

Abstract
A 27-year-old fouth gravida patient with previous two partial molar pregnancies and one missed abortion underwent a suction evacuation for partial molar pregnancy at 9 weeks of gestation. She was followed up with serum HCG values. Though the HCG level reduced from a pre-evacuation value of 1 40 223–31 157 mIU/ml 1 week post procedure, the levels continued to be positive in low titres 6 months after suction evacuation. The management options were discussed with the patient and a decision was taken to continue surveillance with serial HCG titres. HCG levels normalised after 11 months without the need for chemotherapy.
Background
Persistent raised serum HCG levels 6 months after evacuation of a molar pregnancy, even if levels fall, is considered to be an indication for chemotherapy.1 Complete and partial moles are followed by persistent gestational trophoblastic neoplasia requiring chemotherapy in 15% and 0.5% of cases, respectively.1–4 Increased risk of litigation has resulted in prophylactic chemotherapy for the fear of malignant transformation with late treatment.5–7 However, a recent retrospective study by Aggarwal et al1 suggested continued surveillance when HCG levels were found to persist even beyond 6 months. This would avoid unnecessary chemotherapy, reducing the risk of unwanted side effects and cost of therapy. Moreover, chemotherapy is not effective for small foci of slowly dividing tumour cells as in quiescent disease.8
Few cases of recurrent partial molar pregnancies have been recorded in literature. The risk of developing persistent gestational trophoblastic disease though low requires surveillance for early detection and therapy.9
Case presentation
A 27-year-old female was referred from a private clinic 4 months after suction evacuation for a partial molar pregnancy for further treatment and follow-up. Her obstetric history was significant as she had two previous partial molar pregnancies. In her first pregnancy, she was diagnosed by sonography to have a partial mole. She underwent a suction evacuation procedure, and histopathology confirmed the diagnosis of a partial mole. Her serum HCG levels normalised 5 weeks after evacuation. She conceived 3 months later, but had a medical abortion at 8 weeks gestation in view of sonographic diagnosis of a missed abortion. The products of conception were not subjected to a histopathological examination. In her third pregnancy, she again underwent a suction evacuation for a partial mole. Subsequently, she had regular menstrual cycles for 1 year, and was not followed up with serial HCG. In the index (4th) pregnancy, she had vaginal bleeding at 9 weeks of gestation. Sonography showed the intrauterine contents to be hyperechoic with multiple cystic spaces suggestive of a molar pregnancy. Her serum HCG level was 1 40 223 mIU/ml before suction evacuation which reduced to 31 157 mIU/ml 1 week after evacuation. Vaginal bleeding continued and a repeat sonography demonstrated a thick irregular endometrium with cystic areas and a 2.5 cm cyst in the right ovary. A repeat suction evacuation was done 1 week after the first. The histopathology was suggestive of a complete mole. Thereafter, the woman followed up only after 4 months when she was referred to the present hospital.
Investigations
At presentation to our hospital 4 months postevacuation, the serum HCG had reduced to 61 mIU/ml. Phantom HCG was ruled out as the urine pregnancy test was positive as well.
Outcome and follow-up
Subsequently, the serum HCG values plateaued and remained in the range 59–84 mIU/ml. CT of the head, thorax and abdomen and chest x-ray were carried out 6 months postevacuation to rule out any metastasis. Vaginal examination was normal and transvaginal ultrasound showed a thin endometrium. She continued to have regular menstruation with no evidence of abnormal uterine bleeding. The serum HCG subsequently reduced to less than 5 mIU/ml after 11 months postevacuation (figure 1).
Figure 1.
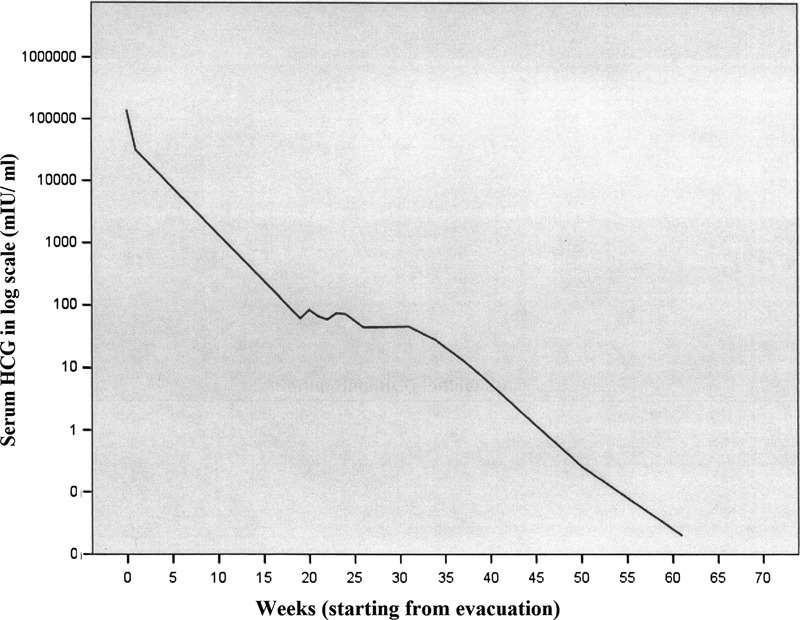
Serum HCG levels (mIU/ml) in log scale over a 1-year period after evacuation.
Discussion
Pregnancies following a partial molar pregnancy have been reported to be molar in 1.7% cases, of which 32% are complete moles.10 Recurrent molar pregnancy is not an indication for chemotherapy but persistent gestational trophoblastic disease needs chemotherapy.11
Low levels of serum HCG after 6 months of evacuation can be found in phantom HCG, pituitary HCG, placental site trophoblastic disease and quiescent HCG. Though the role of hyperglycosylated HCG to indicate the activity of the disease has been shown by Cole et al, it requires validation from larger trials. The availability of the investigation is also limited.9 Though there is no evidence of placental site trophoblastic tumor (PSTT) in this patient, long-term follow-up is required to detect late onset of its presentation.6 12
As per reported literature, this is the first case with a history of recurrent molar pregnancy that was prospectively managed conservatively with surveillance of low levels of serum HCG even 6 months after evacuation. The levels reverted to normal and the patient showed no evidence of recurrence of molar pregnancy. She will be kept under follow-up with serum HCG for six more months and further.
Learning points.
A conservative approach can be followed for persistently raised low levels of serum HCG in women with recurrent molar pregnancy.
Surveillance for low levels of serum HCG may be used for follow-up and to select women for chemotherapy.
Footnotes
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Agarwal R, Teoh S, Short D, et al. Chemotherapy and human chorionic gonadotropin concentrations 6 months after uterine evacuation of molar pregnancy: a retrospective cohort study. Lancet 2012;379:130–5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hancock BW, Nazir K, Everard JE. Persistent gestational trophoblastic neoplasia after partial hydatidiform mole incidence and outcome. J Reprod Med 2006;51:764–6 [PubMed] [Google Scholar]
- 3.Bagshawe KD, Dent J, Webb J. Hydatidiform mole in England and Wales 1973–83. Lancet 1986;328:673. [DOI] [PubMed] [Google Scholar]
- 4.Seckl MJ, Fisher RA, Salerno GA, et al. Choriocarcinoma and partial hydatidiform moles. Lancet 2000;356:36–9 [DOI] [PubMed] [Google Scholar]
- 5.Powles T, Young A, Sammit A. The significance of the time interval between antecedent pregnancy and diagnosis of high-risk gestational trophoblastic tumours. Br J Cancer 2006;95:1145–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Schmid P, Nagai Y, Agarwal R. Prognostic markers and long-term outcome of placental-site trophoblastic tumours: a retrospective observational study. Lancet 2009;374:48–55 [DOI] [PubMed] [Google Scholar]
- 7.Palmieri C, Dhillon T, Fisher RA. Management and outcome of healthy women with a persistently elevated beta-hCG. Gynecol Oncol 2007;106:35–43 [DOI] [PubMed] [Google Scholar]
- 8.Cole LA, Muller CY. Hyperglycosylated hCG in the management of quiescent and chemorefractory gestational trophoblastic diseases. Gynecol Oncol 2010;116:3–9 [DOI] [PubMed] [Google Scholar]
- 9.Boafo-Yirenki M, Everard J, Tidy J, et al. A conservative approach in persistent low-level elevation of serum beta-human chorionic gonadotropin following chemotherapy for gestational trophoblastic neoplasia. J Reprod Med 2009;54:288–90 [PubMed] [Google Scholar]
- 10.Sebire NJ, Fisher RA, Foskett M, et al. Risk of recurrent hydatidiform mole and subsequent pregnancy outcome following complete or partial hydatidiform molar pregnancy. BJOG 2003;110:22–6 [PubMed] [Google Scholar]
- 11.Koc S, Ozdegirmenci O, Tulunay G, et al. Recurrent partial hydatidiform mole: a report of a patient with three consecutive molar pregnancies. Int J Gynecol Cancer 2006;16:940–3 [DOI] [PubMed] [Google Scholar]
- 12.Palmieri C, Fisher RA, Sebire NJ, et al. Placental site trophoblastic tumour arising from a partial hydatidiform mole. Lancet 2005;366:688. [DOI] [PubMed] [Google Scholar]