgkin’s lymphoma. Indian J Chest Dis Allied Sci. 2006;48(1):67–69. [PubMed] [Google Scholar]
- Bava AJ, Troncoso AR. Strongyloides stercoralis hyperinfection in a patient with AIDS. J Int Assoc Physicians AIDS Care (Chic) 2009;8(4):235–238. doi: 10.1177/1545109709336882. [DOI] [PubMed] [Google Scholar]
- Galimberti R, Ponton A, Zaputovich FA, Velasquez L, Galimberti G, Torre A, Kowalczuk A. Disseminated strongyloidiasis in immunocompromised patients–report of three cases. Int J Dermatol. 2009;48(9):975–978. doi: 10.1111/j.1365-4632.2009.04082.x. [DOI] [PubMed] [Google Scholar]
- Rivero FD, Kremer LE, Allende L, Casero RD. [Strongyloides stercoralis and HIV: a case report of an indigenous disseminated infection from non-endemic area] Rev Argent Microbiol. 2006;38(3):137–139. [PubMed] [Google Scholar]
- Taranto NJ. [Strongyloides stercoralis. Report of a case and review of the literature] Acta Gastroenterol Latinoam. 1995;25(2):113–120. [PubMed] [Google Scholar]
- Trione N, Corti M, Castello T, Abuin JC, Bellegarde E. [Disseminated infection due to strongyloides stercoralis in AIDS patients. A report of 2 cases] Acta Gastroenterol Latinoam. 2001;31(5):399–402. [PubMed] [Google Scholar]
- Dulley FL, Costa S, Cosentino R, Gamba C, Saboya R. Strongyloides stercoralis hyperinfection after allogeneic stem cell transplantation. Bone Marrow Transplant. 2009;43(9):741–742. doi: 10.1038/bmt.2008.383. [DOI] [PubMed] [Google Scholar]
- Salluh JI, Feres GA, Velasco E, Holanda GS, Toscano L, Soares M. Successful use of parenteral ivermectin in an immunosuppressed patient with disseminated strongyloidiasis and septic shock. Intensive Care Med. 2005;31(9):1292. doi: 10.1007/s00134-005-2725-y. [DOI] [PubMed] [Google Scholar]
- German JC, Flores JH, Chiesura G, Ruiz EM, Flores SS, Laudanna AA. [Fatal strongyloidiasis in an immunodepressed patient following renal transplantation] Revista do Hospital das Clinicas. 1992;47(1):31–33. [PubMed] [Google Scholar]
- Lambertucci JR, Leao FC, Barbosa AJ. Gastric strongyloidiasis and infection by the human T cell lymphotropic virus type 1 (HTLV-1) Rev Soc Bras Med Trop. 2003;36(4):541–542. doi: 10.1590/S0037-86822003000400021. [DOI] [PubMed] [Google Scholar]
- Lambertucci JR, Westin MR, Barbosa AJ. Severe gastrointestinal strongyloidiasis. Rev Soc Bras Med Trop. 2005;38(4):365–366. doi: 10.1590/S0037-86822005000400023. [DOI] [PubMed] [Google Scholar]
- Rodrigues MA, Froes RC, Anefalos A, Kobayasi S. Invasive enteritis by Strongyloides stercoralis presenting as acute abdominal distress under corticosteroid therapy. Revista do Hospital das Clinicas. 2001;56(4):103–106. doi: 10.1590/S0041-87812001000400002. [DOI] [PubMed] [Google Scholar]
- Porto MA, Alcantara LM, Leal M, Castro N, Carvalho EM. Atypical clinical presentation of strongyloidiasis in a patient co-infected with human T cell lymphotrophic virus type I. Am J Trop Med H. 2005;72(2):124–125. [PubMed] [Google Scholar]
- Siciliano RF, Mascheretti M, Ho YL, Gryschek RC. Severe strongyloidiasis in AIDS: is steroid therapy guilty again? J Acquir Immune Defic Syndr. 2008;49(3):333–334. doi: 10.1097/QAI.0b013e31817bedde. [DOI] [PubMed] [Google Scholar]
- Tabacof J, Feher O, Katz A, Simon SD, Gansl RC. Strongyloides hyperinfection in two patients with lymphoma, purulent meningitis, and sepsis. Cancer. 1991;68(8):1821–1823. doi: 10.1002/1097-0142(19911015)68:8<1821::AID-CNCR2820680829>3.0.CO;2-J. [DOI] [PubMed] [Google Scholar]
- Takayanagui OM, Lofrano MM, Araugo MB, Chimelli L. Detection of Strongyloides stercoralis in the cerebrospinal fluid of a patient with acquired immunodeficiency syndrome. Neurology. 1995;45(1):193–194. doi: 10.1212/WNL.45.1.193. [DOI] [PubMed] [Google Scholar]
- Vilela EG, Clemente WT, Mira RR, Torres HO, Veloso LF, Fonseca LP, De Carvalho EFLR, Franca MC, Lima AS. Strongyloides stercoralis hyperinfection syndrome after liver transplantation: case report and literature review. Transplant Inf Dis: J Transplant Soc. 2009;11(2):132–136. doi: 10.1111/j.1399-3062.2008.00350.x. [DOI] [PubMed] [Google Scholar]
- De Goede E, Martens M, Van Rooy S, VanMoerkerke I. A case of systemic strongyloidiasis in an ex-coal miner with idiopathic colitis. European J Gastroenterol Hepatol. 1995;7(8):807–809. [PubMed] [Google Scholar]
- Mora CS, Segami MI, Hidalgo JA. Strongyloides stercoralis hyperinfection in systemic lupus erythematosus and the antiphospholipid syndrome. Semin Arthritis Rheu. 2006;36(3):135–143. doi: 10.1016/j.semarthrit.2006.06.001. [DOI] [PubMed] [Google Scholar]
- Zavala J, Sanchez L, Carillo L, Cueva A, Balbin G, Quispe V. [Atypical presentations of strongyloidiasis: a report of 8 cases] Rev Gastroenterol Peru. 1994;14(1):15–21. [PubMed] [Google Scholar]
- Adetiloye VA. A case of fatal gastrointestinal strongyloidiasis in an otherwise healthy Nigerian, masquerading as gastric outlet obstruction. Trop Geogr Med. 1992;44(1–2):60–62. [PubMed] [Google Scholar]
- Coovadia YM, Rajput MC, Bhana RH. Disseminated strongyloidiasis in a diabetic patient. Trop Geogr Med. 1993;45(4):179–180. [PubMed] [Google Scholar]
- Daubenton JD, Buys HA, Hartley PS. Disseminated strongyloidiasis in a child with lymphoblastic lymphoma. J Pediatr Hematol Oncol: Am Soc Pediatr Hematol Oncol. 1998;20(3):260–263. doi: 10.1097/00043426-199805000-00014. [DOI] [PubMed] [Google Scholar]
- Haddow LJ, Mahlakwane MS, Ramdial PK, Moosa MY. Histopathology of Strongyloides stercoralis hyperinfection during immune reconstitution in an HIV-infected patient. AIDS. 2009;23(12):1609–1611. doi: 10.1097/QAD.0b013e32832c41f4. [DOI] [PubMed] [Google Scholar]
- Jamil SA, Hilton E. The Strongyloides hyperinfection syndrome. New York State J. 1992;92(2):67–68. [PubMed] [Google Scholar]
- Purvis RS, Beightler EL, Diven DG, Sanchez RL, Tyring SK. Strongyloides hyperinfection presenting with petechiae and purpura. Nt J Dermatol. 1992;31(3):169–171. doi: 10.1111/j.1365-4362.1992.tb03925.x. [DOI] [PubMed] [Google Scholar]
- Boken DJ, Leoni PA, Preheim LC. Treatment of Strongyloides stercoralis hyperinfection syndrome with thiabendazole administered per rectum. Clin Infect Dis: Infect Dis Soc Am. 1993;16(1):123–126. doi: 10.1093/clinids/16.1.123. [DOI] [PubMed] [Google Scholar]
- Celedon JC, Mathur-Wagh U, Fox J, Garcia R, Wiest PM. Systemic strongyloidiasis in patients infected with the human immunodeficiency virus. A report of 3 cases and review of the literature. Medicine. 1994;73(5):256–263. doi: 10.1097/00005792-199409000-00004. [DOI] [PubMed] [Google Scholar]
- El Masry HZ, O’Donnell J. Fatal stongyloides hyperinfection in heart transplantation. J Heart Lung Transpl: Int Soc Heart Transpl. 2005;24(11):1980–1983. doi: 10.1016/j.healun.2005.04.005. [DOI] [PubMed] [Google Scholar]
- Foreman EB, Abraham PJ, Garland JL. Not your typical strongyloides infection: a literature review and case study. South Med J. 2006;99(8):847–852. doi: 10.1097/01.smj.0000203813.70054.3c. [DOI] [PubMed] [Google Scholar]
- Friedenberg F, Wongpraparut N, Fischer RA, Gubernick J, Zaeri N, Eiger G, Ozden Z. Duodenal obstruction caused by Strongyloides stercoralis enteritis in an HTLV-1-infected host. Digest Dis Sci. 1999;44(6):1184–1188. doi: 10.1023/A:1026636509713. [DOI] [PubMed] [Google Scholar]
- Fusco DN, Downs JA, Satlin MJ, Pahuja M, Ramos L, Barie PS, Fleckenstein L, Murray HW. Non-oral treatment with ivermectin for disseminated strongyloidiasis. Am J Trop Med Hyg. 2010;83(4):879–883. doi: 10.4269/ajtmh.2010.10-0258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nomura J, Rekrut K. Strongyloides stercoralis hyperinfection syndrome in a patient with AIDS: diagnosis by fluorescent microscopy. Clin inf dis: Inf Dis Soc Am. 1996;22(4):736. doi: 10.1093/clinids/22.4.736. [DOI] [PubMed] [Google Scholar]
- Goldman DE, Grier JF, Ball BE, Abreo F, Abreo KD. A 72-year-old woman with non-Hodgkin’s lymphoma, dyspnea, vomiting, diarrhea, and eosinophilia. J La State Med Soc: Louisiana State Med Soc. 1995;147(6):243–250. [PubMed] [Google Scholar]
- Gordon SM, Gal AA, Solomon AR, Bryan JA. Disseminated strongyloidiasis with cutaneous manifestations in an immunocompromised host. J Am Acad Dermatol. 1994;31(2 Pt 1):255–259. doi: 10.1016/s0190-9622(94)70158-x. [DOI] [PubMed] [Google Scholar]
- Gulick RM. Reappearance of a remotely acquired infection. AIDS Clin Care. 1997;9(9):70. [PubMed] [Google Scholar]
- Gutierrez Y, Bhatia P, Garbadawala ST, Dobson JR, Wallace TM, Carey TE. Strongyloides stercoralis eosinophilic granulomatous enterocolitis. Am J Surg Pathol. 1996;20(5):603–612. doi: 10.1097/00000478-199605000-00007. [DOI] [PubMed] [Google Scholar]
- Hamilton KW, Abt PL, Rosenbach MA, Bleicher MB, Levine MS, Mehta J, Montgomery SP, Hasz RD, Bono BR, Tetzlaff MT. et al. Donor-derived Strongyloides stercoralis infections in renal transplant recipients. Transplantation. 2011;91(9):1019–1024. doi: 10.1097/TP.0b013e3182115b7b. [DOI] [PubMed] [Google Scholar]
- Hong IS, Zaidi SY, McEvoy P, Neafie RC. Diagnosis of Strongyloides stercoralis in a peritoneal effusion from an HIV-seropositive man. A case report. Acta Cytol. 2004;48(2):211–214. doi: 10.1159/000326318. [DOI] [PubMed] [Google Scholar]
- Jain AK, Agarwal SK, El-Sadr W. Streptococcus bovis bacteremia and meningitis associated with Strongyloides stercoralis colitis in a patient infected with human immunodeficiency virus. Cli inf dis: Inf Dis Soc Am. 1994;18(2):253–254. doi: 10.1093/clinids/18.2.253. [DOI] [PubMed] [Google Scholar]
- Kao D, Murakawa GJ, Kerschmann R, Berger T. Disseminated strongyloidiasis in a patient with acquired immunodeficiency syndrome. Arch Dermatol. 1996;132(8):977–978. doi: 10.1001/archderm.1996.03890320127027. [DOI] [PubMed] [Google Scholar]
- Kothary NN, Muskie JM, Mathur SC. Strongyloides stercoralis hyperinfection. Radiographics: Radiological SocNorth Am Inc. 1999;19(4):1077–1081. doi: 10.1148/radiographics.19.4.g99jl171077. [DOI] [PubMed] [Google Scholar]
- Lambroza A, Dannenberg AJ. Eosinophilic ascites due to hyperinfection with Strongyloides stercoralis. Am J Gastroenterol. 1991;86(1):89–91. [PubMed] [Google Scholar]
- Lemos LB, Qu Z, Laucirica R, Fred HL. Hyperinfection syndrome in strongyloidiasis: report of two cases. Ann Diagn Pathol. 2003;7(2):87–94. doi: 10.1053/adpa.2003.50019. [DOI] [PubMed] [Google Scholar]
- Lin AL, Kessimian N, Benditt JO. Restrictive pulmonary disease due to interlobular septal fibrosis associated with disseminated infection by Strongyloides stercoralis. Am J Respir Crit Care Med. 1995;151(1):205–209. doi: 10.1164/ajrccm.151.1.7812554. [DOI] [PubMed] [Google Scholar]
- Link K, Orenstein R. Bacterial complications of strongyloidiasis: Streptococcus bovis meningitis. South Med J. 1999;92(7):728–731. doi: 10.1097/00007611-199907000-00016. [DOI] [PubMed] [Google Scholar]
- Malhotra A, Kochar T, Rangasetty UC. A perfect host. Intern Med J. 2008;38(11):869–870. doi: 10.1111/j.1445-5994.2008.01782.x. [DOI] [PubMed] [Google Scholar]
- Schaeffer MW, Buell JF, Gupta M, Conway GD, Akhter SA, Wagoner LE. Strongyloides hyperinfection syndrome after heart transplantation: case report and review of the literature. J Heart Lung Transpl: Int Soc Heart Transpl. 2004;23(7):905–911. doi: 10.1016/j.healun.2003.06.008. [DOI] [PubMed] [Google Scholar]
- Tarr PE, Miele PS, Peregoy KS, Smith MA, Neva FA, Lucey DR. Case report: Rectal adminstration of ivermectin to a patient with Strongyloides hyperinfection syndrome. Am J Trop Med Hyg. 2003;68(4):453–455. [PubMed] [Google Scholar]
- Marty FM, Lowry CM, Rodriguez M, Milner DA, Pieciak WS, Sinha A, Fleckenstein L, Baden LR. Treatment of human disseminated strongyloidiasis with a parenteral veterinary formulation of ivermectin. Clin Inf Dis: Inf Dis Soc Am. 2005;41(1):e5–e8. doi: 10.1086/430827. [DOI] [PubMed] [Google Scholar]
- Miller MA, Church LW, Salgado CD. Strongyloides hyperinfection: a treatment dilemma. Am J Med Sci. 2008;336(4):358–361. doi: 10.1097/MAJ.0b013e31815cff89. [DOI] [PubMed] [Google Scholar]
- Mizuno S, Iida T, Zendejas I, Martin TD, Schain DC, Turner B, Fujita S. Strongyloides hyperinfection syndrome following simultaneous heart and kidney transplantation. Transplant Int: J European Soc Organ Transplant. 2009;22(2):251–253. doi: 10.1111/j.1432-2277.2008.00767.x. [DOI] [PubMed] [Google Scholar]
- Morgello S, Soifer FM, Lin CS, Wolfe DE. Central nervous system Strongyloides stercoralis in acquired immunodeficiency syndrome: a report of two cases and review of the literature. Acta Neuropathol. 1993;86(3):285–288. doi: 10.1007/BF00304143. [DOI] [PubMed] [Google Scholar]
- Morrell MR, Dallas J, Kollef MH. A 50-year-old woman with abdominal pain and respiratory failure 3 months after kidney transplantation. Chest. 2008;134(2):442–446. doi: 10.1378/chest.07-2754. [DOI] [PubMed] [Google Scholar]
- Newton RC, Limpuangthip P, Greenberg S, Gam A, Neva FA. Strongyloides stercoralis hyperinfection in a carrier of HTLV-I virus with evidence of selective immunosuppression. Am J Med. 1992;92(2):202–208. doi: 10.1016/0002-9343(92)90113-P. [DOI] [PubMed] [Google Scholar]
- Gupta S, Jain A, Fanning TV, Couriel DR, Jimenez CA, Eapen GA. An unusual cause of alveolar hemorrhage post hematopoietic stem cell transplantation: a case report. BMC Cancer. 2006;6:87. doi: 10.1186/1471-2407-6-87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perazella MA, Sadigh M. Acute nonspecific illness in an AIDS patients with dysphagia. Hosp Pract (Off Ed) 1994;29(11):39. doi: 10.1080/21548331.1994.11443104. 43, 47. [DOI] [PubMed] [Google Scholar]
- Phelps KR, Ginsberg SS, Cunningham AW, Tschachler E, Dosik H. Case report: adult T-cell leukemia/lymphoma associated with recurrent strongyloides hyperinfection. Am J Med Sci. 1991;302(4):224–228. doi: 10.1097/00000441-199110000-00006. [DOI] [PubMed] [Google Scholar]
- Qazilbash MH, Ueno NT, Hosing C, De Lima M, Cortes J, Massaro A, Rivera Z, Deavers M, Adachi JA, Champlin RE. Strongyloidiasis after unrelated nonmyeloablative allogeneic stem cell transplantation. Bone Marrow Transplant. 2006;38(5):393–394. doi: 10.1038/sj.bmt.1705448. [DOI] [PubMed] [Google Scholar]
- Purvis RS, Beightler EL, Diven DG, Sanchez RL, Tyring SK. Strongyloides stercoralis hyperinfection. Int J Dermatol. 1992;31(3):160–164. doi: 10.1111/j.1365-4362.1992.tb03918.x. [DOI] [PubMed] [Google Scholar]
- Krishnamurthy R, Dincer HE, Whittemore D. Strongyloides stercoralis hyperinfection in a patient with rheumatoid arthritis after anti-TNF-alpha therapy. J Clin Rheumatology: Rheumatic & musculoskeletal dis. 2007;13(3):150–152. doi: 10.1097/RHU.0b013e3180690933. [DOI] [PubMed] [Google Scholar]
- Reddy TS, Myers JW. Syndrome of inappropriate secretion of antidiuretic hormone and nonpalpable purpura in a woman with Strongyloides stercoralis hyperinfection. Am Journal Med Sci. 2003;325(5):288–291. doi: 10.1097/00000441-200305000-00007. [DOI] [PubMed] [Google Scholar]
- Gorman SR, Craven DE. Images in clinical medicine. Strongyloides stercoralis hyperinfection. New England J Med. 2008;359(11):e12. doi: 10.1056/NEJMicm066791. [DOI] [PubMed] [Google Scholar]
- Reiman S, Fisher R, Dodds C, Trinh C, Laucirica R, Whigham CJ. Mesenteric arteriographic findings in a patient with strongyloides stercoralis hyperinfection. JVIR. 2002;13(6):635–638. doi: 10.1016/S1051-0443(07)61660-1. [DOI] [PubMed] [Google Scholar]
- Roxby AC, Gottlieb GS, Limaye AP. Strongyloidiasis in transplant patients. Clin Inf Dis: Inf Dis So Am. 2009;49(9):1411–1423. doi: 10.1086/630201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patel G, Arvelakis A, Sauter BV, Gondolesi GE, Caplivski D, Huprikar S. Strongyloides hyperinfection syndrome after intestinal transplantation. Transpl inf Dis: J Transplant Soc. 2008;10(2):137–141. doi: 10.1111/j.1399-3062.2007.00256.x. [DOI] [PubMed] [Google Scholar]
- Schindzielorz A, Edberg SC, Bia FJ. Strongyloides stercoralis hyperinfection and central nervous system involvement in a patient with relapsing polychondritis. Southern Med J. 1991;84(8):1055–1057. doi: 10.1097/00007611-199108000-00030. [DOI] [PubMed] [Google Scholar]
- Lichtenberger P, Rosa-Cunha I, Morris M, Nishida S, Akpinar E, Gaitan J, Tzakis A, Doblecki-Lewis S. Hyperinfection strongyloidiasis in a liver transplant recipient treated with parenteral ivermectin. Transplant Inf Disease: J Transplant SocS. 2009;11(2):137–142. doi: 10.1111/j.1399-3062.2008.00358.x. [DOI] [PubMed] [Google Scholar]
- Agarwal VK, Khurana HS, Le HX, Mathisen G, Kamangar N. 30-year-old HIV-positive female with diffuse alveolar hemorrhage. J Int Care Med. 2009;24(3):200–204. doi: 10.1177/0885066609332583. [DOI] [PubMed] [Google Scholar]
- Balagopal A, Mills L, Shah A, Subramanian A. Detection and treatment of Strongyloides hyperinfection syndrome following lung transplantation. Transplant Inf Dis: J Transplant Soc. 2009;11(2):149–154. doi: 10.1111/j.1399-3062.2009.00375.x. [DOI] [PubMed] [Google Scholar]
- Simpson WG, Gerhardstein DC, Thompson JR. Disseminated Strongyloides stercoralis infection. Southern Med J. 1993;86(7):821–825. doi: 10.1097/00007611-199307000-00022. [DOI] [PubMed] [Google Scholar]
- Huston JM, Eachempati SR, Rodney JR, Cayci C, Fusco D, Mathew M, Shou J, Goldstein MJ, Kapur S, Barie PS. Treatment of Strongyloides stercoralis hyperinfection-associated septic shock and acute respiratory distress syndrome with drotrecogin alfa (activated) in a renal transplant recipient. Transplant Inf Dis: J Transplant Soc. 2009;11(3):277–280. doi: 10.1111/j.1399-3062.2009.00386.x. [DOI] [PubMed] [Google Scholar]
- Khasawneh F, Sreedhar R, Chundi V. Strongyloides hyperinfection: an unusual cause of respiratory failure. Ann Intern Med. 2009;150(8):570–571. doi: 10.7326/0003-4819-150-8-200904210-00019. [DOI] [PubMed] [Google Scholar]
- Thompson JR, Berger R. Fatal adult respiratory distress syndrome following successful treatment of pulmonary strongyloidiasis. Chest. 1991;99(3):772–774. doi: 10.1378/chest.99.3.772. [DOI] [PubMed] [Google Scholar]
- Aregawi D, Lopez D, Wick M, Scheld WM, Schiff D. Disseminated strongyloidiasis complicating glioblastoma therapy: a case report. J Neurooncol. 2009;94(3):439–443. doi: 10.1007/s11060-009-9878-4. [DOI] [PubMed] [Google Scholar]
- Apewokin S, Steciuk M, Griffin S, Jhala D. Strongyloides hyperinfection diagnosed by bronchoalveolar lavage in an immunocompromized host. Cytopathology: Journal of the British Soc Clin Cytol. 2010;21(5):345–347. doi: 10.1111/j.1365-2303.2010.00765.x. [DOI] [PubMed] [Google Scholar]
- Upadhyay D, Corbridge T, Jain M, Shah R. Pulmonary hyperinfection syndrome with Strongyloides stercoralis. Am J Med. 2001;111(2):167–169. doi: 10.1016/s0002-9343(01)00708-2. [DOI] [PubMed] [Google Scholar]
- Basile A, Simzar S, Bentow J, Antelo F, Shitabata P, Peng SK, Craft N. Disseminated Strongyloides stercoralis: hyperinfection during medical immunosuppression. J Am Acad Dermatol. 2010;63(5):896–902. doi: 10.1016/j.jaad.2009.09.037. [DOI] [PubMed] [Google Scholar]
- Vadlamudi RS, Van Dort M, Barklow T, Byrd RP Jr, Moorman JP. Strongyloides hyperinfection syndrome complicating (ectopic) Cushing syndrome. Southern Med J. 2008;101(7):750–752. doi: 10.1097/SMJ.0b013e31817a836e. [DOI] [PubMed] [Google Scholar]
- Wang BY, Krishnan S, Isenberg HD. Mortality associated with concurrent strongyloidosis and cytomegalovirus infection in a patient on steroid therapy. Mount Sinai J Med New York. 1999;66(2):128–132. [PubMed] [Google Scholar]
- Williams BT, Guerry-Force ML. Disseminated strongyloidiasis in a World War II Veteran with metastatic undifferentiated carcinoma of neuroendocrine type. Southern Med J. 1992;85(10):1023–1026. doi: 10.1097/00007611-199210000-00025. [DOI] [PubMed] [Google Scholar]
- Wirk B, Wingard JR. Strongyloides stercoralis hyperinfection in hematopoietic stem cell transplantation. Transplant Inf Dis: J Transplant Soc. 2009;11(2):143–148. doi: 10.1111/j.1399-3062.2008.00360.x. [DOI] [PubMed] [Google Scholar]
- Grein JD, Mathisen GE, Donovan S, Fleckenstein L. Serum ivermectin levels after enteral and subcutaneous administration for Strongyloides hyperinfection: a case report. Scandinavian J Inf Dis. 2010;42(3):234–236. doi: 10.3109/00365540903443165. [DOI] [PubMed] [Google Scholar]
- Martin SJ, Cohen PR, MacFarlane DF, Grossman ME. Cutaneous manifestations of Strongyloides stercoralis hyperinfection in an HIV-seropositive patient. Skinmed. 2011;9(3):199–202. [PubMed] [Google Scholar]
- Weiser JA, Scully BE, Bulman WA, Husain S, Grossman ME. Periumbilical parasitic thumbprint purpura: strongyloides hyperinfection syndrome acquired from a cadaveric renal transplant. Transplant Inf Dis: J Transplant Soc. 2011;13(1):58–62. doi: 10.1111/j.1399-3062.2010.00516.x. [DOI] [PubMed] [Google Scholar]
- Lessnau KD, Can S, Talavera W. Disseminated Strongyloides stercoralis in human immunodeficiency virus-infected patients. Treatment failure and a review of the literature. Chest. 1993;104(1):119–122. doi: 10.1378/chest.104.1.119. [DOI] [PubMed] [Google Scholar]
- Ali HA, Walkenstein M. Bilateral nodular pulmonary infiltrates in an immunocompromised host. Thorax. 2008;63(8):746–753. doi: 10.1136/thx.2007.090100. [DOI] [PubMed] [Google Scholar]
- Hughes R, McGuire G. Delayed diagnosis of disseminated strongyloidiasis. Intensive Care Med. 2001;27(1):310–312. doi: 10.1007/s001340000798. [DOI] [PubMed] [Google Scholar]
- Lagace-Wiens PR, Harding GK. A Canadian immigrant with coinfection of Strongyloides stercoralis and human T-lymphotropic virus 1. CMAJ. 2007;177(5):451–453. doi: 10.1503/cmaj.070126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leung V, Al-Rawahi GN, Grant J, Fleckenstein L, Bowie W. Case report: failure of subcutaneous ivermectin in treating Strongyloides hyperinfection. Am J Trop Med Hyg. 2008;79(6):853–855. [PubMed] [Google Scholar]
- Lim S, Katz K, Krajden S, Fuksa M, Keystone JS, Kain KC. Complicated and fatal Strongyloides infection in Canadians: risk factors, diagnosis and management. CMAJ. 2004;171(5):479–484. doi: 10.1503/cmaj.1031698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peters L, McCarthy AE, Faught C. Secondary Strongyloides stercoralis prophylaxis in patients with human T-cell lymphotropic virus type 1 infection: report of two cases. IJID: Int Soc Inf Dis. 2009;13(6):e501–e503. doi: 10.1016/j.ijid.2009.02.009. [DOI] [PubMed] [Google Scholar]
- Rawat B, Simons ME. Strongyloides stercoralis hyperinfestation. Another cause of focal hepatic lesions. Clin Imaging. 1993;17(4):274–275. doi: 10.1016/0899-7071(93)90069-Y. [DOI] [PubMed] [Google Scholar]
- Turner SA, Maclean JD, Fleckenstein L, Greenaway C. Parenteral administration of ivermectin in a patient with disseminated strongyloidiasis. Am J Trop Med Hyg. 2005;73(5):911–914. [PubMed] [Google Scholar]
- Vandebosch S, Mana F, Goossens A, Urbain D. Strongyloides Stercoralis infection associated with repititive bacterial meningitis and SIADH: a case report. Acta gastro-enterologica Belgica. 2008;71(4):413–417. [PubMed] [Google Scholar]
- Collet F, Favory R, Augusto D, Moukassa D, Dutoit E, Mathieu D. [Massive haemoptysis associated with pulmonary Strongyloides stercoralis hyperinfestation] Rev Mal Respir. 2005;22(5 Pt 1):815–818. doi: 10.1016/s0761-8425(05)85640-2. [DOI] [PubMed] [Google Scholar]
- Couprie R, Maslo C, Bouchaud O, Matheron S, Saimot AG, Coulaud JP. [Disseminated anguilluliasis in HIV infection. A new case] Presse Med. 1993;22(20):968. [PubMed] [Google Scholar]
- Daoudal P, Ribier G, Numeric P, Desbois N, Ramialison C. [Disseminated strongyloidiasis, a rare cause of multiple organ failure] Presse Med. 2002;31(26):1216–1217. [PubMed] [Google Scholar]
- Gloro R, Ollivier-Hourmand I, Morin-Fatome A, Rousselot P, Le Moel G, Dao T. [Disseminated strongyloidiasis associated with pulmonary fibrosis and gastrointestinal bleeding] Gastroenterol Clin Biol. 2004;28(12):1287–1290. doi: 10.1016/S0399-8320(04)95223-2. [DOI] [PubMed] [Google Scholar]
- Hovette P, Tuan JF, Camara P, Lejean Y, Lo N, Colbacchini P. [Pulmonary strongyloidiasis complicated by E. coli meningitis in a HIV-1 and HTLV-1 positive patient] Presse Med. 2002;31(22):1021–1023. [PubMed] [Google Scholar]
- Marsan C, Marais MH, Sollet JP, Le Turdu F, Guerin PH, Garcia R, Bleichner G. Disseminated strongyloidiasis: a case report. Cytopathology: J British Soc Clin Cytol. 1993;4(2):123–126. doi: 10.1111/j.1365-2303.1993.tb00525.x. [DOI] [PubMed] [Google Scholar]
- Mattioni S, Valin N, Cracco C, Thellier M, Danis M, Caumes E. Fatal relapse of disseminated strongyloidiasis in an HIV-positive patient, despite ivermectin treatment. Ann Trop Med Parasitol. 2008;102(8):693–698. doi: 10.1179/136485908X337616. [DOI] [PubMed] [Google Scholar]
- Mejia JH, Denis M, Leleu G, Roux P, Mayaud C, Akoun G. [Acute respiratory insufficiency caused by hyperinfestation with strongyloides. BALF diagnosis and favourable outcome] Rev Pneumol Clin. 1992;48(2):75–78. [PubMed] [Google Scholar]
- Pacanowski J, Santos MD, Roux A, LEM C, Guillot J, Lavarde V, Cornet M. Subcutaneous ivermectin as a safe salvage therapy in Strongyloides stercoralis hyperinfection syndrome: a case report. Am J Trop Med Hyg. 2005;73(1):122–124. [PubMed] [Google Scholar]
- Pinatelle P, De Monbrison F, Bedock B. [Disseminated strongyloidiasis with parasitemia in a patient under corticosteroid-treatment] Med Mal Infect. 2009;39(4):267–269. doi: 10.1016/j.medmal.2008.11.005. [DOI] [PubMed] [Google Scholar]
- Quinio D, Moalic E, Masure O, Renault A, Le Flohic AM. [Pulmonary manifestations of malignant strongyloidiasis] Rev Mal Respir. 2002;19(2 Pt1):265–266. [PubMed] [Google Scholar]
- Said S, Nevez G, Moriniere P, Fournier A, Raccurt CP. [Hemodialysis and strongyloidiasis: a presumed cause of eosinophilia able to mask the other] Nephrologie. 1999;20(6):343–346. [PubMed] [Google Scholar]
- Hauber HP, Galle J, Chiodini PL, Rupp J, Birke R, Vollmer E, Zabel P, Lange C. Fatal outcome of a hyperinfection syndrome despite successful eradication of Strongyloides with subcutaneous ivermectin. Infection. 2005;33(5–6):383–386. doi: 10.1007/s15010-005-5060-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steiner B, Riebold D, Wolff D, Freund M, Reisinger EC. Strongyloides stercoralis eggs in a urethral smear after bone marrow transplantation. Clin Inf Dis: Inf Dis Soc Am. 2002;34(9):1280–1281. doi: 10.1086/339753. [DOI] [PubMed] [Google Scholar]
- Almasidou D, Maniatis M, Vassiou K, Damani E, Vakalis N, Fesoulidis I, Gourgoulianis KI. Strongyloides hyperinfection in a patient with sarcoidosis. Respirology. 2003;8(1):105–106. doi: 10.1046/j.1440-1843.2003.00429.x. [DOI] [PubMed] [Google Scholar]
- Bamias G, Toskas A, Psychogiou M, Delladetsima I, Siakavellas SI, Dimarogona K, Daikos GL. Strongyloides hyperinfection syndrome presenting as enterococcal meningitis in a low-endemicity area. Virulence. 2010;1(5):468–470. doi: 10.4161/viru.1.5.12703. [DOI] [PubMed] [Google Scholar]
- Kosmadakis G, Georgoulias C, Filiopoulos V, Stefanou I, Smirloglou D, Michail S. Lethal Strongyloides stercoralis superinfection in an immunocompromised patient. Ren Fail. 2010;32(6):750–752. doi: 10.3109/0886022X.2010.486490. [DOI] [PubMed] [Google Scholar]
- Casati A, Cornero G, Muttini S, Tresoldi M, Gallioli G, Torri G. Hyperacute pneumonitis in a patient with overwhelming Strongyloides stercoralis infection. Eur J Anaesthesiol. 1996;13(5):498–501. doi: 10.1097/00003643-199609000-00014. [DOI] [PubMed] [Google Scholar]
- Gulletta M, Chatel G, Pavia M, Signorini L, Tebaldi A, Bombana E, Carosi G. AIDS and strongyloidiasis. Int J STD AIDS. 1998;9(7):427–429. doi: 10.1258/0956462981922421. [DOI] [PubMed] [Google Scholar]
- Mariotta S, Pallone G, Li Bianchi E, Gilardi G, Bisetti A. Strongyloides stercoralis hyperinfection in a case of idiopathic pulmonary fibrosis. Panminerva Med. 1996;38(1):45–47. [PubMed] [Google Scholar]
- Pampiglione S, Pampiglione E, Di Stefano MA. [Strongyloides stercoralis hyperinfection with encephalitis manifestations] Pathologica. 1993;85(1096):195–204. [PubMed] [Google Scholar]
- Rotolo U, Scarlata F, Giordano S, Tortorici C, Bono L, Coglitore M, Faraci C, Infurnari L, Rubino R, Romano A. [Nephrotic syndrome and Gram-negative sepsis in a patient with strongyloidiasis: a case report] Le infezioni in medicina: rivista periodica di eziologia, epidemiologia, diagnostica, clinica e terapia delle patologie infettive. 2007;15(1):59–62. [PubMed] [Google Scholar]
- Sidoni A, Polidori GA, Alberti PF, Scionti L. Fatal Strongyloides stercoralis hyperinfection diagnosed by Papanicolaou-stained sputum smears. Pathologica. 1994;86(1):87–90. [PubMed] [Google Scholar]
- Lanzafame M, Faggian F, Lattuada E, Antolini D, Vento S. Strongyloidiasis in an HIV-1-infected patient after highly active antiretroviral therapy-induced immune restoration. J Infect Dis. 2005;191(6):1027. doi: 10.1086/428099. [DOI] [PubMed] [Google Scholar]
- Brugemann J, Kampinga GA, Riezebos-Brilman A, Stek CJ, Edel JP, van der Bij W, Sprenger HG, Zijlstra F. Two donor-related infections in a heart transplant recipient: one common, the other a tropical surprise. J Heart Lung Transplant: Int Soc Heart Transplant. 2010;29(12):1433–1437. doi: 10.1016/j.healun.2010.08.002. [DOI] [PubMed] [Google Scholar]
- Grijsen M, van den Berk G, Hoekstra E, Terpstra W, Veldman S, Jansen J. Intestinal strongyloidiasis as a presenting symptom of HTLV-1-associated adult T-cell leukemia/lymphoma. Endoscopy. 2009;41(Suppl 2):E271–E272. doi: 10.1055/s-0029-1215068. [DOI] [PubMed] [Google Scholar]
- Janssen R, Vlaminckx BJ, Seldenrijk CA, Voorn GP, Grutters JC. Strongyloides stercoralis hyperinfection mimicking accelerated form of idiopathic pulmonary fibrosis. Lancet Inf Dis. 2008;8(7):456. doi: 10.1016/S1473-3099(08)70155-5. [DOI] [PubMed] [Google Scholar]
- Van Hattem S, Schuttelaar ML. Disseminated strongyloidiasis caused by heart donor-to-host transmission presenting with purpura. Clin Exp Dermatol. 2010;35(4):e149–e150. doi: 10.1111/j.1365-2230.2009.03740.x. [DOI] [PubMed] [Google Scholar]
- Gomez J, Plaza V, Munoz C, Franquet T. [Hyperinfection by Strongyloides stercoralis and other pathogens in a patient with chronic obstructive airways disease] Medicina clinica. 1997;109(15):609. [PubMed] [Google Scholar]
- Llagunes J, Mateo E, Pena JJ, Carmona P, De Andres J. [Hyperinfection caused by Strongyloides stercoralis] Medicina intensiva/Sociedad Espanola de Medicina Intensiva y Unidades Coronarias. 2010;34(5):353–356. doi: 10.1016/j.medin.2009.06.006. [DOI] [PubMed] [Google Scholar]
- Lopez Gallardo A, Diez Garcia F, Yelamos F, Orozco F. [Hyperinfection by Strongyloides stercoralis in a patient with ulcerative colitis] Enferm Infecc Microbiol Clin. 1997;15(5):273. [PubMed] [Google Scholar]
- Mayayo E, Gomez-Aracil V, Azua-Blanco J, Azua-Romeo J, Capilla J, Mayayo R. Strongyloides stercolaris infection mimicking a malignant tumour in a non-immunocompromised patient. Diagnosis by bronchoalveolar cytology. J Clin Pathol. 2005;58(4):420–422. doi: 10.1136/jcp.2004.017756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rodriguez-Hernandez MJ, Ruiz-Perez-Pipaon M, Canas E, Bernal C, Gavilan F. Strongyloides stercoralis hyperinfection transmitted by liver allograft in a transplant recipient. Am J Transplant: J Am Soc Transplant Am Soc Transplant Sur. 2009;9(11):2637–2640. doi: 10.1111/j.1600-6143.2009.02828.x. [DOI] [PubMed] [Google Scholar]
- Rojo-Marcos G, Cuadros-Gonzalez J, Gonzalez-Juarez MJ, Gomez-Ayerbe C. [Strongyloides stercoralis hyperinfection syndrome in a Colombian patient receiving immunosuppressive treatment] Enferm Infecc Microbiol Clin. 2009;27(7):432–434. doi: 10.1016/j.eimc.2008.11.015. [DOI] [PubMed] [Google Scholar]
- Sauca Subias G, Barrufet Barque P, Besa Beringues A, Rodriguez Ramos E. [Strongyloides stercoralis hyperinfection in a patient with acquired immunodeficiency syndrome] An Med Interna. 2005;22(3):139–141. doi: 10.4321/s0212-71992005000300009. [DOI] [PubMed] [Google Scholar]
- Tirado MD, Gil M, Galiano J, Pardo F, Moreno R, Del Busto AG, Sabater S, Gomila B. [Respiratory and renal insufficiency in a COPD patient receiving corticoid treatment] Enferm Infecc Microbiol Clin. 2002;20(8):401–402. [PubMed] [Google Scholar]
- Tornero C, Galan A, Garrigos E, Ramos JA, Pastor A. [Hyperinfection by S. stercoralis: membranous glomerulonephritis, double bacteremia and petechiae exanthema] Enferm Infecc Microbiol Clin. 1998;16(10):495–496. [PubMed] [Google Scholar]
- Troncoso Garcia E, Munoz Medina L, Callejas Rubio JL, Lopez Ruz MA. [Klebsiella pneumoniae meningitis, Strongyloides stercoralis infection and HTLV-1] Medicina clinica. 2000;115(4):158. doi: 10.1016/s0025-7753(00)71493-x. [DOI] [PubMed] [Google Scholar]
- Pusztaszeri M, Bouzourene H. [Intestinal and disseminated strongyloidosis: two case studies] Ann Pathol. 2005;25(4):322–326. doi: 10.1016/S0242-6498(05)80137-3. [DOI] [PubMed] [Google Scholar]
- Brown M, Cartledge JD, Miller RF. Dissemination of Strongyloides stercoralis as an immune restoration phenomenon in an HIV-1-infected man on antiretroviral therapy. Int J STD AIDS. 2006;17(8):560–561. doi: 10.1258/095646206778145712. [DOI] [PubMed] [Google Scholar]
- Chiodini PL, Reid AJ, Wiselka MJ, Firmin R, Foweraker J. Parenteral ivermectin in Strongyloides hyperinfection. Lancet. 2000;355(9197):43–44. doi: 10.1016/S0140-6736(99)02744-0. [DOI] [PubMed] [Google Scholar]
- Feely NM, Waghorn DJ, Dexter T, Gallen I, Chiodini P. Strongyloides stercoralis hyperinfection: difficulties in diagnosis and treatment. Anaesthesia. 2010;65(3):298–301. doi: 10.1111/j.1365-2044.2009.06196.x. [DOI] [PubMed] [Google Scholar]
- Gill GV, Beeching NJ, Khoo S, Bailey JW, Partridge S, Blundell JW, Luksza AR. A British Second World War veteran with disseminated strongyloidiasis. T Roy Soc Trop Med H. 2004;98(6):382–386. doi: 10.1016/j.trstmh.2003.11.002. [DOI] [PubMed] [Google Scholar]
- Harcourt-Webster JN, Scaravilli F, Darwish AH. Strongyloides stercoralis hyperinfection in an HIV positive patient. J Clin Pathol. 1991;44(4):346–348. doi: 10.1136/jcp.44.4.346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Orlent H, Crawley C, Cwynarski K, Dina R, Apperley J. Strongyloidiasis pre and post autologous peripheral blood stem cell transplantation. Bone Marrow Transplant. 2003;32(1):115–117. doi: 10.1038/sj.bmt.1704104. [DOI] [PubMed] [Google Scholar]
- Pagliuca A. Strongyloides hyperinfection in adult T-cell leukaemia/lymphoma. British J Haematol. 1999;105(1):1. doi: 10.1111/j.1365-2141.1999.01401.x. [DOI] [PubMed] [Google Scholar]
- Rahim S, Drabu Y, Jarvis K, Melville D. Strongyloidiasis: a mistaken diagnosis and a fatal outcome in a patient with diarrhoea. Trans R Soc Trop Med H. 2005;99(3):215–217. doi: 10.1016/j.trstmh.2004.08.003. [DOI] [PubMed] [Google Scholar]
- Heath T, Riminton S, Garsia R, MacLeod C. Systemic strongyloidiasis complicating HIV: a promising response to ivermectin. Int J STD AIDS. 1996;7(4):294–296. doi: 10.1258/0956462961917843. [DOI] [PubMed] [Google Scholar]
- Lim L, Biggs BA. Fatal disseminated strongyloidiasis in a previously treated patient. Med J Australia. 2001;174(7):355–356. doi: 10.5694/j.1326-5377.2001.tb143315.x. [DOI] [PubMed] [Google Scholar]
- Mak DB. Recurrent bacterial meningitis associated with strongyloides hyperinfection. Med J Australia. 1993;159(5):354. doi: 10.5694/j.1326-5377.1993.tb137883.x. [DOI] [PubMed] [Google Scholar]
- Mak DB. Recurrent bacterial meningitis associated with strongyloides hyperinfection. Med J Aust. 1993;159(5):354. doi: 10.5694/j.1326-5377.1993.tb137883.x. [DOI] [PubMed] [Google Scholar]
- Thomas MC, Costello SA. Disseminated strongyloidiasis arising from a single dose of dexamethasone before stereotactic radiosurgery. Int J Clin Prac. 1998;52(7):520–521. [PubMed] [Google Scholar]
- Kanazawa S, Yamaguchi K, Kinoshita Y, Nomura S. Adult T-cell leukaemia and strongyloidiasis. Eur J Cancer Care (Engl) 2008;17(2):209–210. doi: 10.1111/j.1365-2354.2007.00836.x. [DOI] [PubMed] [Google Scholar]
- Kinjo T, Tsuhako K, Nakazato I, Ito E, Sato Y, Koyanagi Y, Iwamasa T. Extensive intra-alveolar haemorrhage caused by disseminated strongyloidiasis. Int J Parasitol. 1998;28(2):323–330. doi: 10.1016/S0020-7519(97)00162-8. [DOI] [PubMed] [Google Scholar]
- Miyazaki M, Tamura M, Kabashima N, Serino R, Shibata T, Miyamoto T, Furuno Y, Nishio T, Ohara J, Sakurai T. et al. Minimal change nephrotic syndrome in a patient with strongyloidiasis. Clin Exp Nephrol. 2010;14(4):367–371. doi: 10.1007/s10157-010-0273-4. [DOI] [PubMed] [Google Scholar]
- Mori S, Konishi T, Matsuoka K, Deguchi M, Ohta M, Mizuno O, Ueno T, Okinaka T, Nishimura Y, Ito N. et al. Strongyloidiasis associated with nephrotic syndrome. Intern Med. 1998;37(7):606–610. doi: 10.2169/internalmedicine.37.606. [DOI] [PubMed] [Google Scholar]
- Morimoto J, Kaneoka H, Sasatomi Y, Sato YN, Murata T, Ogahara S, Sakata N, Takebayashi S, Naito S, Saito T. Disseminated strongyloidiasis in nephrotic syndrome. Clin Nephrol. 2002;57(5):398–401. [PubMed] [Google Scholar]
- Satoh M, Futami A, Takahira K, Kodaira M, Tanaka T, Kuriki K, Hori E. Severe strongyloidiasis complicated by meningitis and hydrocephalus in an HTLV-1 carrier with increased proviral load. J Infect Chemother. 2003;9(4):355–357. doi: 10.1007/s10156-003-0272-4. [DOI] [PubMed] [Google Scholar]
- Setoyama M, Fukumaru S, Takasaki T, Yoshida H, Kanzaki T. SLE with death from acute massive pulmonary hemorrhage caused by disseminated strongyloidiasis. Scand J Rheumatol. 1997;26(5):389–391. doi: 10.3109/03009749709065706. [DOI] [PubMed] [Google Scholar]
- Wong VW, Leung WK, To KF, Sung JJ. Diarrhoea and rash in a retired farmer. HKMJ, Xianggang yi xue za zhi/Hong Kong Academy of Medicine. 2005;11(5):397–398. [PubMed] [Google Scholar]
- Chiu HH, Lai SL. Fatal meningoencephalitis caused by disseminated strongyloidiasis. Acta Neurol Taiwan. 2005;14(1):24–27. [PubMed] [Google Scholar]
- Hsieh YP, Wen YK, Chen ML. Minimal change nephrotic syndrome in association with strongyloidiasis. Clin Nephrol. 2006;66(6):459–463. doi: 10.5414/cnp66459. [DOI] [PubMed] [Google Scholar]
- Huang MS, Hwang KP, Chiang PC, Hwang JJ. Pulmonary hyperinfection with Strongyloides stercoralis. J Formos Med Asso, Taiwan yi zhi. 1996;95(7):551–554. [PubMed] [Google Scholar]
- Ting YM. Pulmonary strongyloidiasis–case report of 2 cases. Kaohsiung J Med Sci. 2000;16(5):269–274. [PubMed] [Google Scholar]
- Liu HC, Hsu JY, Chang KM. Strongyloides stercoralis hyperinfection presenting with symptoms mimicking acute exacerbation of chronic obstructive pulmonary disease. JCMA. 2009;72(8):442–445. doi: 10.1016/S1726-4901(09)70403-4. [DOI] [PubMed] [Google Scholar]
- Hira PR, Al-Ali F, Shweiki HM, Abdella NA, Johny M, Francis I, Iqbal J, Thompson R, Nevar F. Strongyloidiasis: challenges in diagnosis and management in non-endemic Kuwait. Ann Trop Med Parasitol. 2004;98(3):261–270. doi: 10.1179/000349804225003299. [DOI] [PubMed] [Google Scholar]
- Mokaddas EM, Shati S, Abdulla A, Nampoori NR, Iqbal J, Nair PM, Said T, Abdulhalim M, Hira PR. Fatal strongyloidiasis in three kidney recipients in Kuwait. Med Princ Pract: Int J K U, Health Sci Centre. 2009;18(5):414–417. doi: 10.1159/000226298. [DOI] [PubMed] [Google Scholar]
- Al Maslamani MA, Al Soub HA, Al Khal AL, Al Bozom IA, Abu Khattab MJ, Chacko KC. Strongyloides stercoralis hyperinfection after corticosteroid therapy: a report of two cases. Ann Saudi Med. 2009;29(5):397–401. doi: 10.4103/0256-4947.55172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Uwaydah AK, Al Qadah F. Strongyloides stercoralis hyperinfection in a patient with angioimmunoblastic lymphadenopathy. Postgrad Med J. 1992;68(806):974–975. doi: 10.1136/pgmj.68.806.974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Malnick S, Somin M, Beilinson N, Basevitch A, Bregman G, Zimhony O. Strongyloides hyperinfection in Ethiopian immigrants in Israel. IMAJ. 2009;11(11):660–663. [PubMed] [Google Scholar]
- Somin M, Neogolani V, Zimhony O, Wolpart A, Sokolowski N, Malnick S. Fatal recurrent bacterial meningitis: a complication of chronic Strongyloides infection. Eur J Int Med. 2008;19(6):e42–e43. doi: 10.1016/j.ejim.2007.07.009. [DOI] [PubMed] [Google Scholar]
- Kia EB, Rahimi HR, Mirhendi H, Nilforoushan MR, Talebi A, Zahabiun F, Kazemzadeh H, Meamar AR. A case of fatal strongyloidiasis in a patient with chronic lymphocytic leukemia and molecular characterization of the isolate. Korean J Parasitol. 2008;46(4):261–263. doi: 10.3347/kjp.2008.46.4.261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gulbas Z, Kebapci M, Pasaoglu O, Vardareli E. Successful ivermectin treatment of hepatic strongyloidiasis presenting with severe eosinophilia. South Med J. 2004;97(9):907–910. doi: 10.1097/01.SMJ.0000139936.20116.A7. [DOI] [PubMed] [Google Scholar]
- Incani RN, Hernandez M, Cortez J, Gonzalez ME, Salazar YD. Staphylococcus warneri meningitis in a patient with Strongyloides stercoralis hyperinfection and lymphoma: first report of a case. Rev Inst Med Trop Sao Paulo. 2010;52(3):169–170. doi: 10.1590/s0036-46652010000300011. [DOI] [PubMed] [Google Scholar]
- Chaudhary K, Smith RJ, Himelright IM, Baddour LM. Case report: purpura in disseminated strongyloidiasis. Am J Med Sci. 1994;308(3):186–191. doi: 10.1097/00000441-199409000-00014. [DOI] [PubMed] [Google Scholar]
- Davidson RA. Infection due to Strongyloides stercoralis in patients with pulmonary disease. South Med J. 1992;85(1):28–31. doi: 10.1097/00007611-199201000-00008. [DOI] [PubMed] [Google Scholar]
- Kim J, Joo HS, Ko HM, Na MS, Hwang SH, Im JC. A case of fatal hyperinfective strongyloidiasis with discovery of autoinfective filariform larvae in sputum. Korean J Parasitol. 2005;43(2):51–55. doi: 10.3347/kjp.2005.43.2.51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ochoa MD, Ramirez-Mendoza P, Ochoa G, Vargas MH, Alba-Cruz R, Rico-Mendez FG. [Bronchial nodules produced by Strongyloides stercoralis as the cause of bronchial obstruction] Arch Bronconeumol. 2003;39(11):524–526. doi: 10.1157/13053217. [DOI] [PubMed] [Google Scholar]
- Roman-Velez JM, Martinez-Camacho RN, Alayon-Laguer D, Fernandez-Gonzalez R, Reyes-Sosa R, Santos-Llanos G, Colon-Perez M, Ferrer D. An unusual presentation of alveolar hemorrhage. PCRJ: J Gen Prac Airways Group. 2009;18(4):337–339. doi: 10.4104/pcrj.2009.00049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arsic-Arsenijevic V, Dzamic A, Dzamic Z, Milobratovic D, Tomic D. Fatal Strongyloides stercoralis infection in a young woman with lupus glomerulonephritis. J Nephrol. 2005;18(6):787–790. [PubMed] [Google Scholar]
- Finkielman JD, Grinberg AR, Paz LA, Plana JL, Benchetrit GA, Nicastro MA, Roncoroni AJ. Case report: reactive hemophagocytic syndrome associated with disseminated strongyloidiasis. Am J Med Sci. 1996;312(1):37–39. doi: 10.1097/00000441-199607000-00008. [DOI] [PubMed] [Google Scholar]
- Yun HR, Yoo DH, Lee HS, Kim TH, Ahn MH, Min DY, Park MH, Kim SY. Fatal strongyloides hyper-infection in a patient with rheumatoid arthritis. Clin Exp Rheumatol. 2001;19(2):224. [PubMed] [Google Scholar]
- Koh MS, Leng PH, Eng P, Hwang J. An unusual cause of pulmonary haemorrhage in a patient with rheumatoid arthritis. Ann Acad Med Singap. 2004;33(3):365–367. [PubMed] [Google Scholar]
- Leung VK, Liew CT, Sung JJ. Fatal strongyloidiasis in a patient with ulcerative colitis after corticosteroid therapy. Am J Gastroenterol. 1997;92(8):1383–1384. [PubMed] [Google Scholar]
- Shorman M, Al-Tawfiq JA. Strongyloides stercoralis hyperinfection presenting as acute respiratory failure and Gram-negative sepsis in a patient with astrocytoma. IJID: Int Soc Inf Dis. 2009;13(5):e288–e291. doi: 10.1016/j.ijid.2008.11.019. [DOI] [PubMed] [Google Scholar]
- Fasih N, Irfan S, Sheikh U, Beg MS. A fatal case of gram negative bacterial sepsis associated with disseminated strongyloidiasis in an immunocompromised patient. JPMA. 2008;58(2):91–92. [PubMed] [Google Scholar]
- Seet RC, Lau LG, Tambyah PA. Strongyloides hyperinfection and hypogammaglobulinemia. Clin Diagn Lab Immunol. 2005;12(5):680–682. doi: 10.1128/CDLI.12.5.680-682.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Czachor JS, Jonas AP. Transmission of Strongyloides steracolis person to person. J Travel Med. 2000;7(4):211–212. doi: 10.2310/7060.2000.00063. [DOI] [PubMed] [Google Scholar]
- Csermely L, Jaafar H, Kristensen J, Castella A, Gorka W, Chebli AA, Trab F, Alizadeh H, Hunyady B. Strongyloides hyper-infection causing life-threatening gastrointestinal bleeding. WJG. 2006;12(39):6401–6404. doi: 10.3748/wjg.v12.i39.6401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Azira NM, Zeehaida M. Strongyloides stercoralis hyperinfection in a diabetic patient: case report. Trop Biomed. 2010;27(1):115–119. [PubMed] [Google Scholar]
- Vithayasai N, Jennuvat S. Gastrointestinal manifestations in severe strongyloidiasis: report of 3 cases and literature review. Southeast Asian J Trop Med Public Health. 2010;41(1):22–27. [PubMed] [Google Scholar]
- Pornsuriyasak P, Niticharoenpong K, Sakapibunnan A. Disseminated strongyloidiasis successfully treated with extended duration ivermectin combined with albendazole: a case report of intractable strongyloidiasis. Southeast Asian J Trop Med Public Health. 2004;35(3):531–534. [PubMed] [Google Scholar]
- Suvajdzic N, Kranjcic-Zec I, Jovanovic V, Popovic D, Colovic M. Fatal strongyloidosis following corticosteroid therapy in a patient with chronic idiopathic thrombocytopenia. Haematologia. 1999;29(4):323–326. [PubMed] [Google Scholar]
- Hagelskjaer LH. A fatal case of systemic strongyloidiasis and review of the literature. Eur J Clin Microbiol Infect Dis: Eur Soc Clin Microbiol. 1994;13(12):1069–1074. doi: 10.1007/BF02111831. [DOI] [PubMed] [Google Scholar]
- Leang B, Lynen L, Tootill R, Griffiths S, Monchy D. Death caused by strongyloides hyperinfection in a leprosy patient on treatment for a type II leprosy reaction. Lepr Rev. 2004;75(4):398–403. [PubMed] [Google Scholar]
- Wong TY, Szeto CC, Lai FF, Mak CK, Li PK. Nephrotic syndrome in strongyloidiasis: remission after eradication with anthelmintic agents. Nephron. 1998;79(3):333–336. doi: 10.1159/000045058. [DOI] [PubMed] [Google Scholar]
- Adedayo AO, Grell GA, Bellot P. Case study: Fatal strongyloidiasis associated with human T-cell lymphotropic virus type 1 infection. Am J Trop Med Hyg. 2001;65(5):650–651. doi: 10.4269/ajtmh.2001.65.650. [DOI] [PubMed] [Google Scholar]
- Foucan L, Genevier I, Lamaury I, Strobel M. [Aseptic purulent meningitis in two patients co-infected by HTLV-1 and Strongyloides stercoralis] Med Trop (Mars) 1997;57(3):262–264. [PubMed] [Google Scholar]
- N’Dri K, Kouame KE, Sahari R, Hommel D, Hulin A. [Strongyloides stercoralis hyperinfection syndrome with acute meningoencephalitis associated to HTLV-1 and HTLV-2 virus co-infection] Med Mal Infect. 2008;38(3):162–164. doi: 10.1016/j.medmal.2007.11.012. [DOI] [PubMed] [Google Scholar]
- Drug V, Haliga R, Akbar Q, Mihai C, Cijevschi Prelipcean C, Stanciu C. Ascites with Strongyloides stercoralis in a patient with acute alcoholic pancreatitis and liver cirrhosis. JGLD. 2009;18(3):367–369. [PubMed] [Google Scholar]
- Ho PL, Luk WK, Chan AC, Yuen KY. Two cases of fatal strongyloidiasis in Hong Kong. Pathology. 1997;29(3):324–326. doi: 10.1080/00313029700169215. [DOI] [PubMed] [Google Scholar]
- WHO. Model Lists of Essential Medicines. http://www.who.int/medicines/publications/essentialmedicines/en/