

Abstract
Background:
High flexion implants have been reported to provide better range of motion (ROM). The few studies analyzing the factors affecting the ROM are scarce. This study aims to find the factors that affect ROM when using a high flex knee design (INDUS knee).
Materials and Methods:
Two hundred and fifty three consecutive patients of total knee arthroplasty (TKA) done by using INDUS knee prosthesis between Sept 2008 and Sept 2009 were included in the study. The cases with osteoarthritis (OA) and Rheumatoid arthritis (RA) were included in study. 5 patients were lost to followup and 248 patients (267 knees, 19 bilateral, 221 OA, and 46 RA) were analyzed for the following factors – sex, age, body mass index (BMI), preoperative ROM, flexion deformity, preoperative total knee score and functional score, time of tourniquet release and patella resurfacing. Subgroup classification using above factors was performed and statistical analysis of effect of all the above factors on final knee ROM was done. Assessment was done preoperatively and at 3 months, 6 months and 1 year postoperatively. The final outcome evaluation was done at one year followup.
Results:
The mean age was 68.2 years (range 40-89 years) with 79 males and 189 females. The mean knee range improved from 97.62 ± 11° to 132 ± 8°. Factors that positively affect ROM of INDUS knee prosthesis at the end of 1 year were preoperative ROM, total knee score and functional score, and diagnosis of osteoarthritis, whereas BMI, preoperative flexion deformity has a negative influence on final flexion at the end of 1 year. Age and gender of the patients, patella resurfacing, and use of two different tourniquet protocols did not affect the final outcome.
Conclusion:
Preoperative ROM and preoperative functional status are the most important factors affecting final range. Patients should be counseled accordingly and made to understand these factors.
Keywords: High flex knee prosthesis, range of motion, total knee arthroplasty
INTRODUCTION
Range of motion (ROM) is the most important outcome that defines the functional ability after total knee arthroplasty (TKA). A minimum range of knee flexion of 90° is essential to daily activities with about 67° required in swing phase, 83° in climbing stairs, 90° in descending stairs, and 93° in rising from a chair.1 Preoperative range of knee motion, etiology, BMI, patient age, and knee society score are among the most important factors that affect the final outcome.2,3 Surgical technique, implant design, and postoperative rehabilitation are also said to affect the final knee ROM.3,4 Conventional total knee designs limited ROM to near 90°.5 Reports of long term followup of PFC have shown average ROM of 101°.6 A large review of TKAs of different designs performed before the end of 1985 and was found that 46% of patients could not flex their knees beyond 90 deg after the surgery.7 Older published series report a final flexion between 100 and 115°.8–11 High flex knee designs have been introduced with improved ROM and ability to reach higher flexion angles.12 Such an outcome is more significant in countries where people are accustomed to squatting and sitting cross legged. Results of the high flex implants have shown a mixed review.13–15 Recent reviews have commented on similar ROM and functional outcome in high flexion and standard implants.16–18 High flexion implants might provide a safer deep flexion and may be better in certain situations like preoperative knee stiffness.19,20 Yet the field of high flexion knee prosthesis is still expanding and more studies are needed. Recently, early results of indigenously developed INDUS knee prosthesis were published with good short term results and improved range of knee motion.21,22 However, both these studies were performed on heterogeneous group of patients and no subgroup analysis was made on the factors affecting the outcome. The aim of this study is to investigate the factors that affect the final ROM achieved following TKA using high flex knee prosthesis and to compare the effect of each factor on early ROM at different time intervals postoperatively.
MATERIALS AND METHODS
An observational study of all the knees, operated with INDUS knee prosthesis in our Institute between Sept 2008 and Sept 2009 was set up. Inclusion criteria were any primary osteoarthritis or rheumatoid arthritis of knee operated with TKA with the chosen prosthesis. Patients with complex knees with ROM less than 50°, severe varus or valgus deformity >20°, or bone defect requiring bone grafting were excluded. This was done to minimize the effect of these factors on the ROM and get a relatively homogeneous cohort. 398 patients (435 knees: 37 bilateral) were screened. A total number of 35 patients (42 knees; 7 bilateral) did not consent for study while 43 patients (51 knees; 8 bilateral) were excluded as they stayed at far away places and regular followup was not feasible. A total number of 67 patients (67 knees) were excluded according to exclusion criteria. Thus, 253 patients (275 knees; 22 bilateral) met the inclusion criteria. One patient suffered from peri-prosthetic fractures during the first 3 months and was subsequently excluded from the study. Two patients (bilateral) developed instability of the knee following a fall but were included in study. Four patients (one bilateral, n=5 knees) were lost to followup. Thus, a total of 248 patients (267 knees; 19 bilateral) were available for final analysis.
All patients underwent TKA using standard median parapatellar approach. A uniform postoperative rehabilitation protocol was employed for every patient. Knee ROM of all patients was evaluated using a standard goniometer.23 Calculation of knee ROM, flexion deformity, and functional score was done by a group of trained outcome assessors who were blinded to the implant used and aim of the study. Knee ROM was assessed preoperatively and at 3 months, 6 months and 1 year postoperatively.
Subgroup analysis was performed dividing the cohort based on following factors: Gender (males/females), preoperative diagnosis (OA/RA), patella Replacement (yes/no), tourniquet release (before or after Closure). Other factors like age, body mass index, preoperative ROM, preoperative flexion deformity, preoperative total Knee score, preoperative total functional score,24 were statistically correlated with the final ROM attained. Gain in ROM from base line was also assessed in various subgroups.
Statistical methods
Paired t-test was used for statistical testing of the difference in mean values in comparing preoperative to postoperative improvement, and a significant difference was found with a risk less than 1%, i.e., P < 0.01.Unpaired t-test was used for subgroup analysis with significant P value <0.01. For analysis of the correlation of the two variants, Pearson correlation coefficient was calculated. With a risk of less than 1%, they were judged as weakly correlated. When the absolute value of the coefficient of correlation was 0.1 or greater, moderately correlated when it was 0.4 or greater, and strongly correlated when it was 0.7 or greater. For analysis of multiple variants, ANOVA test was used.
RESULTS
The mean age was 68.2 years (range 40-89 years) at the time of the surgery. A total of 79 were men and 189 were women. The surgery was performed on 151 right knees and 116 left knees, including 19 patients in whom bilateral surgery was performed. The implant used was posterior stabilized, high flex INDUS knee design. All surgeries were performed through a medial parapatellar approach. All components were cemented. Patella was replaced in 41 patients and patelloplasty done in 227. Cases with relatively good patella cartilage and no grade IV eburnation a patelloplasty was done while in cases with severe cartilage lesion, the patella was replaced. Tourniquet was used in 263 of the 267 knees. Tourniquet was released before closure in 198 patients and after closure in 65 patients based on the surgeons’ preference.
Preoperative diagnosis was osteoarthritis (OA) in 221 subjects (82.8%), rheumatoid arthritis (RA) in 47 subjects (17.2%). Preoperatively the mean ROM was 97.62 ± 11° (range 60 to 110°). This improved postoperatively to 132 ± 8° (range 96-140) [Figures 1 and 2]. A total of 71 knees had ROM >130°, 150 knees had ROM between 120° and 130°, 34 knees had ROM between 100° and 120° and only 12 kneeshad <100°. A total of 205 out of 248 patients (76.6%) patients retained their ability to sit cross legged at final followup. The knee score improved from preoperative 39.4 to postoperative 87.7 while the function score improved from preoperative 46.7 to 89.7. Statistical analysis of ROM, knee score, and function score showed significant improvement postoperatively (P < 0.001 for paired t test).
Figure 1.
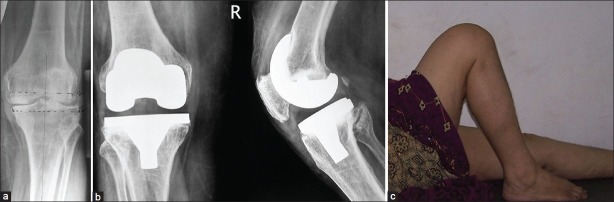
(a) Preoperative radiograph of 63-year-old female with primary osteoarthritis of the knee, (b) One year post surgery radiograph of the knee with INDUS knee prosthesis, (c) Clinical picture showing knee ROM at 1 year followup
Figure 2.
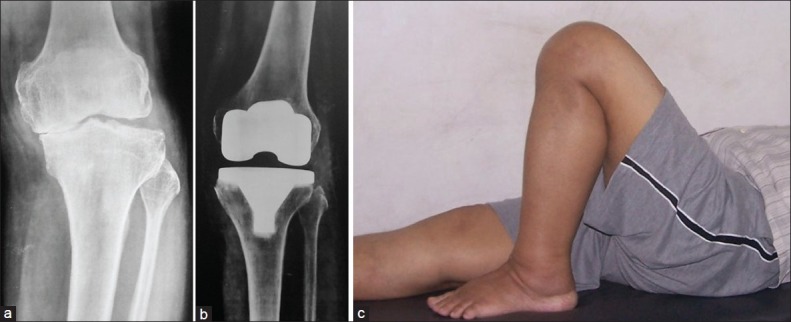
(a) Preoperative radiograph of 71 year old male showing OA changes, (b) Postoperative radiograph showing one year post knee replacement using INDUS knee prosthesis with, (c) Clinical picture showing good knee range of motion
Subgroup analysis
Preoperatively, no significant difference in ROM was noted between the two genders (97.08 ± 23.10° in male patients and 97.12 ± 22.37° in female patients; P = 0.989). The average ROM at 3 months after surgery was 112.44 ± 21.24° in males and 108.66 ± 19.37° in females (P = 0.175). Even though males showed a larger gain in ROM at 6 months (127.39 ± 15.6° in males and 124.17 ± 17.11° in females; P = 0.137) and 1 year (132.76 ± 15.09° in males and 131.76 ± 18.48° in female patients; P = 0.071) after surgery this was not statistically significant.
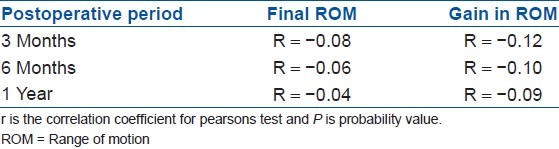
No correlation between age and postoperative ROM of the knee was found. Significant difference in gain in ROM was found in younger age groups at 3 months but this was not observed at 6 month and 1 year period [Table 1].
Table 1.
Correlation between age and range of motion
Body mass index had a weak negative correlation with ROM at 6 months and 1 year after surgery (r = −0.137, P = 0.02 and r = −0.137, and P = 0.02, respectively). However, there was no correlation between BMI and ROM at 3 months (r = −0.115, P = 0.56). This shows that obese patients did not gain much ROM after the initial gain.
There was significant difference in the ROM before surgery in OA and RA group. Preoperatively, the ROM were 99.98 ± 11.34° in OA and 83.88 ± 21° in RA (P < 0.0001). Postoperatively ROM was 120.07° in OA and 117.46° in RA at 3 months after surgery, 125.56° in OA and 123.04° in RA at 6 months, and 135.91 ± 14.2° in OA and 123.98 ± 11.2° in RA at 1 year after surgery, respectively. At each followup, the ROM was greater in the OA group postoperatively but this was significant only at the end of 12 Months (P < 0.01 at 1 year). However, RA group had higher gain in flexion angle from the baseline.
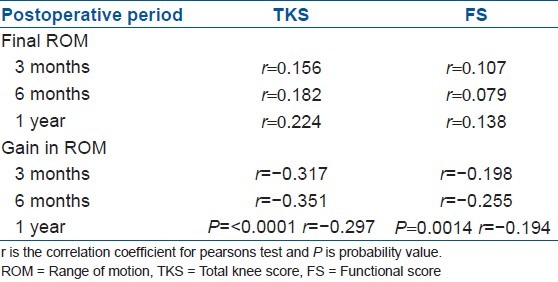
The preoperative TKS and FS were found to have significant influence on both pre and postoperative ROM. There was weak negative correlation between TKS at all time intervals and FS at 6 months and gain in ROM from the preoperative value [Table 2]. Knee score had weak positive correlation with ROM at the end of 1 year. Functional score too correlated positively but this was not statistically significant [Table 2].
Table 2.
Correlation of total knee score and functional score to the final flexion angle and change in ROM from preoperative values
The preoperative ROM had a moderately positive correlation with ROM at 6 months (r = 0.41, P = <0.0001) and was weakly positive at the end of 1 year (r = 0.38, P = <0.0001) after surgery.
When considering the gain in ROM, preoperative ROM had moderately negative correlation at 3 months and 1 year but had strong negative correlation at 6 months (r = −0.631, P = <0.0001 at 3 months, r = −0.71, P = <0.0001 at 6 months and r = −0.69, P = <0.0001 at 1 year). The preoperative flexion deformity (extension angle) had an opposite effect. It had a weak negative correlation with final flexion angle r = −0.263, −0.278, −0.300 at 3, 6, and 12 months, respectively (P < 0.0001) but positive correlation with gain in ROM from baseline values.
There was no difference in preoperative knee flexion when comparing the groups where patella was replaced and the ones where patelloplasty was done. Postoperatively the group in which patella was replaced showed a higher gain in ROM though this was not statistically significant. (P = 0.42, 0.39, and 0.48 respectively at 3, 6, and 12 months).
The group where tourniquet was released after closure had increased tourniquet time by an average of 15 ± 7.8 min. There was a significant gain in ROM in this group at 3 months (P = 0.009) but this was not seen at the end of 6 months and 1 year. (P = 0.10, 0.12, respectively). Thus, when tourniquet was released earlier, the gain in ROM was quicker; however, no long term difference between the two groups was noted.
DISCUSSION
Studies have compared various preoperative and postoperative parameters between high flexion and standard implant.25–35 Factors affecting ROM in an high flexion implant may be different than standard implant. We studied the high flexion Indus knee implant with respect to factors affecting the final ROM and also the functional satisfaction of the patients.
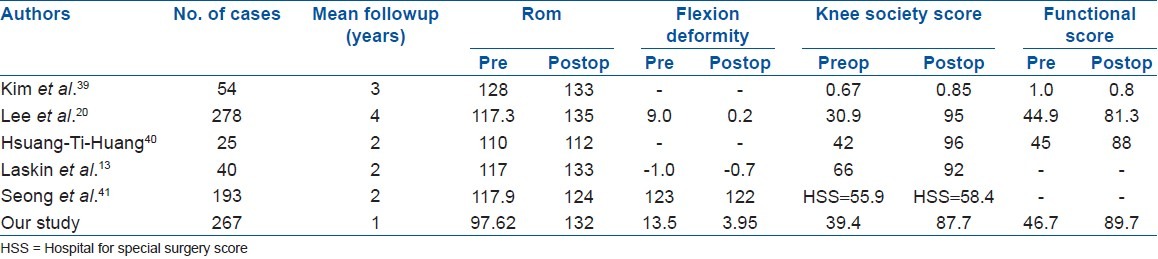
Two prospective series have been published on the INDUS knee prosthesis. First a multicentric trial of 276 patients performed at six centers across India.21 This cohort was followed prospectively for 2 years and was analyzed to clinical and functional outcome. Of the 276 patients (297 knees), 79 knees had flexion above 140°, 167 had a flexion range of 130-140°, 27 had a flexion range of 100-130°, and 24 knees had a flexion <100°, with the mean range of movement being 132.9°. Improvements in the range of movement were retained over time and a total of 205 patients (224 knees, 75.7%) could squat or sit cross-legged at the final followup. The mean knee score and the mean function score were significantly improved from a preoperative value of 39.4 points and 46.7 points to a postoperative value of 87 points and 86 points, respectively. The mean tibiofemoral angle was 8.5° ± 6.9° of varus preoperatively and 5.4° ± 2.2° of valgus (3-7° of valgus) at the final followup, with no loss of alignment noted in any case. Second report was again a prospective cohort of 208 knees and results published in 2010.22 The patients were followedup for average 3.5 years (range, 2.8 years to 4.3 years). The mean knee score and mean function score were significantly improved from preoperative value of 38.6 points and 47.7 points to postoperative value of 90 points and 89 points, respectively (P value <0.05). Out of 208 knees, 60 knees had flexion above 140°, 96 had flexion range 130° to 140°, 32 had flexion range 100° to 130°, and 20 knees had flexion less than 100° with mean range of movement being 133.90°. The mean tibiofemoral angle was 7.9° ± 5.4° of varus preoperatively and 5.2° ± 2.2° of valgus (3° to 6° of valgus) at final followup. In our study the final ROM achieved was mean of 132 ± 8° (range 96-140), flexion deformity improved to a mean of 3.95 ± 3.77 (range 0-13), preoperative alignment increased to 4.8 ± 1.32° (range, 0 to 8) of valgus and the knee score and function score improved postoperatively to 87.7 and 89.7, respectively. Thus, in our series too, the INDUS knee prosthesis had result similar to the earlier INDUS series.The ROM was similar to the other studies on high flexion knee implants [Table 3].
Table 3.
Comparison of our results with other studies of high flexion knee prosthesis
Factors affecting the final range of motion are discussed below
Gender
Harvey et al.28 reported in his study that sex had no correlation in affecting the final knee ROM postoperatively in conventional total knee arthroplasty. Other studies also showed no relation between sex and ROM.6,10 In our study ROM was preoperatively similar in both males and females. At 6 months and 1 year post surgery, we found final ROM to be slightly more in males however this was not statistically significant.
Age
Schurman et al.33 found that gain in ROM was better in younger patients at 3 months post-surgery. Franklin et al.26 reported older age groups to have a poorer outcome when compared to younger ones. Farahini et al. reported univariate analysis showing good correlation (r=-0.102, P-value=0.04) with post operative flexion angle however multivariate analysis showed no significant correlation. In contrast, Anouchi et al.27 reported no correlation between age and postoperative knee ROM. In our study too we found no relation between age and postoperative range of movement at 3 months, 6 month and 1 year time interval (r value).
Body mass index
Obesity has an adverse effect on postoperative knee ROM due to soft tissue impingement between the femur and the tibia, which restricts flexion of the knee.26 Studies show that patients who were obese had higher chances of a poor ROM.28–30 Our study shows that people with lesser BMI gained significant flexion from baseline after the first 3 months till 1 year post surgery. Thus, although the patient with higher BMI did had decreased ROM, the final flexion angle did not correlate with BMI, agreeing with Kotani et al.6 Further studies will be required to assess the relation of body mass index and postoperative ROM in high flexion implants.
Type of disease
Studies have reported that patients suffering from rheumatoid arthritis had poor preoperative ROM compared to osteoarthritis. Harvey et al.30 described the type of disease as the most important factor in predicting ROM after total knee replacement. Ritter and Stringer35 evaluated 145 consecutive TKAs and found that the knee flexion range increased by 2° in RA patients, a non-statistically significant difference. In our study, there was significant difference in preoperative ROM between the OA and RA groups with RA group having lesser preoperative ROM. Postoperatively, the RA group showed a significantly greater increase in ROM in agreement with most published studies.6,30 The final flexion angle was greater in OA group and this was significant at the end of 1 year when compared with RA group. Thus, although patients with RA had better gain in ROM, the final ROM was better in OA group.
Preoperative range of motion
Increased preoperative ROM has proved by several studies that there is a greater postoperative flexion arc achieved by the patient. Kurosaka et al.,36 Harvey et al.30 reported that preoperative ROM of the knee joint was the most important factor with patients with good preoperative ROM showing better final outcome. Our study results demonstrated moderately positive correlation between preoperative flexion and postoperative flexion at 3 months and 6 months, but reduced to a weak positive correlation by the end of 1 year.
Preoperative flexion deformity and postoperative range of motion
A positive correlation between preoperative and postoperative ROM is well established.6,36 In our study, preoperative ROM had positive correlation with postoperative ROM indicating more final ROM in patients with more peroperative ROM. However, preoperative ROM had negative correlation with gain in ROM indicating patients with more preoperative ROM did not gain much range (Preoperative ROM α postoperative ROM/gain in ROM). Kawamura and Bourne5 concluded that preoperative flexion deformity did not correlate with final ROM. In our series patients with greater flexion deformity had significant but weak negative correlation with final ROM and a positive correlation with gain in ROM. Thus, more the preoperative flexion deformity less was the final ROM and more was the gain in ROM with P < 0.0001 at all-time intervals (Preoperative flexion deformity directly proportional to gain in ROM and inversely proportional to final ROM).This correlation of preoperative ROM and flexion deformity with postoperative ROM and gain in ROM is not reported in literature.
Patella resurfacing and tourniquet protocol
We performed the arthroplasty of patellar component in 40 of 267 patients. Our study found that patella resurfacing has no effect on the postoperative ROM in agreement with Burnett et al.37 However, the sample size in our series is much skewed to reach a definitive conclusion. Tourniquet was used in 99% of cases. In these, 202 had tourniquets released before closure and 65 after closure. The range of flexion increased significantly at the end of 3 months but toward the end of 1 year the increase in range had evened out. Wakankar et al.38 found that not using a tourniquet had a beneficial effect on ROM only in early period. In this study, early release of tourniquet was associated with early gain in ROM, but no long term effect was noted.
Scores
Anouchi et al.27 found that most important factor to predict the ROM was the preoperative knee society scores. In our study, patients with good preoperative knee society score were shown to have more final range of flexion however the ones with lower Total knee Score and Functional Score showed higher gain in ROM from the preoperative value. Our study shows that in high flexion implants there is weak correlation between the knee score and final flexion angle but there was a significant correlation between flexion angle and functional score after 1 year. This was similar to findings of other studies and concluded that both preoperative and postoperative scores positively correlate with better postoperative ROM.6,32
No comparison group in our study relatively short followup are the main limitations of the study. Intraoperative factors like ligament balancing, flexion extension gap after bony cuts among others were not considered. However, since this is a series from single institution following a standard technique, other factors can be considered to be comparable.
To conclude use of INDUS Knee Prosthesis in our series had mean final ROM of 132° similar to earlier reports on high flexion achieved by the implant. Factors that positively affected ROM at the end of 1 year were preoperative ROM, total knee score, and functional Score and diagnosis of osteoarthritis whereas BMI, preoperative flexion deformity has a negative influence on final flexion at the end of 1 year. Age and gender of the patients, patella resurfacing and use of two different tourniquet protocols did not affect the final outcome.41
Footnotes
Source of Support: Nil
Conflict of Interest: None
REFERENCES
- 1.Kettelkamp DB, Johnson RJ, Smidt GL, Chao EY, Walker M. An electrogoniometric study of knee motion in normal gait. J Bone Joint Surg Am. 1970;52:775–90. [PubMed] [Google Scholar]
- 2.Laubenthal KN, Smidt GL, Kettelkamp DB. A quantitative analysis of knee motion during activities of daily living. Phys Ther. 1972;52:34–43. doi: 10.1093/ptj/52.1.34. [DOI] [PubMed] [Google Scholar]
- 3.Gatha NM, Clarke HD, Fuchs R, Scuderi GR, Insall JN. Factors affecting postoperative range of motion after total knee arthroplasty. J Knee Surg. 2004;17:196–202. doi: 10.1055/s-0030-1248221. [DOI] [PubMed] [Google Scholar]
- 4.Kawamura H, Bourne RB. Factors affecting range of flexion after total knee arthroplasty. J Orthop Sci. 2001;6:248–52. doi: 10.1007/s007760100043. [DOI] [PubMed] [Google Scholar]
- 5.Insall JN, Ranawat CS, Aglietti P, Shine J. A comparison of four models of total knee-replacement prostheses. J Bone Joint Surg Am. 1976;58:754–65. [PubMed] [Google Scholar]
- 6.Kotani A, Yonekura A, Bourne RB. Factors affecting range of motion after contemporary total knee arthroplasty. J Arthroplasty. 2005;7:850–6. doi: 10.1016/j.arth.2004.12.051. [DOI] [PubMed] [Google Scholar]
- 7.Schurman DJ, Parker JN, Ornstein D. Total condylar knee replacement. J Bone Joint Surg. 1985;67A:100–6. [PubMed] [Google Scholar]
- 8.Hanusch B, Lou TN, Warriner G, Hui A, Gregg P. Functional outcome of PFC Sigma fixed and rotating-platform total knee arthroplasty.A prospective randomised controlled trial. Int Orthop. 2010;34:349–54. doi: 10.1007/s00264-009-0901-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Tew M, Forster IW, Wallace WA. Effect of total knee arthroplasty on maximal flexion. Clin Orthop Relat Res. 1989;247:168–74. [PubMed] [Google Scholar]
- 10.Ishii Y, Matsuda Y, Sakata S, Onda N, Omori G. Primary total knee arthroplasty using the Genesis I total knee prosthesis: A 5- to 10-year followup study. Knee. 2005;12:341–5. doi: 10.1016/j.knee.2004.12.004. [DOI] [PubMed] [Google Scholar]
- 11.Hirsch HS, Lotke PA, Morrison LD. The posterior cruciate ligament in total knee surgery.Save, sacrifice, or substitute? Clin Orthop Relat Res. 1994;309:64–8. [PubMed] [Google Scholar]
- 12.Ranawat AS, Rossi R, Loreti I, Rasquinha VJ, Rodriguez JA, Ranawat CS. Comparison of the PFC Sigma fixed-bearing and rotating-platform total knee arthroplasty in the same patient: Short-term results. J Arthroplasty. 2004;19:35–9. doi: 10.1016/j.arth.2003.08.010. [DOI] [PubMed] [Google Scholar]
- 13.Laskin RS. The effect of a high-flex implant on postoperative flexion after primary total knee arthroplasty. Orthopedics. 2007;30(8 Suppl):86–8. [PubMed] [Google Scholar]
- 14.Ritter MA. High-flexion knee designs: More hype than hope.In the affirmative? J Arthroplasty. 2006;21(4 Suppl 1):40–1. doi: 10.1016/j.arth.2006.02.088. [DOI] [PubMed] [Google Scholar]
- 15.Bin SI, Nam TS. Early results of high-flex total knee arthroplasty: Comparison study at 1 year after surgery. Knee Surg Sports Traumatol Arthrosc. 2007;15:350–5. doi: 10.1007/s00167-006-0202-y. [DOI] [PubMed] [Google Scholar]
- 16.Hamilton WG, Sritulanondha S, Engh CA., Jr Results of prospective, randomized clinical trials comparing standard and high-flexion posterior-stabilized TKA: A focused review. Orthopedics. 2011;34:e 500–3. doi: 10.3928/01477447-20110714-47. [DOI] [PubMed] [Google Scholar]
- 17.Luo SX, Su W, Zhao JM, Sha K, Wei QJ, Li XF. High-flexion vs conventional prostheses total knee arthroplasty: A meta-analysis. J Arthroplasty. 2011;26:847–54. doi: 10.1016/j.arth.2010.09.008. [DOI] [PubMed] [Google Scholar]
- 18.Mehin R, Burnett RS, Brasher PM. Does the new generation of high-flex knee prostheses improve the postoperative range of movement?: A meta-analysis. J Bone Joint Surg Br. 2010;92:1429–34. doi: 10.1302/0301-620X.92B10.23199. [DOI] [PubMed] [Google Scholar]
- 19.Kelly MA. High-flexion knee designs: More hype than hope? In opposition. J Arthroplasty. 2006;21:42–3. doi: 10.1016/j.arth.2006.02.087. [DOI] [PubMed] [Google Scholar]
- 20.Lee BS, Kim JM, Lee SJ, Jung KH, Lee DH, Cha EJ, et al. High-flexion total knee arthroplasty improves flexion of stiff knees. Knee Surg Sports Traumatol Arthrosc. 2011;19:936–42. doi: 10.1007/s00167-010-1272-4. [DOI] [PubMed] [Google Scholar]
- 21.Sancheti KH, Laud NS, Bhende H, Reddy G, Pramod N, Mani JN. The INDUS knee prosthesis-prospective multicentric trial of a posteriorly stabilized high-flex design: 2 years followup. Indian J Orthop. 2009;43:367–74. doi: 10.4103/0019-5413.55976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Sancheti KH, Sancheti PK, Shyam AK, Patil S, Dhariwal Q, Joshi R. Clinical and functional outcome of INDUS knee prosthesis- A prospective single centre study. Med J Western India. 2009:35–43. [Google Scholar]
- 23.Gogia PP, Braatz JH, Rose SJ, Norton BJ. Reliability and validity of goniometric measurements at the knee. Phys Ther. 1987;67:192–5. doi: 10.1093/ptj/67.2.192. [DOI] [PubMed] [Google Scholar]
- 24.Insall J, Dorr L, Scott R, Scott W. Rationale of the Knee Society clinical rating system. Clin Orthop Relat Res. 1989;248:13–4. [PubMed] [Google Scholar]
- 25.Ritter MA, Campbell ED. Effect of range of motion on the success of a total knee arthroplasty. J Arthroplasty. 1987;2:95–7. doi: 10.1016/s0883-5403(87)80015-3. [DOI] [PubMed] [Google Scholar]
- 26.Franklin PD, Li W, Ayers DC. The Chitranjan Ranawat Award: Functional outcome after total knee replacement varies with patient attributes. Clin Orthop Relat Res. 2008;466:2597–604. doi: 10.1007/s11999-008-0428-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Anouchi YS, McShane M, Kelly F, Jr, Elting J, Stiehl J. Range of motion in total knee replacement. Clin Orthop Relat Res. 1996;331:87–92. doi: 10.1097/00003086-199610000-00012. [DOI] [PubMed] [Google Scholar]
- 28.Insall JN, Scott WN, Ranawat CS. The total condylar knee prosthesis.A report of two hundred and twenty cases. J Bone Joint Surg Am. 1979;61:173–80. [PubMed] [Google Scholar]
- 29.Long WJ, Scuderi GR. High-flexion total knee arthroplasty. J Arthroplasty. 2008;23:6–10. doi: 10.1016/j.arth.2008.06.024. [DOI] [PubMed] [Google Scholar]
- 30.Harvey IA, Barry K, Kirby SP, Johnson R, Elloy MA. Factors affecting the range of movement of total knee arthroplasty. J Bone Joint Surg Br. 1993;75:950–5. doi: 10.1302/0301-620X.75B6.8245090. [DOI] [PubMed] [Google Scholar]
- 31.Shoji H, Solomonow M, Yoshino S, D’Ambrosia R, Dabezies E. Factors affecting postoperative flexion in total knee arthroplasty. Orthopedics. 1990;13:643–9. doi: 10.3928/0147-7447-19900601-08. [DOI] [PubMed] [Google Scholar]
- 32.Ritter MA, Harty LD, Davis KE, Meding JB, Berend ME. Predicting range of motion after total knee arthroplasty.Clustering, log-linear regression, and regression tree analysis. J Bone Joint Surg Am. 2003;85-A:1278–85. doi: 10.2106/00004623-200307000-00014. [DOI] [PubMed] [Google Scholar]
- 33.Schurman DJ, Matityahu A, Goodman SB, Maloney W, Woolson S, Shi H, et al. Prediction of postoperative knee flexion in Insall-Burstein II total knee arthroplasty. Clin Orthop Relat Res. 1998;353:175–84. doi: 10.1097/00003086-199808000-00020. [DOI] [PubMed] [Google Scholar]
- 34.Farahini H, Moghtadaei M, Bagheri A, Akbarian E. Factors influencing range of motion after total knee arthroplasty. Iran Red Crescent Med J. 2012 Jul;14(7):417–21. [PMC free article] [PubMed] [Google Scholar]
- 35.Ritter MA, Stringer EA. Predictive range of motion after total knee replacement. Clin Orthop Relat Res. 1979;143:115–9. [PubMed] [Google Scholar]
- 36.Kurosaka M, Yoshiya S, Mizuno K, Yamamoto T. Maximizing flexion after total knee arthroplasty: The need and the pitfalls. J Arthroplasty. 2002;17(4 Suppl 1):59–62. doi: 10.1054/arth.2002.32688. [DOI] [PubMed] [Google Scholar]
- 37.Burnett RS, Boone JL, McCarthy KP, Rosenzweig S, Barrack RL. A prospective randomized clinical trial of patellar resurfacing and nonresurfacing in bilateral TKA. Clin Orthop Relat Res. 2007;464:65–72. doi: 10.1097/BLO.0b013e31812f783b. [DOI] [PubMed] [Google Scholar]
- 38.Wakankar HM, Nicholl JE, Koka R, D’Arcy JC. The tourniquet in total knee arthroplasty. A prospective, randomised study. J Bone Joint Surg Br. 1999;81:30–3. doi: 10.1302/0301-620x.81b1.8971. [DOI] [PubMed] [Google Scholar]
- 39.Kim YH, Sohn KS, Kim JS. Range of motion of standard and high-flexion posterior stabilized total knee prostheses.A prospective, randomized study. J Bone Joint Surg Am. 2005;87:1470–75. doi: 10.2106/JBJS.D.02707. [DOI] [PubMed] [Google Scholar]
- 40.Huang HT, Su JY, Wang GJ. The early results of high-flex total knee arthroplasty: A minimum of 2 years of follow-up. J Arthroplasty. 2005;20:674–79. doi: 10.1016/j.arth.2004.09.053. [DOI] [PubMed] [Google Scholar]
- 41.Seon JK, Song EK, Lee JY. Comparison of range of motion of high-flexion prosthesis and mobile-bearing prosthesis in total knee arthroplasty. Orthopedics. 2005;28()(10 Suppl):s1247–s1250. doi: 10.3928/0147-7447-20051002-08. [DOI] [PubMed] [Google Scholar]