

Abstract
Adenoid cystic carcinoma is the most frequent pathology occurring in the minor salivary glands .It is usually slow growing; however, it can spread via perineural invasion, haematogenous and lymphatogenous metastasis. Most common sites of metastasis are lung and bone. Involvement of the other sites is not common. In this article, we present a woman with coincident lung and liver metastases.
Background
Adenoid cystic carcinoma (ACC) is a rare neoplasm and accounts for less than 1% of all head and neck malignancies and about 10% of salivary neoplasms,1 though it is the most frequent malignant tumour in the minor salivary glands.2 It is slow growing; however, multiple local recurrence and perineural spread is common.1–3 Haematogenous metastasis is more common than lymphatogenous metastasis .The common sites of metastasis are lung and bones; however, involvement of other organs such as liver is not common.1–3 In this paper, we present a woman with ACC of hard plate and coincidental lung and liver metastases.
Case presentation
The patient is a 53-year-old woman admitted in our ear, throat and nose clinic. She complained of haemorrhagic mass in her oral cavity. She explained that the mass had been existing for 20 years in the roof of her mouth; however, it did not grow and the patient had no other complication until 3 years ago, when she experienced episodes of self-limiting haemorrhage from this mass. Since 1 month, she had noticed a large rupture in the mass and referred to our clinic. Physical examination revealed a fairly hard mass in the right side of the hard palate extending to the alveolar region, with no satellite lesion and cervical lymphadenopathy. CT scanning revealed a soft tissue mass in the right side of the hard palate extending to the right maxillary sinus and right side of the nasal cavity with bone erosion. Multiple lung and liver contrast-enhanced lesions were seen in the images (figures 1 to 3).
Figure 1.
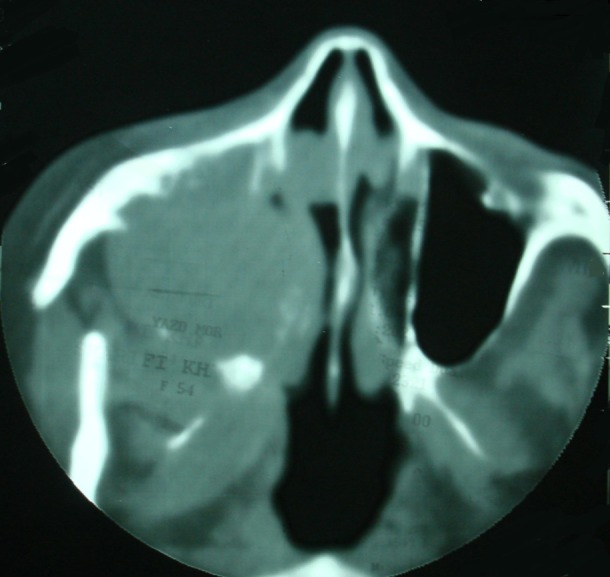
CT scanning shows a mass-filled right maxillary sinus with bone erosion.
Figure 2.

Thoracic CT scanning shows multiple pulmonary nodules in both lungs.
Figure 3.

Liver CT scanning shows multiple metastases.
Differential diagnosis
Pleomorphic adenoma with cribriform pattern, polymorphous low-grade adenocarcinoma and basaloid squamous cell carcinoma should be considered in the differential diagnosis.
Treatment
Surgical resection of primary lesion with negative margins was performed that showed adenoid cystic carcinoma. For assurance biopsy from one of the liver lesions was performed that confirmed metastasis. Then combination chemotherapy with epirubicin (50 mg/m2), cisplatin(60 mg/m2) and 5flurouracil (600 mg/m2) every 3 weeks was done for six courses.
Outcome and follow-up
Repeated CT scanning showed stable disease, and the patient was fairly well, until 1 year later that she complained of facial pain and headache. MRI with gadolinium revealed primary tumour relapse with intracranial extension (figure 4).4 Palliative radiation therapy with 4500cGY dose was done and her pains subsided successfully. Now the patient has no significant medical problem.
Figure 4.
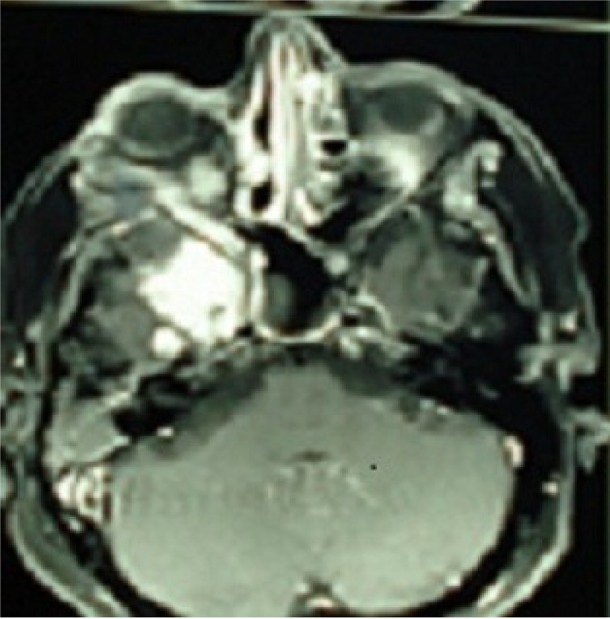
MRI shows intracranial extension of tumour.
Discussion
ACC is a slow-growing malignant tumour, more commonly seen in minor salivary glands, and hard palate is one of the most frequent sites of the disease.2 Local recurrences, intracranial spread via perineural invasion and late distant metastasis are responsible for rather low long-term survival rate.2 3 The distant organs involved in decreasing order of frequency are lung, bone, brain and liver. Other rare metastatic sites include stomach, choroids, kidney and skin.4 Spiro et al from the Memorial Sloan-Kettering Cancer Centre reported results of evaluation of 434 malignant minor salivary gland tumours. Patients with adenoid cystic carcinoma have the poorest prognosis, and about only 20% of them survive without recurrence.5 In another study by Spiro et al incidence of distant metastases in 197 ACC patients treated for cure was 42% and the patients who died from the disease this rate approached 70%; however, most of the patients with distant metastases had uncontrolled disease in the primary site or the neck. They concluded that ‘extensive local tumour infiltration, rather than distant spread, was the usual cause of death in these patients’. In this study from 93 patients showing metastatic disease only one patient had visceral metastasis without pulmonary involvement.6 Stage is the most and may be the only significant prognostic factor.2 Surgery with adequate margin is the main treatment procedure and improves local control; however, there are some controversies about the role of negative margins in the overall survival.7 Regarding high incidence of perineural invasion many authors propose adjuvant radiotherapy, and this procedure improves locoregional control and disease-free survival, although without any significant improvement of the overall survival.2 Presence of the lung metastasis in a patient with ACC does not necessarily preclude the treatment of primary disease, especially in the case of parotid tumours because of slow growth rate and with an average tumour doubling of 393 days.6 5 8 Liver is not a frequent organ of metastasis for adenoid cystic carcinoma. Kim et al evaluated 94 cases of ACC of head and neck 46 (49%) of whom showed distance metastases. Pulmonary metastasis arose in 40 patients and bone metastasis in 12. Six patients had lung and bone metastasis. Lung metastasis was followed by bone metastasis in five patients. In one patient, lung and bone metastases were concurrently found. Only one patient had lung, bone and liver metastases.9 Ninety-five percent of cases with pulmonary metastasis were asymptomatic when metastasis was diagnosed. In contrast, 83% of patients who had bone metastasis were symptomatic. The results of this study showed that development of distant metastasis was significantly higher in ACCs arising from the minor salivary glands of the oral cavity and pharynx and with solid histological subtype; however, tumour stage, age, sex, duration of symptoms, primary treatment modalities, extent of surgical resection, histological grade, perineural invasion or surgical margins of excision were not significant.9 On the other hand, Rapidis et al evaluated 23 cases with ACC of head and neck. Distant metastasis occurred in 47.8% of patients. Three patients showed liver metastasis in one of whom with lung, in another with brain and in the third with lung and spinal involvement. Solid subtype ACC and high-grade tumour were associated with a higher incidence of distant metastases; however, this association was not statistically significant. In contrast, perineural invasion was associated with both distant metastasis and adverse final outcome in a statistically significant way. There is no significant correlation between local recurrence, margin status and subsequent development of distant metastasis.10 In a single institution study in Brazil from 129 cases of head and neck ACC cases only one of them (0.8%) showed liver metastasis.11 Van der wal et al3 reported two cases of liver metastasis, besides lung metastasis. In another study Spiers et al12 presented two cases of liver metastasis in both of which liver metastasis occurred subsequent to pulmonary involvement. Deshpande et al13 introduced a case presented with hepatomegaly and fine-needle aspiration revealed ACC and further investigations showed the tumour originating from submandibular gland however they did not explain the treatment and the patient's survival. Harish et al reported a case of liver metastasis 3 years after primary parotid surgery without lung and bone involvement. The patient refused chemotherapy and died 21 months later with no evidence of local recurrence or pulmonary metastasis.4 In two separate studies liver metastasis from ACC of Bartholin gland14 and lacrimal gland15 was reported without lung and bone metastases. The paucity of literature relating to chemotherapy for adenoid cystic carcinoma stems in part from the relative rarity of these tumours.4 The information at hand would suggest that a combination of Cisplatin, Adriamycin and 5FU would be the initial chemotherapy regimen, but paclitaxel does not appear to be active on ACC.5
Distant metastasis can occur despite primary tumour control3 5 10 and about one-third of patients developed metastasis during the follow-up period without any evidence of locoregional failure. Rapidis et al according to their findings and others propose ‘The detection of distant metastases to the lungs or to other organs in asymptomatic patients is not an indication for further treatment, as radiotherapy and chemotherapy are ineffective for the management of secondary ACC deposits’.10 However, there is scarce knowledge on patients presenting with distant metastasis especially in the sites other than lung or multiple organ metastasis such as our patient. Careful decision about the treatment, especially for asymptomatic patients, by a multidisciplinary team with special emphasis on balancing between quality of life, side effects of treatment and disease control can be helpful. Our patient had the palate lesion for more than 20 years and the tumour had enough time to involve lung and liver. Since chemotherapy could not lead to an objective response and the patient was not symptomatic, it seems better to postpone chemotherapy until the patient become symptomatic. To palliate local recurrent symptoms, a lower radiation dose may be effective.
Learning points.
Although coincident lung and liver metastases is not common in adenoid cystic carcinoma (ACC) occasionally, however, it may occur.
Despite multiple gross metastases in lung and liver, ACC produces fewer symptoms.
Not with standing lung and liver metastases, the patient survived enough until local recurrence occurred.
Footnotes
Competing interests: None.
Patient consent: Obtained.
References
- 1.Matsuba HM, Spector GJ, Thawley SE, et al. Adenoid cystic salivary gland carcinoma: a histologic review of treatment failure patterns. Cancer 1986;57:519–24 [DOI] [PubMed] [Google Scholar]
- 2.Bradley JP. Adenoid cystic carcinoma of the head and neck: a review. Curr Opin Otolaryngol Head Neck Surg 2004;12:127–32 [DOI] [PubMed] [Google Scholar]
- 3.van der Wal JE, Becking AG, Snow GB, et al. Distant metastases of adenoid cystic carcinoma of the salivary glands and the value of diagnostic examinations during follow-up. Head Neck 2002;24:779–83 [DOI] [PubMed] [Google Scholar]
- 4.Harish K, Mangala Gouri SR. Adenoid cystic carcinoma of the parotid metastasizing to liver: case report. BMC Cancer 2004;4:41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Spiro RH, Huvos AG, Strong EW. Adenoid cystic carcinoma of salivary origin: a clinicopathologic study of 242 cases. Am J Surg 1974;128:512–20 [DOI] [PubMed] [Google Scholar]
- 6.Spiro RH, Koss LG, Hajdu SI, et al. Tumors of minor salivary origin: a clinicopathologic study of 492 cases. Cancer 1973;31:117–29 [DOI] [PubMed] [Google Scholar]
- 7.Kokemueller H, Eckardt A, Brachvogel P, et al. Adenoid cystic carcinoma of the head and neck—a 20 years experience. Int J Oral Maxillofac Surg 2004;33:25–31 [DOI] [PubMed] [Google Scholar]
- 8.Umeda M, Nishimatsu N, Masago H, et al. Tumor-doubling time and onset of pulmonary metastasis from adenoid cystic carcinoma of the salivary gland. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;88:473–8 [DOI] [PubMed] [Google Scholar]
- 9.Sung MW, Kim KH, Kim JW, et al. Clinicopathologic predictors and impact of distant metastasis from adenoid cystic carcinoma of the head and neck. Arch Otolaryngol Head Neck Surg 2003;129:1193–7 [DOI] [PubMed] [Google Scholar]
- 10.Rapidis AD, Givalos N, Gakiopoulou H, et al. Adenoid cystic carcinoma of the head and neck. Clinicopathological analysis of 23 patients and review of the literature. Oral Oncol 2005;41:328–35 [DOI] [PubMed] [Google Scholar]
- 11.Da Cruz Perez DE, de Abreu Alves F, Nobuko Nishimoto I, et al. Prognostic factors in head and neck adenoid cystic carcinoma. Oral Oncol 2006;42:139–46 [DOI] [PubMed] [Google Scholar]
- 12.Spiers AS, Esseltine DL, Ruckdeschel JC, et al. Metastatic adenoid cystic carcinoma of salivary glands: case reports and review of the literature. Cancer Control 1996;3:336–42 [DOI] [PubMed] [Google Scholar]
- 13.Deshpande AH, Kelkar AA. hepatic metastasis as an initial manifestation of salivary adenoid cystic carcinoma: cytologic diagnosis. Diagn Cytopathol 2009;37:45–7 [DOI] [PubMed] [Google Scholar]
- 14.Shahabi S, Nathan LM, Chanana C, et al. Liver metastasis in a case of adenoid cystic carcinoma of the Bartholin's gland: a rare presentation. Arch Gynecol Obstet 2009;279:747–50 [DOI] [PubMed] [Google Scholar]
- 15.Zeidan BA, Abu Hilal M, Al-Gholmy M, et al. Adenoid cystic carcinoma of the lacrimal gland metastasising to the liver: report of a case. World J Surg Oncol 2006;20:66. [DOI] [PMC free article] [PubMed] [Google Scholar]