

Abstract
A 3-year-old boy presented with complaints of abnormal genitalia. On examination, there was penile duplication with two completely separate phalluses, unequal in size, one with hypospadias and the other with meatus at the tip of the glans. Voiding cystourethrography revealed a normal sized single bladder but two urethras with no associated vesicoureteral reflux.
Background
This is a rare case of isolated complete penile duplication with no other associated systemic anomaly.
Case presentation
A 3-year-old boy was admitted with complaints of abnormal genitalia. The child was born by vaginal delivery and his antenatal history was uneventful. There was no history of oral contraceptives intake by the mother, no radiation exposure or infection during gestation period, and no significant family history was reported. On examination, there were two completely separate phalluses, unequal in size, one with hypospadias and the other with normal meatus (figure 1).
Figure 1.

Isolated complete diphallus with soft tissue mass in the scrotum.
There was a history of dribbling of urine from the hypospadic smaller sized phallus and continuous flow from the other phallus while micturating. Each phallus was found to have an apparently normal corpus cavernosum. The scrotum was well developed with palpable normal sized testis separated by soft tissue mass. The anal opening was at its normal site, and the anal sphincter had a normal tone.
Investigations
A karyotyping study showed 46XY. x-Rays of the spine and pelvis were normal. Abdominal ultrasonography and CT were normal. Intravenous urography (IVP) showed bilateral normal functioning of the kidneys. Baseline blood investigations were within the normal range. Voiding cystourethrography revealed no vesicoureteral reflux, a normal single bladder and two urethras (figure 2).
Figure 2.
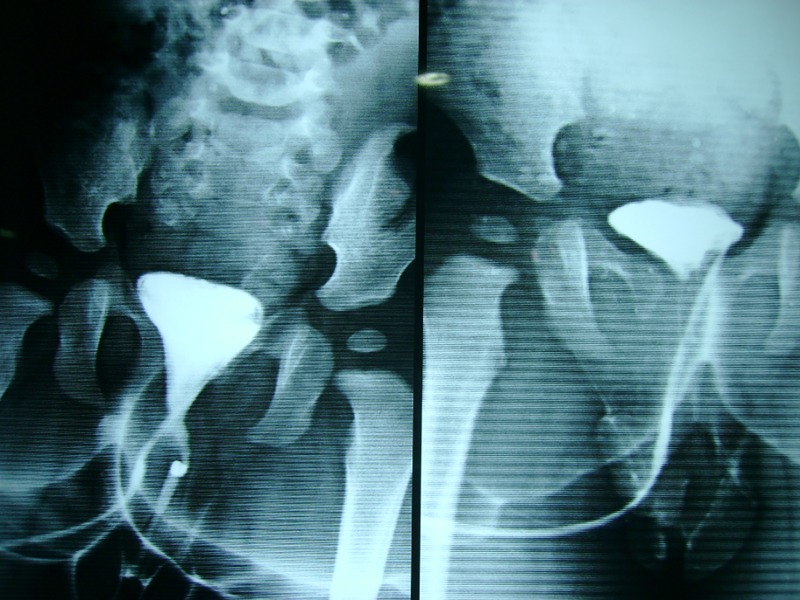
Voiding cystourethrograph showing two urethras with a single bladder and no vesicoureteral reflux.
Treatment
Surgical procedure included the following steps: penile dissection up to the ischiopubic region; dissection of the hypoplastic urethra; amputation of the smaller phallus; urethral anastomosis and phalloplasty. The postoperative period was uneventful.
Discussion
Diphallus or duplication of the penis is one of the very rare congenital anomalies of the urogenital system. It has an incidence of 1 in 5 million live-births.1 Wecker2 first reported diphallia in the literature in 1609. About 100 cases have been reported worldwide till now.3 The extent of duplication and the number of associated anomalies vary greatly from glans duplication arising from a common shaft to complete duplication of the penis accompanied by multiple anomalies including ventral hernia, bladder exstrophy, vesicointestinal fissure, bladder duplication, ureteral and renal defects, imperforate anus, ectopic scrotum, prepenile scrotum and meningomyelocele.4–8 According to Schneider,9 diphallia has been divided into three categories: (1) glans duplication, (2) bifid diphallia and (3) complete diphallia or complete penis duplication. Later, Vilanova and Raventos10 added a fourth category, namely pseudodiphallia.
All cases of diphallia need to be evaluated carefully and completely in view of the high incidence of systemic anomalies. Prognosis is largely dependent on whether it is a case of penile duplication with multiple associated anomalies or one of isolated penile duplication. The duplication of the phallus may be orthotopic or ectopic, symmetric or asymmetric in shape and size. Currently, widely accepted classification includes two main types: true diphallia and bifid phallus.11 These two types are further divided into partial or complete. True complete diphallia or complete penile duplication is described as a case where each phallus has two corpora cavernosa and a corpus spongiosum. When one of the penises is smaller or rudimentary, it is called true partial diphallia. The term bifid phallus is used when only one corpus cavernosum is present in each penis. When the degree of separation is complete up to the base of the shaft, it is called complete bifid phallus. Penile duplication is usually associated with other systemic anomalies, such as bladder and urethral duplication, cloacal exstrophy, imperforate anus, gastrointestinal duplications and vertebral anomalies, and it may also present as an isolated anomaly.8 12 13
Detailed studies of embryological anatomy of the genital tubercle have thrown light on the understanding of diphallus. The development of the normal phallus begins with the joining of bilateral cloacal tubercles at the anterior end of pars phallic of the urogenital sinus.14 Mesodermal columns grow rapidly around the lateral margin of the cloacal plate from the genital tubercle.
Various possible embryological explanations for diphallia are as follows:
Historically, Cecil15 had suggested that penile and bladder duplication are considered the end result of incompletely fused bilateral anlagen or a form of atavism, because snakes and lizards possess a double penis.
Ravitch16 reported that diphallia could represent a teratoid structure or a form of incomplete twinning.
De vries and Friedland17 described that inhibited growth of the dorsal inferior wall of the urogenital sinus underlay accessory urethral development.
Das and Brosman18 hypothesised that abnormal Mullerian duct termination was responsible for urethral duplication.
Hollowell et al19 described that diphallia results from the failure of fusion of mesodermal bands.
Woodhouse and Williams20 attributed it to an ischaemic process in embryogenesis.
Troyer21 proposed that maldevelopment of the distal portion of the urethra is because of the uncoordinated growth of the urogenital sinus and the urethral plate.
There are multiple embryological explanations for diphallia and systemic anomalies, but most researchers agree that it is a defect connecting the genital tubercle. It is hypothesised that diphallia during the gestation period occurs between 23 and 25 days, when the fetal caudal mass of the mesoderm is deeply disturbed by trauma, drugs or infections.
Management of diphallia poses a challenge in view of the medical, surgical and ethical decision-making. Patients with diphallia should undergo a thorough evaluation to rule out associated anomalies. Furthermore, a detailed anatomy of the external genitalia also helps to classify not only the degree of penile duplication but also in the planning of surgical procedure. MRI is currently the non-invasive imaging for interpretation of the anatomy of complex genital anomalies.22 Treatment of isolated diphallus includes excision of the duplicated penile structure and its urethra.23 24
Learning points.
Complete penile duplication is a rare congenital genitourinary condition.
Patients of penile duplication should be evaluated in detail to rule out any associated systemic anomaly.
Treatment includes excision of the duplicated penile structure and its urethra.
Footnotes
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Lewis EL. Ectopic scrotum and diphallia—report of a case. J Urol 1960;84:115. [DOI] [PubMed] [Google Scholar]
- 2.Wecker S. Pene gemino visus quidam. Obs. Med. admirab.—Lib. 4. De partibus genitalibus, Francoforti, 1609
- 3.Sharma KK, Jain SK, Purohit A. Concealed diphallus, a case report and review of the literature. JIAPS 2000;5:18–21 [Google Scholar]
- 4.Kaufman A, Guia R, Devila H. Diphallus with third urethra. Urology 1990;35:257–60 [DOI] [PubMed] [Google Scholar]
- 5.Gammie WP, Davies JH. Diphallus in an adult. Br J Urol 1988;62:185–6 [DOI] [PubMed] [Google Scholar]
- 6.Agrawal S, Sogani SK. Diphallus. J Pediatr Surg 1984;19:213–14 [DOI] [PubMed] [Google Scholar]
- 7.Rao TV, Chandra Sekharam V. Diphallus with duplication of cloacal derivatives—report of a rare case. J Urol 1980;124:555–7 [DOI] [PubMed] [Google Scholar]
- 8.Azmy AF. Complete duplication of the hindgut and lower urinary tract with diphallus. J Pediatr Surg 1990;25:647–9 [DOI] [PubMed] [Google Scholar]
- 9.Schneider P. cited by Lattimer JK, Uson AC. The male genital tract. In: Mustard WT, Ravitch MM, Synder WH, Welch K, Benson CD, eds. Pediatric surgery. 2nd edn Vol II Chicago: Year Book Medical Publishers, 1969:1163 [Google Scholar]
- 10.Vilanova X, Raventos A. Pseudodiphallia—a rare anomaly. J Urol 1954;71:338–46 [DOI] [PubMed] [Google Scholar]
- 11.Aleem AA. Diphallia: report of a case. J Urol 1972;108:357–8 [DOI] [PubMed] [Google Scholar]
- 12.Rock SD, Gearhart JP. Complete lower urinary tract duplication with true diphallia presenting as a rare covered exstrophy variant. J Urol 1997;157:1907–8 [PubMed] [Google Scholar]
- 13.Ciftci AO, Senocak ME, Buyukpamukcu N, et al. Complete duplication of the bladder and urethra: a case report and review of literature. J Pediatr Surg 1995;30:1605–6 [DOI] [PubMed] [Google Scholar]
- 14.Stephans FD, Smith ED, Hutson JM. Congenital anomalies of the urinary and genital tracts. Oxford: Isis Medical Media, 1996: 83–4 [Google Scholar]
- 15.Cecil AB. Anatomy, anomalies and injuries of the penis. In: Cabot H, ed. Modern urology. Philadelphia, PA: Lea and Febiger, 1936:162 [Google Scholar]
- 16.Ravitch MM. Hind gut duplication—doubling of colon and genital urinary tracts. Ann Surg 1953;137:588–601 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.De vries PA, Friedland GW. Congenital ‘H-type’ anourethral fistula. Radiology 1974;113:397. [DOI] [PubMed] [Google Scholar]
- 18.Das S, Brosman SA. Duplication of the male urethra. J Urol 1977;117:452. [DOI] [PubMed] [Google Scholar]
- 19.Hollowell JG, Witherington R, Ballayas AJ. Embryologic considerations of diphallus and associated anomalies. J Urol 1977;117:728–32 [DOI] [PubMed] [Google Scholar]
- 20.Woodhouse CRJ, Williams DI. Duplications of the lower urinary tract in children. Br J Urol 1979;51:481. [DOI] [PubMed] [Google Scholar]
- 21.Troyer JR. Urethral duplications. Dial Pediatr Urol 1987;10:2 [Google Scholar]
- 22.Lapointe SP, Wei DC, Hricak H, et al. Magnetic resonance imaging in the evaluation of congenital anomalies of the external genitalia. Urology 2001;58:452–6 [DOI] [PubMed] [Google Scholar]
- 23.Abdulkadir T, Mert A, Unsal O, et al. Complete diphallus in a 14-year-old boy. Marmara Med J 2007;20:190–2 [Google Scholar]
- 24.Carvalho AP, Ramires R, Soares J. et al. Surgical treatment of complete penile duplication. Actas Urol Esp 2008;32:941–4 [DOI] [PubMed] [Google Scholar]