

Abstract
Stress fractures are common injuries in sports medicine. Among these fractures, femoral neck stress fractures frequently have a benign course, especially when it happens in the medial aspect of the neck. This case report describes a stress fracture of the medial aspect of the femoral neck that developed a complete fracture and underwent surgical fixation.
Background
Stress fractures are common injuries both in recreational and professional athletes. Repetitive load causes microlesions of the bone and leads to mechanical failure, usually characterised by a stress bone reaction with no cortical discontinuation. Most frequently, it affects weight-bearing bones, as seen in runners, jumpers, skaters and military.1 2
Stress fractures have been described since the forties.3 4 Initially, they were known as march fractures because the first reported cases occured in soldiers during the World War II. The femur accounts for 7.2% of stress fractures.1 This case report describes a femoral neck stress fracture with an unusual clinical course.
Case presentation
A 56-year-old female patient presented to our clinic with a history of 1 week of left hip pain with no trauma. The patient was otherwise healthy and active, practising sports three times a week, mainly strengthening at the gymnasium, and jogging. At physical examination, the patient deambulated with no aiding device, she had a negative Trendelemburg sign, she had full range of motion of the hip with mild pain, and tenderness over the greater trochanter. An anteroposterior pelvic radiograph was considered normal (figure 1). She was discharged with anti-inflammatory drugs and a prescription for an elective MRI with the hypothesis of trochanteric bursitis.
Figure 1.

Anteroposterior radiography of the pelvis at initial presentation. This x-ray was considered normal.
After 5 days, the patient returned to our office reporting worsening of the pain despite medication. The MRI demonstrated oedema of the medial femoral neck with no evidence of a fracture line (figure 2). A medial (compression) stress fracture of the femoral neck was diagnosed, and the patient was advised to use crutches with no weight bearing on the affected limb. Because of the atypical presentation, an investigation for bone metabolism disorder was conducted. The patient had no history of previous fractures, bone disease, rheumatological disorders or biphosphonate use. Her alkaline phosphatase level was within normal limits. Radiographs of her skull, lumbar spine and tibia did not demonstrate any abnormal findings (figure 3).
Figure 2.
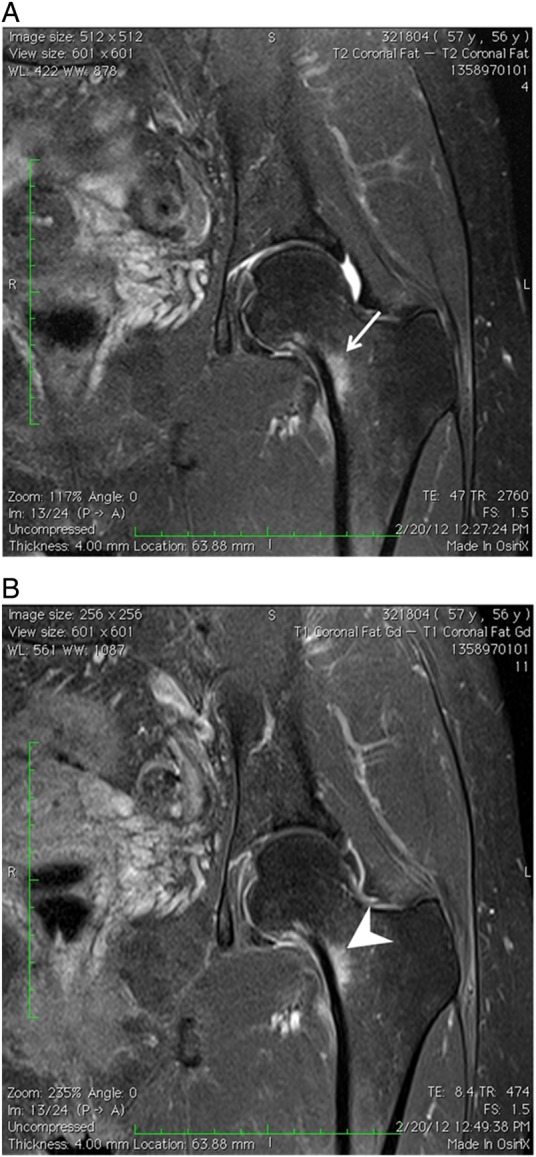
Coronal T2-weighted fat saturated (A) and Coronal T1-weighted fat saturated postgadolinium (B) MR images of left hip demonstrating area of bone marrow oedema adjacent to the medial femoral neck cortex (arrow). Note that the area of bone marrow oedema demonstrates enhancement without focal bone lesion (arrow head). There is also mild soft tissue oedema, without evidence of cortical rupture.
Figure 3.

(A) Radiographs obtained for investigation of bone metabolism disorder were considered normal. Lateral skull radiograph. (B) Tibia anteroposterior radiograph. (C) Lumbar spine lateral radiograph.
During the same day of consultation, the patient presented severe pain during a rotational movement of the hip at a physical therapy session. She went to the emergency department unable to bear weight on the affected leg. Radiographic examination, including x-ray and CT scan demonstrated a complete fracture of the femoral neck with subtle displacement (figure 4). The patient was admited to the hospital and closed reduction with percutaneous fixation was performed with three lag screws. The patient was kept on crutches for 12 weeks. After 4 months, the fracture was considered healed, and 6 months after surgery, the patient was symptom-free and was able to resume her activities (figure 5).
Figure 4.

(A) Anteroposterior radiography of the pelvis demonstrating area of cortical thickening of to the left femoral neck cortex with linear lucency suggesting a minimally displaced fracture. (B) Coronal reformat CT image of the left hip demonstrating a minimally displaced oblique fracture of the left femoral neck cortex.
Figure 5.

Postoperative radiographs demonstrating three fixation screws within the femoral neck. Note that the femoral neck stress fracture demonstrates callus formation, without deviation.
Discussion
Stress fractures are overload fractures, which can be defined by partial or complete fractures that result from repetitive load, less than the necessary to fracture the bone in a single event.5 This cyclic load creates an inbalance between bone production and resorption, weekenig the bone. Stress fractures are responsible for approximately 10% of all sports-related injuries, and the tibia is the most frequent location.1
Patients with femoral neck fractures usually present with groin pain and lateral trochanteric pain.6 Physical examination is not specific. x-Rays are frequently normal, and bone scans and MRI are necessary to confirm the diagnosis. Femoral neck stress fractures are classified as compression or tension fractures, and as displaced or non-displaced.7 Compression fractures occur at the medial femoral neck and tension fractures occur at the lateral femoral neck. Non-displaced compression fractures are the most common, and can be treated non-operatively with non-weight bearing.8 Tension fractures are associated with greater morbidity and are treated operatively. Pihlajamaki et al9 published a case series of femoral neck stress fractures. In their series, patients with displaced femoral neck fractures presented 29% of avascular necrosis, and 38% of severe osteoarthritis of the hip joint.
Therefore, this case report presents an unusual case of a femoral neck stress fracture. The patient had oedema of the medular bone, with no fracture line, thus an initial stage stress fracture. The oedema was on the medial side of the bone, considered as the compression side, possibilitating conservative treatment. Although the benign presentation, the patient developed a complete displaced fracture necessitating surgical treatment. Fortunately, despite this unusual course, the clinical outcome was excellent.
In conclusion, we report a femoral stress fracture with benign characteristics with an uncommon and serious complication. Patients with femoral neck stress fractures must be advised since their initial office visit of the potential complications of this pathology.
Learning points.
▶ Femoral neck stress fractures usually need MRI and/or bone scan to be diagnosed.
▶ Fractures can be divided in compression and tension fractures.
▶ Compression fractures can be treated conservately.
▶ Rarely, compression fractures can displace.
▶ Early diagnosis and treatment are of paramount importance to avoid late complications.
Acknowledgments
The authors would like to thank Felipe Souza for his kind review of the radiographic images.
Footnotes
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Matheson GO, Clement DB, McKenzie DC, et al. Stress fractures in athletes. A study of 320 cases. Am J Sports Med 1987;15:46–58 [DOI] [PubMed] [Google Scholar]
- 2.Kadel NJ, Teitz CC, Kronmal RA. Stress fractures in ballet dancers. Am J Sports Med 1992;20:445–9 [DOI] [PubMed] [Google Scholar]
- 3.Branch H. March fractures of the femur. J Bone Joint Surg Am 1944;26:387–91 [Google Scholar]
- 4.Peterson L. March fracture of the femur—report of a case. J Bone Joint Surg Am 1942;24:185–8 [Google Scholar]
- 5.Ivkovic A. Stress fractures of the femoral shaft in athletes: a new treatment algorithm. Br J Sports Med 2006;40:518–20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Talbot JCJ, Cox GG, Townend MM, et al. Femoral neck stress fractures in military personnel—a case series. J R Army Med Corps 2008;154:47–50 [DOI] [PubMed] [Google Scholar]
- 7.Devas MB. Stress fractures of the femoral neck. J Bone Joint Surg Br 1965;47:728–38 [PubMed] [Google Scholar]
- 8.Lassus J, Tulikoura I, Konttinen YT, et al. Bone stress injuries of the lower extremity: a review. Acta Orthop Scand 2002;73:359–68 [DOI] [PubMed] [Google Scholar]
- 9.Pihlajamäki HK, Ruohola J-P, Kiuru MJ, et al. Displaced femoral neck fatigue fractures in military recruits. J Bone Joint Surg Am 2006;88:1989–97 [DOI] [PubMed] [Google Scholar]