

Abstract
Introduction:
The association of anemia with primary hypothyroidism has been common knowledge for many years. However; its pathogenesis is far from clear in many cases. Often the causes of anemia are manifold.
Aims and objectives:
In this study, we evaluated the causes of anemia in patients with primary hypothyroidism.
Materials and Methods:
Sixty adult nonpregnant untreated primary hypothyroid patients with anemia without any obvious cause were included. All patients were subjected to full medical history, clinical examination, biochemical and imaging studies. Serum iron profile, vitamin B12, folic acid, anti parietal cell antibody, anti TPO antibody, bone marrow study, and stool for occult blood, Coomb's test, HPLC for hemoglobinopathies and complete hemogram with reticulocyte count were done and analyzed.
Results:
Normocytic, normochromic anemia was present in 31 patients (51.6%) followed by microcytic anemia in 26 patients (43.3%). Six patients (10%) had megaloblastic anemia with vitamin B12 deficiency including 3 cases of pernicious anemia. Two patients had combined deficiency of iron and vitamin B12.
Conclusion:
Normocytic normochromic anemia with normal bone marrow was commonest type of anemia in this study, followed by iron deficiency anemia.
Keywords: Primary hypothyroidism, anemia, eastern India
INTRODUCTION
Anemia and hypothyroidism are both common diseases in the community. We need to evaluate the prevalence and types of anemia in primary hypothyroid patients because both have significant medical implications.
AIMS AND OBJECTIVE
In this study, we evaluated the causes of anemia and its causes in patients with untreated primary hypothyroidism.
MATERIALS AND METHODS
Sixty adult nonpregnant treatment naïve primary hypothyroid patients attending endocrine out patients department of N.R.S. Medical College and Hospital, Kolkata were included. They had no obvious causes of anemia. Patients with chronic diseases, infection, malignancy, hemoglobinopathies, bleeding diathesis were excluded from our study. Anemia has been defined as hemoglobin less than 13 gram/dl in male, or less than 12 gram/dl in female. Sixteen subclinical and 44 overt hypothyroidism patients as per standard definition were included. The patients first underwent complete blood count for inclusion in the study. On the basis of red cell indices (MCV) anemia has been classified as normocytic normochromic (MCV 80-100 fl), microcytic hypochromic (MCV<80 fl), and macrocytic (MCV>100 fl). For microcytic anemia, stool for occult blood, upper gastrointestinal endoscopy, iron profile study, HPLC for hemoglobinopathies were done. Serum assay of vitamin B12, folic acid, anti parietal cell antibody tests were performed for macrocytic anemia. In normocytic anemia, Coomb's test and bone marrow examination were also done. Anemia was classified as mild, moderate, and severe when hemoglobin (Hb) concentration were (10-12 gm/dl), (8-10 gm/dl) and (<8 gm/dl) respectively.
RESULTS AND ANALYSIS
The mean age of the patients was 36.5 years (19 to 67 years). Seventy percent patients were female and anti TPO antibody was positive in 58.3% cases. The prevalence of various types of anemia has been shown in Table 1 and Figure 1.
Table 1.
Prevalence of various types of anemia in patients of anemia with primary hypothyroidism

Figure 1.
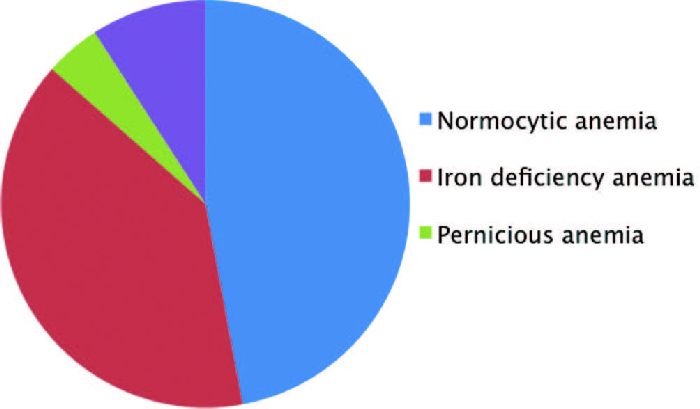
showing percent of various types of anemia with primary hypothyroidism
Among those with normocytic normochromic anemia, 1 (1.6%) had deficiency of vitamin B12 and 2 (2.8%) patients had deficiency of both iron and vitamin B12. Three (4.8 %) patients had pernicious anemia. Macrocytic anemia was present in 10 % patients. The serum levels of vitamin B12 of all these patients were low with normal serum folate. Bone marrow examination of the patients with normocytic normochromic anemia revealed normocellular marrow with varying degree of marrow iron store. Nineteen (31.6%) patients of this group had only mild anemia. In this study, 12 (20%) patients had severe anemia; among them 3 (4.8%) had normochromic normocytic anemia and 9 (14.4%) had microcytic anemia. Combined vitamin B12 and iron deficiency was found in 2 (3.2%) patients in our series. Seven (11.2%)) patients with iron deficiency anemia had menorrhagia.
DISCUSSION
Hypothyroidism is a common disease with varying frequency between countries. As decreased thyroid hormone adversely affects erythropoiesis, anemia develops in hypothyroidism. In our study, 70.65% of hypothyroid patients were female, and the most frequent cause of hypothyroidism was determined to be primary hypothyroidism arising from chronic autoimmune thyroiditis[1] consistent with the literature. According to the data of WHO, anemia prevalence is 24.8% throughout the world and it is seen more frequently in underdeveloped countries.[2] Prevalence of anemia in subclinical and overt hypothyroid groups was 26.6 % and 73.2 %, respectively. Thus, the frequency of anemia in subclinical hypothyroidism is higher than general population. Therefore, presence of hypothyroidism is a risk factor for anemia. Lack of stimulation of erythroid colony development by thyroid hormones, reduction in oxygen distribution to tissues and diminution of erythropoietin level in the absence of thyroid hormones leads to normocytic anemia, which is the most frequent type of anemia in hypothyroid patients consistent with our study similar to study by Erdogan and colleagues.[3] Prevalence of vitamin B12 deficiency increases along with the age and the prevalence was observed as 1.6% to 10% in Europe.[4] In our study, vitamin B12 deficiency was 10 % similar with these values. It mostly occurs as a result of malabsorption due to pernicious anemia accompanying hypothyroidism. Antiparietal cell antibody was present in 3 patients (4.8%) out of the 6 patients with macrocytic anemia. Folic acid deficiency is uncommon in hypothyroidism, which is corroborative with our study.
The second most common type of anemia in our series is microcytic anemia due to iron deficiency (43.2%) which is one of the most frequently seen diseases in all over the world. Larson found that 52 % (13 out of 25) of his patients of hypothyroidism had iron deficiency anemia, based on the finding of a low determination of serum iron.[5] Iron deficiency anemia largely due to menorrhagia occurring as a result of various hormonal instability and malabsorption observed in hypothyroidism.
Most common cause of anemia in hypothyroidism is normocytic normochromic and replacement of levothyroxine corrects this type of anemia. Iron deficiency is the second most cause of anemia which should be evaluated and treated properly. Therefore, anemia in hypothyroid needs to be properly evaluated because treatment will depend on the causes of anemia.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Pearce EN, Farwell AP, Braverman LE. Thyroiditis. NEngl J Med. 2003;348:2646–55. doi: 10.1056/NEJMra021194. [DOI] [PubMed] [Google Scholar]
- 2.Benoist B, McLean E, Egli I, Cogswell M. Global database on anemia. Geneva: WHO; 2008. Worldwide prevalence of anemia 1993-2005; pp. 1–2. [Google Scholar]
- 3.Erdogan M, Kosenli A, Sencer G, Kulaksizoglu M. Characteristics of anemia in subclinical and overt hypothyroid patients. Endocr J. 2012;59:213–20. doi: 10.1507/endocrj.ej11-0096. [DOI] [PubMed] [Google Scholar]
- 4.McLean E, de Benoist B, Allen LH. Review of the magnitude of folate and vitamin B12 deficiencies worldwide. Food Nutr Bull. 2008;29(2 Suppl):S38–51. doi: 10.1177/15648265080292S107. [DOI] [PubMed] [Google Scholar]
- 5.Larson SO. Anemia and iron metabolism in hypothyroidism. Acta Med Scand. 1957;157:339–63. doi: 10.1111/j.0954-6820.1957.tb14445.x. [DOI] [PubMed] [Google Scholar]