

Abstract
Posterior cortical atrophy (PCA), also known as Benson's disease, has been previously reported as a variant of Alzheimer's disease (AD). We present a clinical picture and MRI findings of a patient with PCA who developed early right-sided homonymous haemianopia and marked atrophy of parieto-occipital regions of the brain before a cognitive decline appeared. This case demonstrates that PCA may appear with advanced brain atrophy at the onset of focal visual deficits before the development of progressive dementia, and adds to the knowledge of dementias with rapid progression.
Background
Posterior cortical atrophy (PCA) is a condition with initial visual disturbances without any evidence of ocular abnormalities. The visual deficits persist, and the patients gradually develop cognitive impairment reflecting parietal or occipital dysfunction and verified by neuropsychological examination.1–4 Diagnostic criteria for PCA have been proposed.4 PCA and Alzheimer's disease (AD) share in common an abnormal cerebrospinal fluid (CSF) with an equal distribution of amyloid-β deposition,5 but positron emission tomography (PET)-studies have shown that impaired glucose metabolism is more posterior located in PCA than AD.6 MRI studies have demonstrated that PCA patients during the course of the disease develop atrophy in the parietal and occipital regions with relatively sparing the hippocampus which is commonly affected in early AD.7 Although PCA is regarded as a subgroup of AD, younger age at disease onset, the topographic distributions of atrophy and metabolic disturbances are features that differ from a typical AD picture. Brain atrophy assessed by MRI along with clinical evaluation is regarded as the best outcome measurements of AD,8 while better knowledge about how earlier disease markers such as amyloid-β and τ-protein can be used in the process of developing disease-modifying treatment is needed. The sequential development of biological abnormalities with early deposits of amyloid-β and τ-protein are described in AD, but not in PCA.9 This case demonstrates that visual disturbances with focal atrophy on MRI may indicate the onset of a more aggressive AD, alternatively a separate form of rapid progressive dementia in younger adults. Marked focal brain atrophy on MRI may be present at the onset of visual symptoms, and may probably have been developed during a preclinical state in the present PCA patient.
Case presentation
A 52-year-old secretary treated for hypothyreosis was admitted to the neurological department for acute dizziness, and visual impairment lasting about a month. She was not able to get hold of items she reached for and failed when she entered digits on her telephone. She performed well at work, and during hospitalisation she appeared cognitively normal. The only finding at clinical and neurological examination was right-sided homonymous haemianopia. Complete blood count, C reactive protein (CRP), aspartate aminotransferase (ASAT), alanine aminotransferase (ALAT), alkaline phosphatase (ALP), gamma-glutamyltransferase (GT), creatinine and electrolytes and ultrasonographic Doppler of her carotid and vertebral arteries were normal. Visual evoked potential (VEP) did not reveal pathology. A perimetry revealed right-sided homonymous haemianopia most pronounced in the lower quadrants on both sides without macular sparing (figure 1). MRI of the brain with angiography showed pronounced posterior brain atrophy with broadened sulci in the occipital and parietal lobes, slightly more pronounced on the left side and to a lesser extent in the temporal lobes, and with sparing of the hippocampal regions (figures 2–4). Her dizziness improved, and she was discharged from hospital.
Figure 1.

Perimetry illustrating right-sided homonymous haemianopia.
Figure 2.
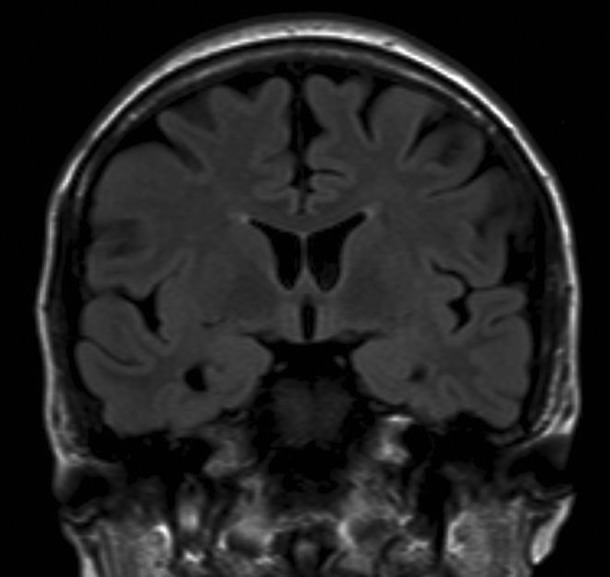
Coronal T1 MRI of progressive cortical atrophy showing marked atrophy of the parietal regions with normal hippocampus.
Figure 3.
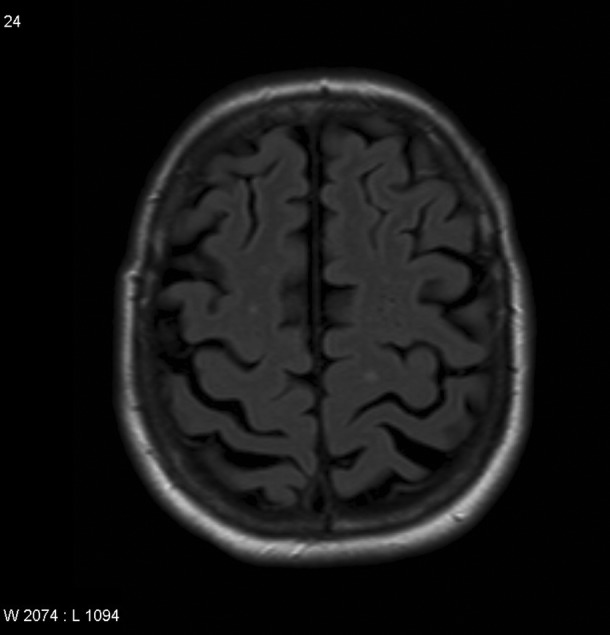
Transversal T1 showing bilateral marked atrophy in the parieto-occipital region.
Figure 4.
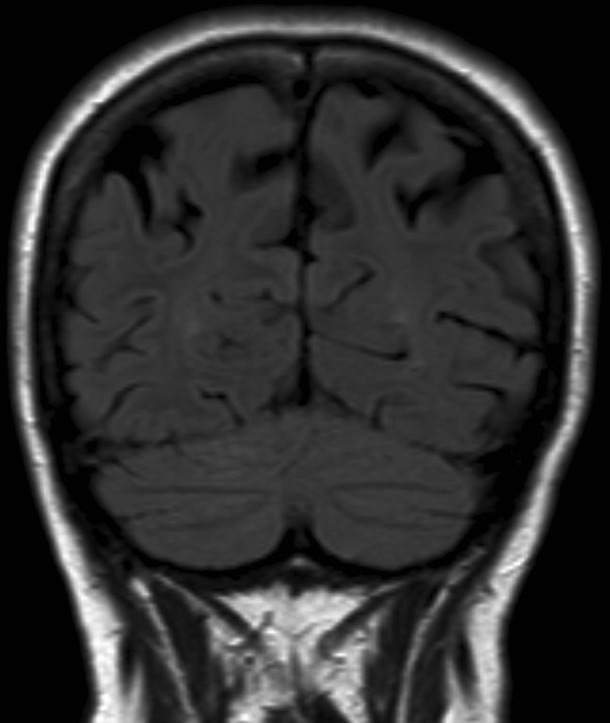
Coronal T1 MRI of progressive posterior cortical atrophy.
On the follow-up consultation 2 months later, relatives reported that her cognitive functioning had deteriorated drastically for the past 2 months. She had difficulties concentrating, repeating herself 20–30 times daily and she did not know what to do and how to behave in common daily situations. She neither knew how to cook nor serve food. Mini mental status (MMS) examination scored 24 of 30 points. A spinal puncture was performed. Leucocytes, protein and glucose were within the reference range, and there were no abnormalities on isoelectric focusing. Dementia markers in the spinal fluid showed increased T-τ (1360 ng/ ml) and p-τ (221 ng/ ml), and a decrease in amyloid-β (404 ng/ml) consistent with AD.
During the follow-up consultation 3 months later, she complained of impaired memory. She did not remember the information given to her during the previous consultations. EEG showed a slow frontotemporal background rhythm. Brain single-photon emission CT (SPECT) was consistent with reduced perfusion in both parietal lobes. Three months after discharge, the result of extensive cognitive assessment by neuropsychological tests revealed a global cognitive impairment that is considered to pose a significant decline from the patient's estimated premorbid level of functioning. The final diagnosis matched with PCA.
Investigations
▶ Complete blood count, CRP, ASAT, ALAT, ALP, GT, creatinine and electrolytes
▶ Brain MRI
▶ Ultrasonographic Doppler of carotid and vertebral arteries
▶ Perimetry
▶ VEP
▶ Brain SPECT
▶ CSF analysis of leucocytes, protein, glucose, isoelectric focusing and dementia biomarkers
Differential diagnosis
Differential diagnoses to consider are AD, dementia with Lewy bodies (DLB), Creutzfeldt Jakob's disease, cerebrovascular disease and demyelinating disease.
Treatment
Treatment with donepezil 10 mg once daily was initiated 3 months after discharge.
Outcome and follow-up
After 9 months she obtained 22 of 30 points on MMS, and the right-sided homonymous haemianopia was unchanged on perimetry.
Discussion
PCA is known as a focal neurodegenerative brain disorder with early visual disturbances followed by progressive cognitive deterioration, but the dynamics of the progression are not well known. The disease is not only predictive of AD, but is also reported in other brain disorders such as corticobasal degeneration, DLB and prion-associated disease according to one study.10 The most striking observation in the present case was that despite a relatively preserved cognitive function there was an advanced stage of brain atrophy at the time of symptom onset, which is consistent with a rapid progressive neurodegenerative disorder (figures 2–4). There is no evidence from the literature that PCA represents a more serious dementia syndrome compared to AD, but PCA typically differs from AD with more atrophy in the parieto-occipital regions in contrast to AD that especially affects medial temporal regions (hippocampus).7 Analogous to this, autopsy studies demonstrate a higher density of neurofibrillary tangles in occipital areas in PCA.4 11 A previous longitudinal report, showing that the symptoms in principle remained focally distributed over time,12 was later confirmed by another follow-up study with brain perfusion and neuropsychological scores.13 A similar pattern of brain atrophy has been found in AD with early onset, while those with later onset, that is, after 65 years, showed a more traditional AD picture with hippocampal atrophy in some reports.14 15 Others have shown less association between brain atrophy and different phenotypes of AD.16 The present case with early and probably preclinical brain atrophy in PCA demonstrates the huge biological variation in the disease, and the need for larger prospective cohort studies. Although more studies on the natural course of PCA are needed, younger age and similar focal distribution of brain atrophy may hypothesise a possible common predisposing genetic or environmental factor in PCA and younger onset AD. Early brain atrophy and rapid functional decline in the present PCA patient are in line with the assumption that brain atrophy predicts disease severity in AD.8 Distribution of atrophy has been related to domains of cognitive dysfunction in AD,17 but clinical studies integrating atrophic brain changes on MRI and PET-imaging studies should include PCA. Changes in fluorodeoxyglucose (FDG)-PET, CSF amyloid-β, T-τ and P-τ often precede clinical presentation of AD, and hypotheses using these biomarkers in staging systems of AD have been proposed.9 Future studies should aim at identifying risk factors of PCA and evolution of the disease.
Dementia is an important condition to consider in cases of visual field impairment. MRI techniques sensitive to volume defects of the brain are important to perform in patients with visual field abnormalities or other higher order visual defects. Whether initial visual field impairment, PCA on imaging studies and CSF biomarkers may be associated with a more serious prognosis in PCA needs further investigation. Few cases with PCA responding to treatment with cholinesterase inhibitors have previously been reported.18 Clinical trials to determine the efficacy of cholinesterase inhibitors in PCA are under way at The Institute of Neurology, Queen Square City London.
Learning points.
▶ Visual field defects can be the first sign of dementia.
▶ Loss of brain tissue may be found to precede cognitive and behavioural symptoms of dementia.
▶ Cholinesterase inhibitors may have an effect, and even hamper disease progression and should be tried early in posterior cortical atrophy.
Footnotes
Competing interests: None.
Patient consent: Obtained.
References
- 1.Cogan DG. Visual disturbances with focal progressive dementing disease. Am J Ophtalmol 1985;100:68–72 [DOI] [PubMed] [Google Scholar]
- 2.Benson DF, Davis RJ, Snyder BD. Posterior cortical atrophy. Arch Neurol 1988;45:789–93 [DOI] [PubMed] [Google Scholar]
- 3.Alladi S, Xuereb J, Bak T, et al. Focal cortical presentations of Alzheimer's disease. Brain 2007;130:2636–45 [DOI] [PubMed] [Google Scholar]
- 4.Tang-Wai DF, Graff-Radford NR, Boeve BF, et al. Clinical, genetic, and neuropathologic characteristics of posterior cortical atrophy. Neurology 2004;63:1168–74 [DOI] [PubMed] [Google Scholar]
- 5.deSouza LC, Corlier F, Habert MO, et al. Similar amyloid-β burden in posterior cortical atrophy and Alzheimer's disease. Brain 2011;134:2036–43 [DOI] [PubMed] [Google Scholar]
- 6.Rosenblom MH, Alkaly A, Agarwal N, et al. Distinct clinical and metabolic deficits in PCA and AD are not related to amyloid distribution. Neurology 2011;76:1789–96 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Whitwell JF, Jack CR, Jr, Kantarci K, et al. Imaging correlates of posterior cortical atrophy. Neurobiol Aging 2007;28:1051–61 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Weiner MW, Veitch DP, Aisen PS, et al. The Alzheimer's disease neuroimaging initiative: a review of papers published since its inception. Alzheimers Dementia 2012;8:S1–S68 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Jack CR, Jr, Knopman DS, Jagust WJ, et al. Hypothetical model of dynamic biomarkers of the Alzheimer's pathological cascade. Lancet Neurol 2010;9:119–28 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Renner JA, Burns JM, Hou CE, et al. Progressive posterior cortical dysfunction. Neurology 2004;63:1175–80 [DOI] [PubMed] [Google Scholar]
- 11.Hof PR, Vogt BA, Bouras C, et al. Atypical form of Alzheimer's disease with prominent posterior cortical atrophy: a review of lesion distribution and circuit disconnection in cortical visual pathways. Vision Res 1997;37:3609–25 [DOI] [PubMed] [Google Scholar]
- 12.McMonagle P, Deering F, Berliner Y, et al. The cognitive profile of posterior cortical atrophy. Neurology 2006;66:331–8 [DOI] [PubMed] [Google Scholar]
- 13.Kas A, de Souza LC, Samri D, et al. Neural correlates of cognitive impairment in posterior cortical atrophy. Brain 2011;134:1464–78 [DOI] [PubMed] [Google Scholar]
- 14.Frisoni GB, Pievani M, Testa C, et al. The topography of grey matter involvement in early and late onset Alzheimer's disease. Brain 2007;130:720–30 [DOI] [PubMed] [Google Scholar]
- 15.Frisoni GB, Testa, Sabattoli F, et al. Structural correlates of early and late onset Alzheimer's disease voxel based morphometric study. J Neurol Neurosurg Psychiatry 2005;76:112–14 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Migliaccio R, Agosta F, Rascovsky K, et al. Clinical syndromes associated with posterior atrophy: early age at onset AD spectrum. Neurology 2009;73:1571–8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.McDonald CR, Gharapetian L, McEvoy LK, et al. Relationship between regional atrophy rates and cognitive decline in mild cognitive impairment. Neurobiol Aging 2012;33:242–53 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kim E, Lee Y, Lee J, et al. A case with cholinesterase inhibitor responsive asymmetric posterior cortical atrophy. Clin Neurol Neurosurg 2005;108:97–101 [DOI] [PubMed] [Google Scholar]