

Abstract
This research investigates the relationship between per capita tobacco control expenditures, cigarette consumption, and healthcare expenditures in the state of Arizona. Arizona’s tobacco control program, which was established in 1994, concentrates on youth uptake of smoking and avoids public policy and commentary on the tobacco industry. We use a cointegrating time series analysis using aggregate data on healthcare and tobacco control expenditures, cigarette consumption and prices and other data. We find there is a strong association between per capita healthcare expenditure and per capita cigarette consumption. In the long run, a marginal increase in annual cigarette consumption of one pack per capita increases per capita healthcare expenditure by $19.5 (SE $5.45) in Arizona. A cumulative increase of $1.00 in the difference between control state and Arizona per capita tobacco control expenditures increases the difference in cigarette consumption by 0.190 (SE 0.0780) packs per capita. In 2004, the cumulative reduction between 1996 to 2004 in pre-tax cigarette sales revenue due to Arizona’s tobacco control expenditures was $500 million (95% CI: $99.0 million, $896 million). The cumulative healthcare savings was $2.33 billion (95% CI $0.374 billion, $5.00 billion) and the cumulative reduction in cigarette consumption was 200 million packs (95% CI 39.0 million packs, 364 million packs). Arizona’s tobacco control expenditures are associated with reduced cigarette consumption and healthcare expenditures, amounting to about 10 times the cost of the program through 2004. This return on investment, while large, was less than the more aggressive California program, which did not limit its focus to youth and included tobacco industry denomalization messages.
Keywords: Medical Economics, Tobacco Control, Tobacco Use (Smoking), Environmental and Public Health, Health Education, Healthcare Costs, USA
INTRODUCTION
Large-scale tobacco control programs reduce cigarette consumption (Institute of Medicine 2007) and tobacco-induced heart disease (Fichtenberg and Glantz 2000) and cancer (Centers for Disease Control and Prevention 2007a; Jemal, Cokkinides et al. 2003; Barnoya and Glantz 2004). Rapidly increasing healthcare expenditures are a major problem in the United States and around the world. The California Tobacco Control Program was created in 1988 by voter initiative and implemented beginning in 1989 (Glantz and Balbach 2000) and has been associated with significant reductions in smoking and direct healthcare expenditures, which, over the first 15 years of the program, totaled approximately 50 times what the program cost (Lightwood, Dinno et al. 2008). Arizona voters established its tobacco control program in 1994, with implementation beginning in 1996 (Aguinaga Bialous and Glantz 1999; Hendlin, Barnes et al. 2008). There are substantial differences between the two programs. The California program focuses on adults, reinforces the nonsmoking norm, emphasizes policy change, and uses media focused on secondhand smoke and the manipulative behavior of the tobacco industry (Tobacco Control Section 1998). The Arizona program concentrates on youth uptake of smoking and avoids public policy and commentary on the tobacco industry. This paper applies and extends our earlier California model (Lightwood, Dinno et al. 2008) to Arizona to estimate the associations between per capita state tobacco control expenditures, cigarette consumption and healthcare expenditures in Arizona and compares the results to California.
METHODS
Model
Classical time series regression techniques are not be appropriate for analysis of the relationship between aggregate tobacco control expenditures and healthcare costs because these classical techniques require that the underlying parameters describing the underlying processes remain constant over time (ie, the processes are “stationary”). The underlying processes that determine state expenditures on tobacco control programs, smoking behavior, and healthcare costs change with time as does the tobacco industry’s promotional efforts, medical technology, costs and the population (i.e., are “nonstationary”). In recent years economists have developed an approach called cointegrating regressions that, if specified mathematical conditions are met, provide consistent and reliable estimates of the relationships between two or more nonstationary processes (Engle and Granger 1987; Maddala and Kim 1998; Greene 2000; Enders 2004; Burke and Hunter 2005). The claim that these processes are nonstationary comes from strong evidence that the data evolve over time in a way similar to random walks.
The cointegrating regression describes the long run equilibrium statistical relationship between the variables. The stationary residuals describe departures of the observations from the long run equilibrium relationship (Engle and Granger 1987; Maddala and Kim 1998; Greene 2000; Enders 2004; Burke and Hunter 2005). A well-specified and identified structural model is required for economic interpretation when a cointegrating regression involves more than two variables (Hsiao 2001; Hsiao 2006).
Each cointegrating regression must be accompanied by an error, or equilibrium, correction model (ECM) that describes the dynamic short-run relationship between the variables. An ECM describes the behavior of the first difference of the dependent variables in the cointegrating regression as a function of the lagged cointegrating regression residual and lagged first differences of the variables in the cointegrating regression. An ECM corresponding to a cointegrating regression exists if the coefficient of the lagged cointegrating regression residual (the “error correction term”) exists. The error correction term measures the rate at which the cointegrating relationship moves toward long run equilibrium (Engle and Granger 1987; Maddala and Kim 1998; Greene 2000; Enders 2004; Burke and Hunter 2005).
We developed a system of two cointegrating regressions that describe the relationship between tobacco control program expenditures and healthcare costs that meet these mathematical conditions:
The first cointegrating regression equation describes annual per capita healthcare expenditures in Arizona modeled as a function of corresponding heath care expenditures in 38 control states that did not have substantial tobacco control programs and the difference in annual per capita cigarette consumption between Arizona and the control states, controlled for per capita personal income and population age structure. This specification controlled for common national trends in per capita healthcare expenditures and smoking over time (e.g., trends in medical practice, insurance status, access to care, medical cost inflation, and demographic changes).
The second cointegrating regression equation describes the difference between Arizona and control states’ per capita cigarette consumption modeled as a function of the difference in cumulative per capita California and control states’ tobacco control expenditures and cigarette prices.
Thus, as in our California (Lightwood, Dinno et al. 2008) study, two equation systems were estimated for the main results: 1) a cointegrating and ECM regression for real per capita healthcare expenditures as a function of the level of cigarette smoking and other variables, and 2) a regression for per capita cigarette consumption as a function of cumulative state tobacco control education expenditures and other variables. Both the Arizona and California analyses use the same 38 control states that did not have substantial tobacco control programs or tobacco tax increases of 50 cents per pack or more over the sample period (Alabama, Arkansas, Colorado, Connecticut, Delaware, Georgia, Idaho, Illinois, Indiana, Iowa, Kansas, Kentucky, Louisiana, Maine, Minnesota, Mississippi, Missouri, Montana, Nebraska, Nevada, New Hampshire, New Mexico, North Carolina, North Dakota, Ohio, Oklahoma, Pennsylvania, Rhode Island, South Carolina, South Dakota, Tennessee, Texas, Utah, Vermont, Virginia, West Virginia, Wisconsin and Wyoming) (Abadie, Diamond et al. 2007).
The model used for Arizona has the same structure as for California, with the addition of the proportion of the population that was elderly (≥ 65 years old) and per capita personal income. (These two variables were explored in our sensitivity analysis of the California model, but were not statistically significant in that model and their presence or absence did not affect the results (Lightwood, Dinno et al. 2008).) Annual per capita all-payer total healthcare expenditures in Arizona is modeled as a function of corresponding healthcare expenditures in the control states and the difference in annual per capita cigarette consumption between Arizona and the control states:
| (1) |
where
hi,t = per capita real total all payer direct healthcare expenditures in i (Arizona = AZ; control states = c) in year t in 2004 dollars,
si,t = per capita cigarette consumption in i, in year t,
Ai,t = proportion of elderly (age ≥ 65) in the population i, in year t,
yi,t = real per capita income in i in year t in 2004 dollars,
t = year (t0 =1975),
ν1,t = stationary regression residuals, in year t.
Per capita healthcare expenditure in the control states controls for common time trends in healthcare expenditures in both populations, such as technological progress, changes in standards of and access to care, and insurance coverage. The additional explanatory variables model determinants of healthcare expenditures that do not follow a common time trend in the two populations: the difference in per capita cigarette consumption, (sc,t − sAZ,t), difference in real per capita income, (yc,t − yAZ,t), and difference in proportion of the population that is elderly, (Ac,t − AAZ,t), between the control states and Arizona. These variables are expressed as differences, but this specification is not necessary for structural interpretation of the coefficients and the use of differences between control and intervention populations as explanatory variables should be considered restrictions that indicate the control state and Arizona variables have the approximately the same effect on healthcare costs. The coefficient of interest is α2, which measures the effect of differences in the level of per capita cigarette consumption between Arizona and control states on the difference in per capita healthcare expenditures.
The cointegrating regression for the difference between per capita cigarette consumption (demand) in Arizona and the 38 control states is:
| (2) |
where
Ei,t = per capita real cumulative tobacco control education expenditures in i (Arizona = AZ or control states = c) in year t in 2004 dollars,
pi,t = real price of cigarette per pack in i, in year t in 2004 dollars,
ν2,t = a stationary regression residuals, in year t.
The difference between per capita cigarette consumption in Arizona and the 38 control states, (sc,t − sAZ,t), is a function of the differences in cumulative per capita tobacco control expenditures, (EAZ,t − Ec,t), cigarette prices, (pc,t − pAZ,t), and per capita income in Arizona, yAZ,t, and a linear time trend (t−t0). The prevalence and intensity of smoking in Arizona and the control state change over time in a way that allows use of per capita cigarette consumption as a single index of two aspects of smoking behavior: prevalence of current smoking and consumption per current smoker (Giovino 2009). As in the California study (Lightwood, Dinno et al. 2008), cumulative expenditures were used because some types of expenditures in any given year (e.g., training, community mobilization to effect policy change) are unlikely to change cigarette consumption immediately but will affect it over a longer period and expenditures for specific programs and services (e.g., media interventions, quit lines) may affect consumption several years later because successful cessation is a process that usually takes many years and multiple quit attempts, and cohorts of youth with decreased initiation rates enter the population gradually (Farrelly, Pechacek et al. 2001).
Equation (2) has the same form as for California (Lightwood, Dinno et al. 2008), except that the effect of price (pc,t − pAZ,t) is in the equation as the price difference between Arizona and the control states because in a preliminary analysis the coefficients for price in Arizona and the control states were of similar absolute value and opposite sign. (In California there was a significant difference in the magnitude of the price effect in California and the control states (Lightwood, Dinno et al. 2008).)
The ECM for the healthcare expenditure equation (1) is:
| (3) |
and the ECM for the cigarette consumption (demand) equation (2) is:
| (4) |
where Δ is the first difference operator (Δx = xt − xt−1) and ε1,t, ε2,t are stationary normally distributed residuals. Equations (3) and (4) are the ECM equations that model the short run dynamics of the dependent variables in the cointegrating regressions as a function of the lagged cointegrating regression residuals ν1.t and ν2.t (measuring departures from the long run cointegrating relationship) and statistically significant lagged differences of the variables in the respective cointegrating regressions.
The system defined by equations (1)-(4) is identified, which means that the coefficients have a structural interpretation (Hsiao 2001; Hsiao 2006). The details of identification, tests for unit roots in the data and residuals of the cointegrating regressions, estimating the parameters in equations (1) and (2) and conducting model reliability and sensitivity analysis are similar to our earlier California study (Lightwood, Dinno et al. 2008) and are presented in the Supplemental Text. The model was estimated using irrelevant instrumental variables regression (Phillips 2006).
Data Sources
As in the California study (Lightwood, Dinno et al. 2008), annual per capita personal healthcare expenditures (the sum of hospital care, physician services, other professional services, dental services, home health and long term care, durable and non-durable goods, drugs and other personal healthcare expenditures) were obtained from the Center for Medicare and Medicaid Services. Data were for calendar years 1976 to 2004 (Department of Health and Human Services 2007). (The data for the California study (Lightwood, Dinno et al. 2008) started in 1980; the additional data for Arizona reduce the influence of an apparent outlier in Arizona cigarette consumption in 1981.)
State per capita personal income data were obtained from the Bureau of Economic Analysis (Bureau of Economic Analysis 2007) and age-specific resident state population was obtained from the Census Bureau (United States Census Bureau 2004a; United States Census Bureau 2004b; United States Census Bureau 2008). Price indices were constructed for each census region using the same method as for the California study (Lightwood, Dinno et al. 2008) using the All-Item (for cigarette prices and state per capita income) and Medical Care Price Indices (for healthcare expenditure) for all urban consumers, respectively (Bureau of Labor Statistics 2007; California State Department of Finance 2007). Cigarette consumption, price and tax data were from Tax Burden on Tobacco (Orzechowski & Walker 2005) as compiled by the CDC State System (Centers for Disease Control and Prevention 2007b). Arizona tobacco control educational expenditures were from state budget records (Bialous and Glantz 1997; Hendlin, Barnes et al. 2008).
Details of construction of the instruments and variables, and the data, appear in the Supplemental Text.
Model Reliability and Sensitivity Analysis
The state healthcare expenditures used for these estimates include all services provided within the state rather than to state residents (i.e., “all payer” data) in the main analysis. The consistency of all-payer and resident data available for the years 1991 to 2004 were measured using correlation analysis.
Alternative estimators (ordinary least squares and fully modified irrelevant instrumental variables (Phillips 2006)) for the cointegrating regression equations (1) and (2) were compared to instrumental variables estimates to check for robustness.
The analysis was repeated using alternative measures of healthcare expenditure that included only higher quality data (called the “subtotal” data) which omitted some components that are based on lower quality survey and health system census data. The cointegrating regression for per capita direct healthcare expenditure, equation (1), was also estimated using the subtotal state resident healthcare expenditure data using the years for which data are available (1991 to 2004). The stability of the results for the cointegrating regressions, equations (1) and (2), were checked using recursive regressions over 1976 to 2004.
The possibility of omitted variable bias was checked by estimating alternative specifications of the cointegrating regressions that included other possible explanatory variables. The variables checked for healthcare expenditure regression, equation (1), were density of community hospital beds and physicians, proportion of population that is White or Hispanic, proportion of the population receiving Medicaid benefits, and prevalence of overweight and obesity. The variables checked for the per capita cigarette consumption, equation (2), were proportions of the population that were elderly, White, and Hispanic.
The potential effect of untaxed consumption from cross border sales was checked using a time series of prices, and we tested the exogoneity of the difference between Arizona and control state tobacco control educational expenditures.
The cointegrating regression for healthcare expenditure, equation (1), was estimated using all states other than Arizona, and control states in the Northeast, Midwest, South and West Census Regions, in order to check robustness of the estimates to the choice of the control states.
Calculations were done using Stata Version 9.
Deterministic dynamic simulations of the median values of the dependent variables were used to predict the observed dependent variables for the regression system, equations (1)-(4), to determine how well the model could reproduce the observed data. Each cointegrating equation and ECM system was solved recursively to generate predictions of the dependent variable as a function of the regression coefficients and the exogenous variables, using the first three observations for initialization. The dependent variables were recursively generated using the previous predicted values. The simulation began in 1997, using 1995 and 1996, for initialization of the ECM regressions, equations (3) and (4).
Healthcare expenditure savings in Arizona
A Monte Carlo simulation was used to calculate the distribution of the differences of several outcome variables attributable to the historical Arizona tobacco control expenditures on state cigarette consumption and healthcare costs. The distribution of the changes in 2004 of the annual per capita healthcare expenditure and per capita cigarette consumption were estimated as well as the cumulative total Arizona state cigarette consumption and healthcare costs from 1996 to 2004. As with our analysis of California (Lightwood, Dinno et al. 2008), the estimates were calculated using the formulas for the deterministic dynamic simulation with historic Arizona state tobacco control education expenditures compared to an alternative history with no expenditures, assuming that the time path of all other variables remained constant. The uncertainty in the estimates was modeled using the standard error of the cigarette consumption (s*, t) and tobacco control education expenditure (E*, t) coefficients, and the distribution of the cointegrating regression and ECM regression errors (υ*, t, and ε*, t). The Monte Carlo estimate used 20,000 trials with Crystal Ball Version 11 (Oracle Corporation 2000).
RESULTS
Cointegrating regressions (long run relationships) and ECMs
The data are integrated of order one, except for the proportion of the population that is elderly (A*, t), which may be integrated of order two. Regressions with mixed variables integrated of order one and two may be cointegrating, so equation (1) is an acceptable specification (Haldrup 1997). Equations (1) and (2) are cointegrating regressions with stationary residuals. The explanatory value of the regressions is high (using R2 as a measure of fit) and all coefficients are highly significant, as expected for cointegrating regressions (Table 1).
Table 1.
Estimated personal healthcare expenditure, per capita cigarette consumption and tobacco control education expenditures
| Regression | R2 (%) | RMSE | Autocorrelation | ||
|---|---|---|---|---|---|
| eq. | Healthcare Expenditure | ||||
| Cointegrating Regression (Long-Run Relationship) | |||||
| 1 |
|
82 | 116 | 0.520* | |
| Equilibrium correction model | |||||
| 3 |
|
42 | 80 | -0.0371 | |
| Difference in Cigarette Consumption | |||||
| Cointegrating Regression (Long-Run Relationship), equation | |||||
| 2 |
|
89 | 2.98 | 0.159 | |
| Equilibrium correction model | |||||
| 4 |
|
54 | 2.48 | -0.070 | |
Significant first order autocorrelation at the 0.05 level.
Note: dollars in year 2004 dollars.
The estimated coefficient for the effect of per capita cigarette consumption on per capita healthcare expenditures in Arizona (α2 in equation (1)) is -$19.5 (SE 5.45) /pack per capita. The coefficients for per capita income and proportion of the population that is elderly are significant and have the expected signs: the coefficients imply per capita healthcare expenditure increase with per capita income and elderly population in both the Arizona and control populations.
The estimated coefficient for the effect of cumulative per capita tobacco control educational expenditure on the difference in per capita cigarette consumption in Arizona (β1 in equation (2)) is 0.190 (SE 0.0780) packs per capita / $ per capita. The price and income coefficients are -16.2 (SE 3.98) packs per capita / $ per pack, and -0.00281 (SE 0.000751) packs per capita / $ per capita, respectively. The time coefficient is 1.07 (SE 0.194) packs per capita / year, indicating that the secular trends in per capita cigarette consumption in Arizona and control populations are growing apart, other factors held constant.
The ECM models have reasonable explanatory power and well behaved, normally distributed residuals without autocorrelation. Outliers exist in the residuals for the ECMs for both cointegrating equations, but they are not influential. The error correction terms in the final version of the ECM models are -0.471 (SE 0.152) and -0.955 (SE 0.182) for healthcare expenditure and cigarette consumption, respectively, and are statistically significant.
There is an unusually large change in the difference between control and Arizona cigarette consumption, (sc,t − sAZ,t), in 1981, but this observation is not influential in any of the estimates for equations (1)-(4).
Estimated savings due to per capita cigarette consumption
This analysis indicates that Arizona’s tobacco control program was associated with a reduction of 46.4 million packs (95% CI: 9.0 million packs, 84.2 million packs) of cigarettes being smoked in 2004, and a cumulative reduction in cigarette consumption due to the tobacco control program between 1996 and 2004 of 200 million packs (95% CI: 39.0 million packs, 364 million packs) worth $500 million (95% CI: $99.0 million, $896 million) in pretax revenue to the tobacco industry. In 2004, healthcare costs were $724 million (95% CI $116 million, $1556 million), or 3%, below what was projected in the absence of the tobacco control program. The cumulative effect of the program (in year 2004 dollars) was a saving of $2.33 billion (95% CI $0.374 billion, $5.00 billion) in healthcare costs (Figures 2 and 3). The total cost of the Arizona tobacco control education program in 2004 dollars was $235 million between 1996 and 2004. The ratio of total direct healthcare cost savings to the cost of the tobacco control program was 10 (95% CI: 2, 21).
Figure 2.
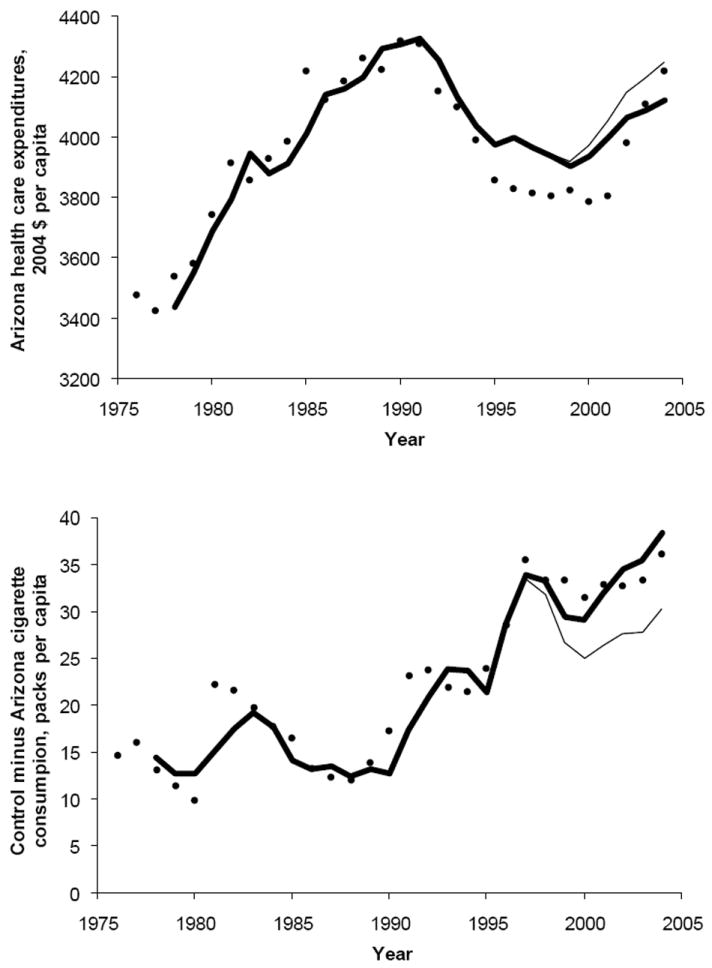
Arizona per capita healthcare expenditures were lower than predicted (top panel) and the differences between control state and Arizona per capita cigarette consumption larger than predicted (bottom panel) without the Arizona tobacco control program (light lines). (top): Arizona hAZ,t, from equations (1) and (3) using predicted difference in control state and Arizona cigarette consumption from equations (2) and (4). (bottom) Difference in control state and Arizona cigarette consumption, (sc,t−sAZ,t) from equations (2) and (4). Symbols: observed values (black circles), predicted values from dynamic predictions using the cointegrating and ECM equations (thick solid line), predicted values without the Arizona tobacco control educational expenditures set to zero (thin black line).
Figure 3.
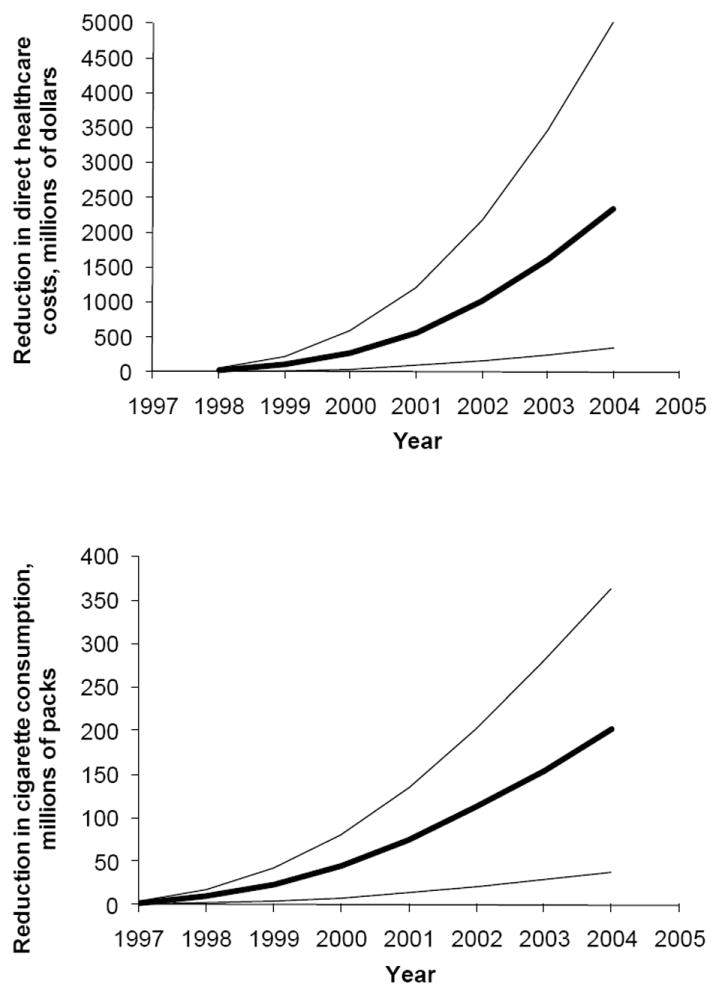
Predicted annual reductions in direct healthcare expenditure in Arizona (top) and difference cigarette consumption between Arizona and control states (bottom) attributable to the Arizona tobacco control program. Light lines show 95% confidence intervals.
Model Reliability and Sensitivity Analysis
All correlations between all-payer and resident healthcare expenditures exceed 0.90 (levels) and 0.85 (first differences) for the years of available data (1991 to 2004), indicating that the all-payer costs are a reasonable estimate of actual healthcare expenditures.
The cointegrating regressions are robust to estimation with ordinary least squares and fully modified irrelevant instrumental variables estimators.
Use of subtotal per capita healthcare expenditures as the dependent explanatory variable for the years 1980 to 2004, and with the restriction (sc,t − sAZ,t) produce similar results to that in the main analysis (Table 1): the estimated effect of per capita cigarette consumption on per capita healthcare costs is -$17.2 (SE 4.31) / pack per capita. However, if the restriction that sc,t = −sAZ,t is not imposed, the coefficient for sc,t is insignificant. All other conclusions of the main analysis hold with the subtotal direct healthcare expenditure data for 1980 to 2004. The estimates of the cointegrating regressions, equations (1) and (2), produced similar results as the main analysis for the subtotal residential data for 1991 to 2004 despite the small sample size (14 years of annual data). These results strongly indicate the use of state all-payer data rather than the residential data for the main analysis does not distort the estimates.
The recursive regressions for healthcare expenditure, equation (1), showed convergence to their final values between 1994 and 1997 and were stable over the last seven years of the sample.
The explanatory variables per capita cigarette consumption, s *,t, and income, y *,t, smoking, proportion elderly, A *,t in equation (1) are expressed as differences between Arizona (the intervention) and the 38 control states. This restriction assumes that the marginal effects of these variables on healthcare costs are equal, on average, in Arizona and the control states. We used an F-test to test the joint hypothesis that the three restrictions held (for s *,t, and income, y *,t, smoking, proportion elderly, A *,t for intervention and control), and the three assumptions were not rejected (P = 0.510). The same comments on the expression of explanatory variables as differences between the intervention and control population apply for equation (2) and the same procedures were used to confirm that the assumptions were consistent with the data.
No other explanatory variables were found to enter the cointegrating regressions, equations (1) and (2), and no evidence was found that untaxed cross-border cigarette sales affected the results. Per capita tobacco control expenditures are weakly exogenous and constant for the period of the Arizona control program. This finding is consistent with other analyses of state tobacco-control expenditure (Gross, Soffer et al. 2002; Marlow 2008).
The specifications for the cointegrating regressions are based on 29 annual observations. Although non-stationarity of the variables and cointegrating regressions methodology provides clearer guidance for specification than in the stationary case, the results may be influenced by finite sample effects. The results of out-of-sample forecasts as new data become available will be important for validation of these results.
The results for the cointegrating regression for healthcare, equation (1) do not change significantly using the rest of the U.S. or census regions as controls.
The dynamic simulations show good performance in tracking the observed values for healthcare costs and are similar to the full sample cointegrating regression fits. The regressions of predicted on observed values have R2 statistics comparable to the cointegrating regressions, and significant correlations; the slope coefficients do not differ significantly from 1.0 (P for t-test for cigarette consumption equation: 0.31, P for t-test for health expenditure equation: 0.32).
See the Supplemental Text for details of these sensitivity analyses.
DISCUSSION
These estimates for Arizona confirm earlier work for California (Lightwood, Dinno et al. 2008) that large scale tobacco control programs are associated with substantial reductions in smoking and healthcare costs, despite the fact that implementation of the two programs has been quite different. Using a different state, the parameter estimates are very similar in the two analyses. The cointegrating regression coefficients for the effect of per capita cigarette consumption on per capita healthcare expenditure are similar for the two system: -$19.5 (SE 5.45) /pack per capita for Arizona vs. -$27.0 (SE 1.82) /pack per capita for California (P = 0.26). The effect of tobacco control expenditures on and difference in per capita cigarette consumption, 0.190 (SE 0.0780) packs per capita/$ per capita for Arizona vs. 0.261 (SE 0.0780) packs per capita/$ per capita for California (P = 0.096) suggest that the magnitude of the effect of the Arizona program may be smaller than the California program.
Using the same method as for California (Lightwood, Dinno et al. 2008), the implied direct healthcare cost per smoker in Arizona is between $2068 and $2324, compared to $3940 to $4800 for California. The difference in these estimates may be due to differences the cost structure between California and Arizona (e.g., home health care is used more intensively used in Arizona than California), different patterns of utilization in current vs. nonsmokers between the two states, different age structures or intensity of smoking not captured in the measure used for smoking behavior (per capita consumption), different exposure to passive smoking, or some combination of all those factors. These estimates are not designed to produce cost estimates directly comparable to the cross-sectional estimates produced by the CDC SAMMEC system, however, they are roughly consistent with the CDC estimates, as are the California results (Lightwood, Dinno et al. 2008).
The long-run price elasticity of cigarette demand in Arizona is in normal range of other estimates (Gallet 2004) and are similar to those for the California estimates (Lightwood, Dinno et al. 2008): they range from 0.190 (SE 0.0467), at the beginning of the available data in the 1970s, to 0.606 (SE 0.149) in the late 1990s, and increase towards unity after cigarette prices increased dramatically in 1999. This increase in the price elasticity of demand is to some extent determined by linear specification of the cigarette consumption equation (the cigarette demand relationship, (equation (2)) that forces the elasticity to rise as the quantity of cigarettes consumed falls. To the extent that they are comparable with constant elasticity models, these elasticity estimates are consistent with existing long-run estimates (Gallet 2004) until the recent large price increase of 1999. The authors are not aware of any estimates of the cigarette price elasticity of demand that isolate the effect of the price increases that occurred starting in 1999.
The research reported here has limitations similar to that for California (Lightwood, Dinno et al. 2008): the regression estimates use observational data and the ability to determine the specification of the cointegrating regression specifications and the short run dynamics estimated with ECM model are uncertain due to small sample size.
The ratio of healthcare cost savings to program cost as of 2004, after the Arizona program had been in place for nine years, was 10 to 1 is smaller than in California ratio of 50 to 1 (Lightwood, Dinno et al. 2008) which as of 2004 had been in place for 15 years, but is still large. As of 1998, when the California program had been in place for nine years, the same number of years as Arizona in 2004, the ratio of cumulative program cost to savings was 25 to 1. The difference in the mean estimated saving is due to the smaller coefficients describing the effect of the Arizona program expenditures and the differing time paths of historical funding of the two programs. While both states’ tobacco control programs yielded many times their costs in healthcare savings, the more aggressive California program may be associated with a greater return on investment.
Because the Arizona program has focused on youth prevention which, even if successful, would not affect health costs for many years, it is possible that over a longer time horizon the relative cost effectiveness (in terms of health costs) between it and the California program could be different than we found. This situation is unlikely, however, because, while the California program did not focus on youth, it led to substantial drops in youth initiation (Messer and Pierce, 2010).
The results for Arizona in this paper and previous results for California have important implications for tobacco control policy worldwide. The World Health Organization Framework Convention on Tobacco Control, the first public health treaty negotiated under the auspices of the WHO, had been ratified by 171 countries as of October 2010 (World Health Organization, 2010). Article 12 of the Framework requires parties to develop and implement “education, communication, training and public awareness programs” with the same elements as the large scale tobacco programs that have been implemented in the United States discussed in this paper. As of October 2010, the implementing protocol for Article 12 was still being developed. The results of this research provide evidence that such programs will be effective in reducing cigarette consumption, which will in turn reduce per capita healthcare costs.
Supplementary Material
Figure 1.
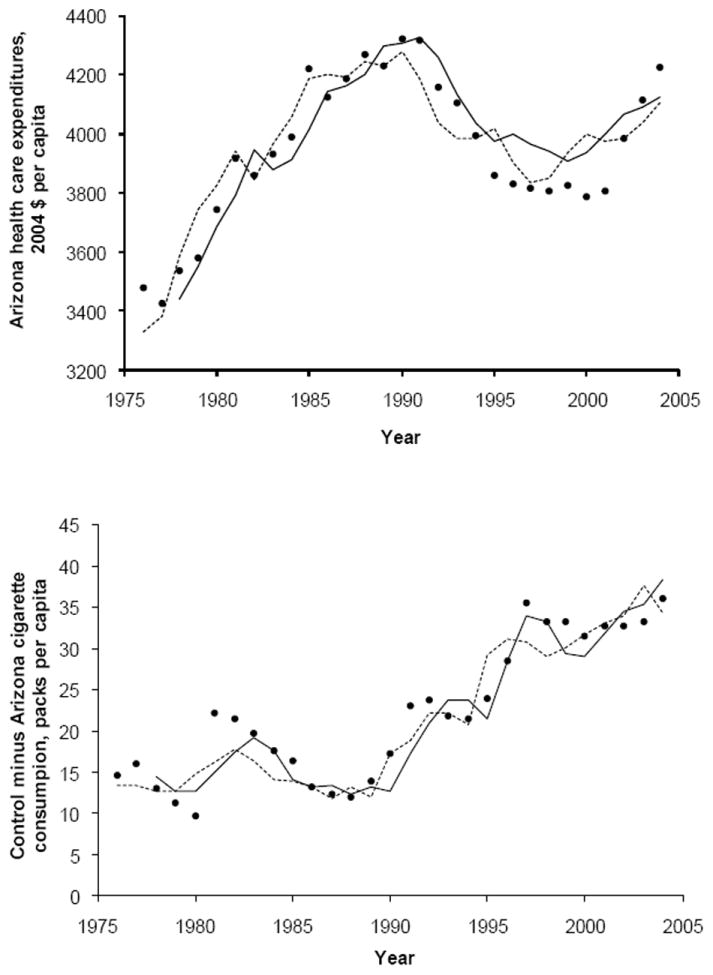
Dynamic predictions of per capita healthcare expenditure and difference in cigarette demand between control states and Arizona describe the observed data. (top) Arizona, hAZ,t from equations (1) and (3) using predicted values of difference in cigarette consumption between control states and Arizona. (bottom) Predicted difference in per capita healthcare expenditure using predicted values of difference in cigarette consumption between control states and Arizona, (sc,t−sAZ,t) from equations (2) and (4). Symbols: observed values (black circles), predicted long-run cointegrating relationship (dotted line), predicted values from dynamic predictions using cointegrating and ECM equations (solid line).
Research Highlights.
There is an association between state tobacco control funding and reduced per capita cigarette consumption in Arizona, USA
The reduction in per capita cigarette consumption is associated with a reduction in per capita healthcare costs in Arizona
Acknowledgments
This research was supported by NCI grant CA-61021. The funding agency played no role in the conduct of the research, preparation of the manuscript or decision to publish.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
James Lightwood, University of California, San Francisco.
Stanton Glantz, Department of Medicine (Cardiology), University of California, San Francisco.
References
- Abadie A, Diamond A, et al. NBER Working Paper Series. w12831. National Bureau of Economic Research; 2007. Synthetic control methods for comparative case studies: Estimating the effect of California’s Tobacco Control Program. [Google Scholar]
- Aguinaga Bialous S, Glantz S. Arizona’s tobacco control initiative illustrates the need for continuing oversight by tobacco control advocates. Tob Control. 1999;8(2):141–151. doi: 10.1136/tc.8.2.141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barnoya J, Glantz S. Association of the California tobacco control program with declines in lung cancer incidence. Cancer Causes Control. 2004;15(7):689–95. doi: 10.1023/B:CACO.0000036187.13805.30. [DOI] [PubMed] [Google Scholar]
- Bialous SA, Glantz S. A Tobacco Control Policy Making: United States: Tobacco Control in Arizona, 1973-1997. 1997 Paper AZ1997. Retrieved Jan 2, 2008, from http://repositories.cdlib.org/ctcre/tcpmus/AZ1997.
- Bureau of Economic Analysis. State Annual Personal Income. 2007 Retrieved December 7, 2007, from http://bea.gov/regional/spi/default.cfm?satable=summary.
- Bureau of Labor Statistics. Consumer Price Index - All Urban Consumers (Current Series) 2007 Retrieved May, 2007, from http://data.bls.gov/PDQ/outside.jsp?survey=cu.
- Burke SP, Hunter J. Modelling Non-Stationary Economic Time Series: A Multivariate Approach. New York, NY: Palgrave McMillan; 2005. [Google Scholar]
- California State Department of Finance. California Almanac 2007: Consumer Price Index, Selected Areas. 2007 Retrieved December 7, 2007, from http://www.dof.ca.gov/HTML/FS_DATA/STAT-ABS/documents/D16.xls.
- Centers for Disease Control and Prevention. Best Practices for Comprehensive Tobacco Control Programs--2007. Atlanta, GA: Centers for Disease Control and Prevention, U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2007a. [Google Scholar]
- Centers for Disease Control and Prevention. Smoking and Tobacco Use, State Tobacco Activities Tracking and Evaluation (STATE) System. 2007b Retrieved Dec 7, 2007, from http://apps.nccd.cdc.gov/statesystem/
- Department of Health and Human Services. Health expenditures by state of provider, 1980-2004. 2007 (Final, February 2007) (compressed excel file). Retrieved December 7, 2007, from http://www.cms.hhs.gov/NationalHealthExpendData/05_NationalHealthAccountsStateHealthAccounts.asp#TopOfPage.
- Enders W. Applied Econometric Time Series. Hoboken, NJ: John Wiley and Sons; 2004. [Google Scholar]
- Engle RF, Granger C. Co-Integration and error correction: representation, estimation, and testing. Econometrica. 1987;55(2):251–276. [Google Scholar]
- Farrelly MC, Pechacek TF, et al. The impact of tobacco control program expenditures on aggregate cigarette sales: 1981-1998. Journal of Health Economics. 2001;22(203):843–859. doi: 10.1016/S0167-6296(03)00057-2. [DOI] [PubMed] [Google Scholar]
- Fichtenberg CM, Glantz SA. Association of the California tobacco control program with declines in cigarette consumption and mortality from heart disease. New England Journal of Medicine. 2000;343(24):1772–7. doi: 10.1056/NEJM200012143432406. [DOI] [PubMed] [Google Scholar]
- Gallet CA. The efficacy of state-level antismoking laws: demand and supply considerations. Journal of Economics and Finance. 2004;28(3):404–412. [Google Scholar]
- Giovino G. Cigarette Smoking Prevalence and Policies in the 50 States: An Era of Change. National Conference on Tobacco OR Health; Phoenix, AZ. 2009. [Google Scholar]
- Glantz S, Balbach E. Tobacco War: Inside the California Battles. Berkeley: University of California Press; 2000. [Google Scholar]
- Greene WH. Econometric Analysis. Upper Saddle River, NJ: Prentice-Hall; 2000. [Google Scholar]
- Gross C, Soffer B, et al. State expenditures for tobacco-control programs and the tobacco settlement. New England Journal of Medicine. 2002;347(14):1080–1086. doi: 10.1056/NEJMsa012743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haldrup N. An econometric analysis of I(2) variables. Journal of Economic Surveys. 1997;12(5):595–650. [Google Scholar]
- Hendlin YH, Barnes R, et al. Tobacco Control in Transition: Public Support and Governmental Disarray in Arizona 1997-2007. San Francisco, CA: University of California; 2008. http://repositories.cdlib.org/ctcre/tcpmus/Arizona2007. [Google Scholar]
- Hsiao C. Identification and dichotimization of long- and short-run relations of cointegrated vector autoregressive models. Econometric Theory. 2001;17:889–912. [Google Scholar]
- Hsiao C. Cowles commission structural equation approach in light of nonstationary time series analysis. In: No H-C, Ing C-K, Lai TL, editors. Time Series and Related Topics: In Memory of Ching-Zong Wei. Beachwood, Ohio: Institute of Mathematical Statistics; 2006. pp. 173–192. [Google Scholar]
- Institute of Medicine. Ending the Tobacco Problem: A Blueprint for the Nation. Washington DC: National Academies Press; 2007. from http://www.iom.edu/en/Reports/2007/Ending-the-Tobacco-Problem-A-Blueprint-for-the-Nation.aspx. [Google Scholar]
- Jemal A, V, Cokkinides E, et al. Lung cancer trends in young adults: an early indicator of progress in tobacco control (United States) Cancer Causes and Control. 2003;14(6):579–585. doi: 10.1023/a:1024891201329. [DOI] [PubMed] [Google Scholar]
- Lightwood JM, Dinno A, et al. Effect of the California tobacco control program on personal health care expenditures. PLoS Medicine. 2008;5(8):e178. doi: 10.1371/journal.pmed.0050178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maddala GS, Kim I-M. Unit Roots, Cointegration, and Structural Change. Cambridge: Cambridge University Press; 1998. [Google Scholar]
- Marlow M. Determinants of state tobacco-control expenditures. Applied Economics. 2008;40(7):831–839. [Google Scholar]
- Messer K, Pierce J. Changes in age trajectories of smoking experimentation during the California Tobacco Control Program. Am J Public Health. 2010;100(7):1298–1306. doi: 10.2105/AJPH.2009.160416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oracle Corporation. Crystal Ball Fusion Edition, Release 11.1.2. Redwood City, CA: Oracle Corp; 2000. [Google Scholar]
- Orzechowski & Walker. Tax Burden on Tobacco, Historical Compilation. Vol. 40. Arlington (VA): Orzechowski & Walker; 2005. [Google Scholar]
- Phillips PCB. Optimal Estimation of Cointegrated Systems with Irrelevant Instruments. New Haven, CT: Cowles Foundation, Yale University; 2006. [Google Scholar]
- Tobacco Control Section. A Model for Change: The California Experience in Tobacco Control. Sacramento, CA: California Department of Health Services; 1998. [Google Scholar]
- United States Census Bureau. State resident population by age and sex, 1980-1989. 2004a Retrieved December 7, 2007, from http://www.census.gov/popest/archives/1980s/80s_st_age_sex.html.
- United States Census Bureau. State resident population by age and sex, 1990-1999. 2004b Retrieved December 7, 2007, from http://www.census.gov/popest/archives/1990s/st_age_sex.html.
- United States Census Bureau. State resident population by age and sex, 2000-2006. 2008 Retrieved December 7, 2007, from http://www.census.gov/popest/states/asrh/files/SC_EST2005_AGESEX_RES.csv.
- World Health Organization. WHO Framework Convention on Tobacco Control. 2010 (webpage). Retrieved Sep 14, 2010, from http://www.who.int/fctc/en.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.