

Abstract
We report a case of posttraumatic false aneurysm of popliteal artery after a total knee arthroplasty in an 82-year-old woman. This case is characterized by the distinct history of trauma to the popliteal fossa in the immediate postoperative period and the location of false aneurysm. In addition, the clinical symptoms were similar to those of deep vein thrombosis. The ultrasonographic examination and computed tomography (CT) angiography confirmed the diagnosis on 6th day after the surgery. Ultrasonographic examination 1 day later revealed no increase in the size of false aneurysm. She was treated with open surgical repair. Presenting the difficulty in the diagnosis, unusual location, etiology, and its management is the intention of this case report.
Keywords: Total knee arthroplasty, pseudoaneurysm, popliteal artery
INTRODUCTION
Vascular complications after a total knee arthroplasty (TKA) occur in less than 0.5% of cases.1 It is uncommon, with a reported incidence following TKA ranging from 0.03 to 0.17%.2–7 However, when such a complication does occur, it is potentially limb and life threatening. Popliteal artery pseudoaneurysm is one of the sequelae of popliteal artery trauma and also can cause arterial thrombosis, arteriovenous fistulae, or arterial severance.2–6 We report a case of a false aneurysm of the popliteal artery after a TKA with unusual presentation, difficult diagnosis and successful management.
CASE REPORT
An 82-year-old female was subjected to right TKA for severe osteoarthritis. Right TKA was done using mobile-bearing knee prosthesis (DePuy, Warsaw, Indiana, USA) [Figure 1a and b]. Anterior midline incision with a medial parapatellar arthrotomy approach was used. Total joint was replaced using the standard technique and patellar resurfacing was done. The operation proceeded without any apparent intraoperative complication. Postoperative rehabilitation was started on the 1st postoperative day and consisted of static exercises and continuous passive motion. For postoperative analgesia, IV Fentanyl patient controlled analgesia (PCA) dose 1.5 ml/h, along with intravenous paracetamol (1 g) thrice daily was used. On the 3rd postoperative day, she was disoriented, agitated, and had a fall while trying to get up from bed. The passive range of motion (ROM) was not affected following fall and there was no increase in swelling or hematoma formation. Disorientation continued, and on the 4th postoperative day, she had accidental fall again. She gave a significant history of direct blunt injury to the popliteal fossa with the railing of the bed. Clinically knee was not affected. Electrolyte levels were normal. Hemoglobin dropped from 8.4 gm% (1st postoperative day) to 6.7 gm%, and she was given packed blood cells.
Figure 1.

(a) Postoperative anteroposterior (a) lateral (b) view X-ray of right total knee arthroplasty showing implant in situ
On the 6th postoperative day, patient complained of swelling and severe pain in her calf, refusing to move her right lower limb. Swelling extended from popliteal fossa up to midcalf region and was nonpulsatile. Homan's sign was positive and squeezing of calf was very painful. Distal pulsations were well felt without any neurological deficit. Deep vein thrombosis (DVT) was suspected. Venous Doppler examination of the right lower limb was done, which showed no evidence of DVT. While doing the venous Doppler, the radiologist suspected an arterial injury. The arterial Doppler showed a pseudoaneurysm of the right popliteal artery, of size 3.9 × 2.6 cm, with hematoma collection extending into calf [Figure 2a and b]. Computed tomography (CT) angiography was done for further evaluation and suggested extensive wall calcification of the abdominal aorta and iliac arteries. A 3 × 2.5 cm pseudoaneurysm in relation to the right popliteal artery just above the knee joint was seen [Figure 3a]. Distal runoffs were present and distal vascularity was good [Figure 3b].
Figure 2.
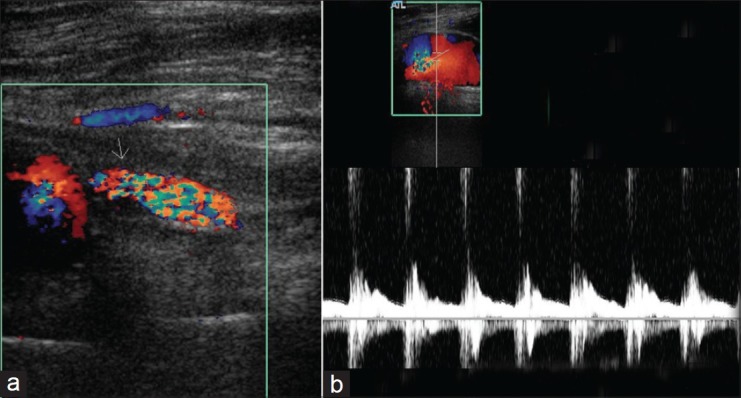
(a) Color Doppler imaging with arrow showing pseudoaneurysm. (b) Color Doppler imaging popliteal artery flow pattern across the pseudoaneurysm
Figure 3a.

CT scan with arrow showing location of pseudoaneurysm (posterior)
Figure 3b.

CT angiography of both lower limbs with distal runoffs and good vascularity
Vascular surgeon opined the need for repair of the rent in the artery causing the aneurysm. A repeat ultrasonographic examination done the next day did not show any increase in the size of the aneurysm. Exploration of the artery was done on 7th postoperative day. Considering the location of false aneurysm, the vascular surgeon decided to go posterior. On exploration, there were significant clots and the rent was found on the posterior surface of the artery of size 2 × 2 mm. The rent in the artery was repaired with 6-0 prolene. The rent was not on the anterior aspect, indicating that the injury to the artery was as a result of the impact on the popliteal region due to a fall in the immediate postoperative period and not an intraoperative incident as is seen in most of the reported cases of popliteal pseudoaneurysm following TKA. After 12 months, the patient remained asymptomatic without any vascular problems. On followup, she had well felt distal pulsations without any clinical evidence of pulsatile swelling in popliteal area. She refused to do followup Doppler or CT angiography.
DISCUSSION
Trauma to popliteal artery in TKA is an intraoperative event. It can present as an acute arterial severance or with arterial thrombosis, pseudoaneurysm, arteriovenous fistula, and occlusion.2–6 Pseudoaneurysm of the popliteal artery is one of the uncommon arterial complications which may present early as a pulsatile mass in the popliteal fossa or remains undetected for a long time.2,3,6 It can present as a painful calf swelling as in DVT.5 Occasionally, it may present very late.7
The reported mechanisms of injury are due to direct trauma to the vessel, like posterior retractor, oscillating saw or pins used to hold the tibial jig, posterior capsular release.2–6 The diagnosis of a post TKA popliteal artery pseudoaneurysm should be suspected clinically, and diagnostic tools such as Doppler ultrasonography and CT angiography should be used to confirm the diagnosis.1,5–16 Repeat ultrasonography is also valuable in determining whether the aneurysm is increasing in size. Smaller pseudoaneurysms which are associated with small defects in the arterial wall can be treated with ultrasound guided compression repair (UGCR). This procedure involves two sittings, week apart, by applying compression at the neck of pseudoaneurysm. Compression is performed with the US transducer itself, a procedure that permits direct and continuous visualization of the vessels. Pressure is applied to pseudoaneurysms in various locations depending on lesion accessibility. Typical protocol includes an initial 10-20-min compression of the pseudoaneurysmal neck; if this is not feasible, the pseudoaneurysm itself is compressed. Compression should eliminate flow within the pseudoaneurysm but permit arterial perfusion to the extremity. Anticoagulation therapy decreases the success rate; therefore, anticoagulants should be discontinued prior to the procedure if possible. Drawbacks of this procedure are long procedure time, discomfort to the patient, recurrence, and rupture of aneurysm. However, due to the nature of the trauma, only a small proportion of these lesions are amenable to percutaneous therapy which is fairly superficial pseudoaneurysm with less hematoma and commonly used for femoral, axillary, and brachial artery pseudoaneurysms.1,4–16 The established treatment for the remainder is open repair with or without popliteal artery bypass grafting with ligation of the native artery. Open repair has its own set of difficulties as it involves operating from a posterior approach and exposing the recently placed prosthesis to infection. It also involves harvesting a venous graft from the contralateral limb. There have been reports of successful treatment of these popliteal pseudoaneurysms with endovascular stenting. Endovascular treatment involves placement of a covered stent across the defect in the popliteal artery.1,13–16 Though no long patient series is available, evidence suggests that endovascular treatment is safe and durable as a treatment modality in the treatment of traumatic popliteal artery pseudoaneurysms and can be performed with an acceptable morbidity rate.
All reported pseudoaneurysms of popliteal artery or inferior geniculate artery are on anterior aspect and due to intraoperative direct injury to the vessel with varied presentation.2–7
Though popliteal pseudoaneurysm is rare, it can be a devastating complication post TKA. We hereby reported an exceptional case where there was trauma to the popliteal fossa due to a fall in the immediate postoperative period probably due to disorientation caused by the use of IV fentanyl and the location of arterial rent was on posterior aspect. This is an unusual presentation of location of injury and etiology to our knowledge. However, intraoperative injury to the popliteal artery is possible.
The clinical presentation of this condition can be confused with that of a postoperative DVT or hematoma formation in early postoperative period and the surgeon should be aware of this condition. The diagnosis is often difficult and can be confirmed by ultrasonography and CT angiography. The treatment options include an open surgical repair or other described noninvasive techniques such as percutaneous embolization or endovascular stenting.
Footnotes
Source of Support: Nil
Conflict of Interest: None
REFERENCES
- 1.Sloan K, Mofidi R, Nagy J, Flett MM, Chakraverty S. Endovascular treatment for traumatic popliteal artery pseudoaneurysms after knee arthroplasty. Vasc Endovascular Surg. 2009;43:286–90. doi: 10.1177/1538574408328664. [DOI] [PubMed] [Google Scholar]
- 2.O’Connor JV, Stocks G, Crabtree JD, Jr, Galasso P, Wallsh E. Popliteal pseudoaneurysm following total knee arthroplasty. J Arthroplasty. 1998;13:830–2. doi: 10.1016/s0883-5403(98)90039-0. [DOI] [PubMed] [Google Scholar]
- 3.Ninomiya JT, Dean JC, Goldberg VM. Injury to the popliteal artery and its anatomic location in total knee arthroplasty. J Arthroplasty. 1999;14:803–9. doi: 10.1016/s0883-5403(99)90029-3. [DOI] [PubMed] [Google Scholar]
- 4.Calligaro KD, Dougherty MJ, Ryan S, Booth RE. Acute arterial complications associated with total hip and knee arthroplasty. J Vasc Surg. 2003;38:1170–7. doi: 10.1016/s0741-5214(03)00918-2. [DOI] [PubMed] [Google Scholar]
- 5.Karkos CD, Thomson GJ, D’Souza SP, Prasad V. False aneurysm of the popliteal artery: A rare complication of total knee replacement. Knee Surg Sports Traumatol Arthrosc. 2000;8:53–5. doi: 10.1007/s001670050011. [DOI] [PubMed] [Google Scholar]
- 6.Vaidhyanath R, Blanshard KS. Case report: Insertion of a covered stent for treatment of a popliteal artery pseudoaneurysm following total knee arthroplasty. Br J Radiol. 2003;76:195–8. doi: 10.1259/bjr/32510074. [DOI] [PubMed] [Google Scholar]
- 7.Ahajjam MA, Ayadi D, Wery D, Lambert J. Percutaneous embolization of a false aneurysm of the tibial anterior artery after total knee arthroplasty. Eur J Orthop Surg Traumatol. 2008;18:391–3. [Google Scholar]
- 8.Davies AJ, Roberts DE. A complication following a total knee arthroplasty. Br J Radiol. 1999;72:317–8. doi: 10.1259/bjr.72.855.10396228. [DOI] [PubMed] [Google Scholar]
- 9.Plagnol P, Diard N, Bruneteau P, Roncheau V. Case report: Pseudoaneurysm of popliteal artery complicating a total knee replacement: A successful percutaneous endovascular treatment. Eur J Vasc Endovasc Surg. 2001;21:81–3. doi: 10.1053/ejvs.2000.1234. [DOI] [PubMed] [Google Scholar]
- 10.Ibrahim M, Booth RE, Jr, Clark TW. Embolization of traumatic pseudoaneurysms after total knee arthroplasty. J Arthroplasty. 2004;19:123–8. doi: 10.1016/j.arth.2003.08.007. [DOI] [PubMed] [Google Scholar]
- 11.Papas TT, Maltezos CK, Papanas N, Antoniou G, Lazarides MK. Popliteal artery pseudoaneurysm after total knee replacement. Vasa. 2007;36:145–58. doi: 10.1024/0301-1526.36.2.145. [DOI] [PubMed] [Google Scholar]
- 12.D’Angelo F, Carrafiello GP, Lagana’ D, Reggiori A, Giorgianni A, Zatti G, et al. Popliteal artery pseudoaneurysm after a revision of total knee arthroplasty: Endovascular treatment with a stent graft. Emerg Radiol. 2007;13:323–7. doi: 10.1007/s10140-006-0553-1. [DOI] [PubMed] [Google Scholar]
- 13.Behnke NM, Cui Q, Orndorff D. Late presentation of a mycotic popliteal artery pseudoaneurysm in the setting of a revised total knee arthroplasty complicated by both prior infection and periprosthetic fracture: A case report. Ann Vasc Surg. 2007;21:519–24. doi: 10.1016/j.avsg.2007.01.009. [DOI] [PubMed] [Google Scholar]
- 14.May J, White GH, Yu W, Waugh R, Stephen MS, Harris JP. Endoluminal repair: A better option for the treatment of complex false aneurysms. Aust N Z J Surg. 1998;68:29–34. doi: 10.1111/j.1445-2197.1998.tb04632.x. [DOI] [PubMed] [Google Scholar]
- 15.Manns RA, Duffield RG. Case report: Intravascular stenting across a false aneurysm of the popliteal artery. Clin Radiol. 1997;52:151–3. doi: 10.1016/s0009-9260(97)80110-9. [DOI] [PubMed] [Google Scholar]
- 16.Mofidi R, Kelman J, Berry O, Bennett S, Murie JA, Dawson AR. Significance of the early postoperative duplex result in infrainguinal vein bypass surveillance. Eur J Vasc Endovasc Surg. 2007;34:327–32. doi: 10.1016/j.ejvs.2007.04.008. [DOI] [PubMed] [Google Scholar]