

Abstract
Hypoparathyroidism is most commonly isolated and idiopathic. Hypoparathyroidism in autoimmune polyendocrine syndrome type-2 (APS-2) is extremely rare with few isolated reports and usually presents late. We present perhaps for the first time, hypoparathyroidism being the initial manifestation of APS-2 which was diagnosed in a 32 year lady with tingling of the extremities along with hypocalcemic tetany for 15 years. She also had generalized acral and mucosal hyperpigmentation of 2 years duration. Investigations were significant for low calcium (7.1mg/dl), elevated phosphorus (4.8mg/dl), vitamin-D insufficiency (27.4ng/ml), low intact parathyroid hormone (2.3pg/ml), low basal (4.7mcg/dl) and stimulated serum cortisol (9.2mcg/dl at half hour, 11.4mcg/dl at 1 hour post synacthen), elevated triiodothyronine (2.1ng/ml) and free tetraiodothyronine (2.4ng/dl) along with suppressed TSH (<0.005 U/L). Imaging relevaled mild cerebellar calcification, normal adrenals with diffuse uptake of Tc99- pertechnate. A diagnosis of hypoparathyroidism with Addison's and Graves’ disease as a part of APS-2 was made. This report intends to highlight the clinical heterogeneity and varied presentation of APS-2. Routine screening of other hormonal function (especially adrenal function, thyroid function and blood glucose) in a patient with diagnosed hypoparathyroidism is advisable to decrease the chances of missing APS-2.
Keywords: Tetany, APS2, hypoparathyroidism
INTRODUCTION
Autoimmmune polyendocrine syndrome type-2 (APS-2) though being the most common polyendocrine disorder, is rare disease with a prevalence of 4-5/100,000, predominantly occurring in females (3:1) with a peak onset in the fourth decade[1]. Hypoparathyroidism is most commonly isolated and idiopathic. Hypoparathyroidism as a part of polyglanduar syndrome is most commonly associated with autoimmune polyendocrinopathy candidiasis and ectodermal dystrophy (APECED) better known as APS-1, observed mostly in children[2]. Hypoparathyroidism is extremely rare in APS-2 with few isolated reports. Hypoparathyroidism as the presenting feature of APS-2 has not been reported to the best of our knowledge.
CASE REPORT
SD, 32 year lady presented with tingling and numbness of bilateral hands and feet progressively worsening for the last 15 years with history of spontaneously resolving episodic twisting of hands, suggestive of tetany. There was no history of seizures, gait instability or falls. She also complained of progressive generalized hyperpigmentation, along with hyperpigmentation of palmer creases of hand and feet for the last 2 years [Figure 1]. There was no history of nausea, vomiting, presyncope, syncope or loss of consciousness. She complained of occasional palpitation. Menstrual cycles were regular and she had 2 children, younger child 12 years of age. Examination was significant for oral mucosal hyperpigmentation, pigmentation of hands and feet, more prominent on the palmer creases, grade-1b goitre, fine tremors, tachycardia, and significant postural drop of blood pressure [Figure 1]. Chvostek sign was absent. Trousseau's sign was positive within 30 seconds of inflation of blood pressure cuff. Investigations were significant for low serum calcium, elevated phosphorus, vitamin-D insufficiency, low intact parathyroid hormone (iPTH), low basal as well as stimulated cortisol, high adrenocorticotropic hormone (ACTH), elevated tri-iodithyronine (T3) and free tetra-iodothyronine (fT4) along with suppressed TSH. Anti-thyroid peroxidise antibody was positive. Serum IgA level was normal and IgA anto-tissue transglutaminase (TTG) antibody was negative. The investigations have been elaborated in Table 1. Thyroid scan using technitium99-pertechnate revealed diffuse increased uptake in the thyroid suggestive of Graves’ disease. Computerized tomography (CT) brain revealed mild cerebellar calcification with normal basal ganglia and cortex [Figure 2]. CT abdomen revealed normally visualized adrenals without any calcification [Figure 3]. A diagnosis of hypoparathyroidism with Addison's and Graves’ disease (autoimmune polyendocrine syndrome type-2) was made.
Figure 1.

(a) Facial profile of the patient showing grade-Ib goitre, (b) Hyperpigmentation of hands and feet, especially involving the plamar creases
Table 1.
Biochemical parameters
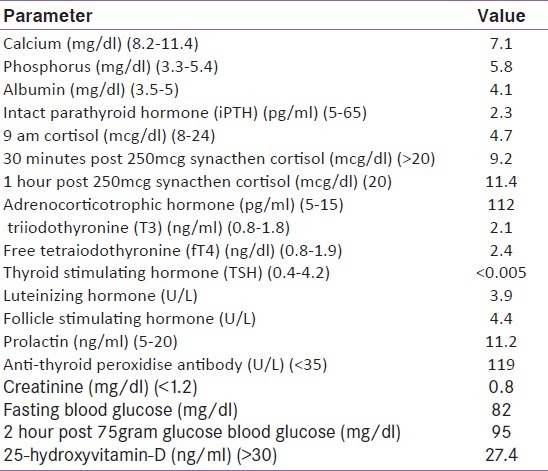
Figure 2.
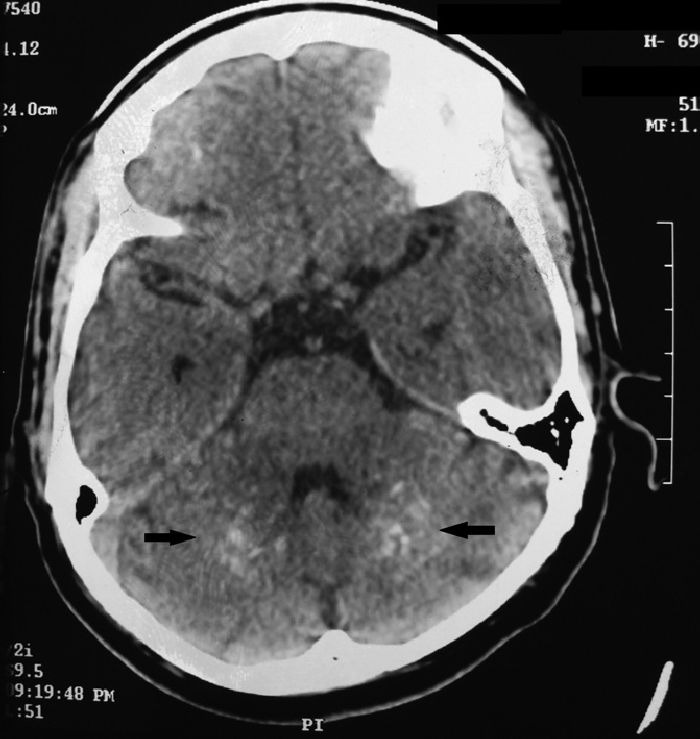
Computerized tomography brain showing mild bilateral cerebellar calcifications (black arrows)
Figure 3.
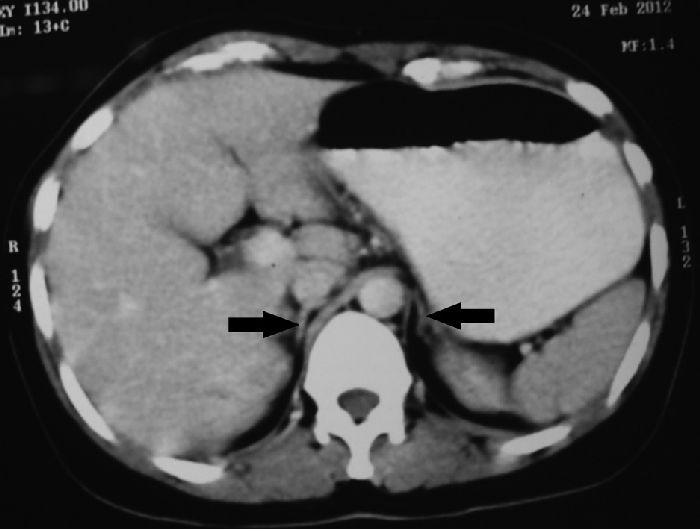
Computerized tomography (CT) of abdomen showing bilateral normal adrenals (black arrows)
Hydrocortisone was started at 25mg per day in divided doses. Tetany along with tingling improved with calcium and calcitriol supplementation. Tremors and palpitations improved with received carbimazole at 30 mg/day and propranolol 40mg/day.
DISCUSSION
APS-2 is defined as occurance of adrenal insufficiency (100%) either with autoimmune thyroid disease (70-90%) (Schimidt syndrome) or with type-1 diabetes (20-50%) (Carpenter syndrome) (1). Adrenal failure is the first endocrine abnormality in around 50% of the patients, autoimmune thyroid disease in around 30% and type-1 diabetes in the remaining 20%. Primary hypogonadism is next most common feature of APS-2 seen in up to 10% women. Other minor manifestations include pernicious anemia (1-25%), vitiligo (4-12%), alopecia (2-5%), autoimmune hepatitis (4%), Celiac disease (2%) and lymphocytic hypophysitis. Hypoparathyroidism in APS-2 is exceedingly rare, and when seen, is usually late onset (1). It has been suggested that hypocalcemia in any patient of APS-2 should lead to investigations to rule out Celiac disease causing malabsorption leading to vitamin-D deficiency, hypocalcemia and secondary hyperparathyroidism (1). Absence of features of chronic diarrhea or malabsorption, along with absence of anti-TTG antibody ruled out Celiac disease. Presence of vitamin-D insufficiency, elevated phosphorus in the background of normal renal function, with low iPTH level confirmed hypoparathyroidism as the cause for hypocalcemia and tetany in our patient.
Anti-TPO antibody was the only studied autoimmune marker in our patient and its presence supported the autoimmune aetiology of the thyroid disease as well as the presence of underlying autoimmunity. One of the limitations of this case report is the lack of estimation of adrenal auto-antibodies (anti-21-hydroxylase antibody, anti-17-hydroxylase antibody). Anti calcium sensing receptor (CaSR) antibody and anti parathyroid antibody testing is not available in this part of the country. It must however be remembered that presence of anti-CaSR antibody is relatively low in patients with hypoparathyroidism (25-49%)[3]. It has been suggested that patients with hypoparathyroidism less than 5 years duration are more likely to have ant-CaSR antibody positivity (72%) as compared to those more than 5 years (14%)[4].
Other minor and rare manifestations of APS-2 include myasthenia, ulcerative colitis, primary biliary cirrhosis, granuloma annulare, dermatitis herpetiformis, stiff man syndrome, thrombocytopenic purpura and heart blocks.
This report intends to highlight the clinical heterogeneity and varied presentation of APS-2. This is perhaps the first report of a patient with APS-2 having hypoparathyroidism as the initial manifestation of the disease. Routine screening of other hormonal function (especially adrenal function, thyroid function and blood glucose) in a patient with diagnosed hypoparathyroidism is advisable to decrease the chances of missing APS-2.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Owen CJ, Cheetham TD. Diagnosis and management of polyendocrinopathy syndromes. Endocrinol Metab Clin North Am. 2009 Jun;38(2):419–36. doi: 10.1016/j.ecl.2009.01.007. [DOI] [PubMed] [Google Scholar]
- 2.Brown EM. Anti-parathyroid and anti calcium sensing receptor antibodies in autoimmune nonehypoparathyroidism. Endocrinol Metab Clin North Am. 2009 Jun;38(2):437–45. doi: 10.1016/j.ecl.2009.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Goswami R, Brown EM, Kochupillai N, et al. Prevalance of calcium sensing receptor autoantibodies in patients with sporadic idiopathic hypoparathyroidism. Eur J Endocrinol. 2004;89:557–62. doi: 10.1530/eje.0.1500009. [DOI] [PubMed] [Google Scholar]
- 4.Li Y, Song YH, Rais N, et al. Autoantibodies to the extracellular domain of calcium sensing receptor in patients with acquired hypoparathyroidism. J Clin Invest. 1996;97:910–4. doi: 10.1172/JCI118513. [DOI] [PMC free article] [PubMed] [Google Scholar]