

Abstract
We report a case of neglected anterior dislocation of the hip. A young man presented 5 months following a fall from a tree where he sustained the injury. An MRI of the hip confirmed avascular necrosis of the dislocated head of femur. A modified girdlestone operation was performed leaving the patient with a painfree functional hip.
Background
Of the 204 cases of dislocation of the hip collected by Thompson and Epstein1, only 18 were anterior. Old unreduced anterior dislocations of the hip are extremely rare and are seen when orthopaedic help is not available in acute situations. A review of English language literature produced 17 cases.2–6 We report one such case which we noticed during a posting in rural India.
Case presentation
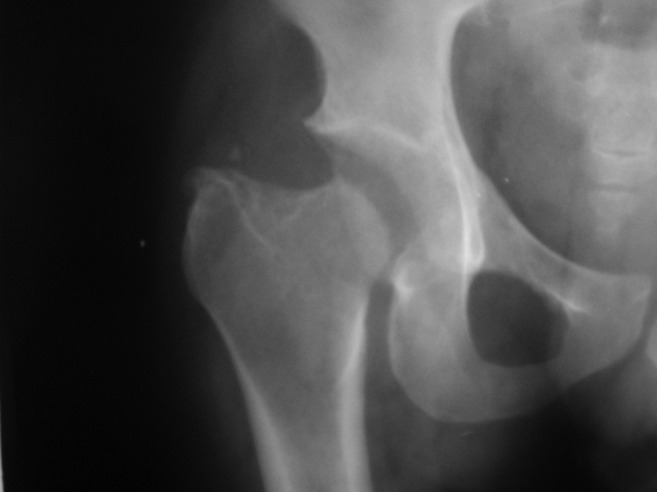
A 25-year-old man presented with a history of fall from a tree 5 months previously. Clinically and radiographically (figure 1), an unreduced anterior dislocation of the right hip was diagnosed. He had exaggerated lumbar lordosis, and the pelvis was lower on the affected side. The limb was in flexion and external rotation. He could walk only a few metres using a walker, with pain.
Figure 1.

X-ray showing anterior dislocation of the right hip.
Investigations
x-Ray revealed an anterior hip dislocation, and an MRI (figures 2) confirmed avascular necrosis with collapse of the dislocated femoral head.
Figure 2.
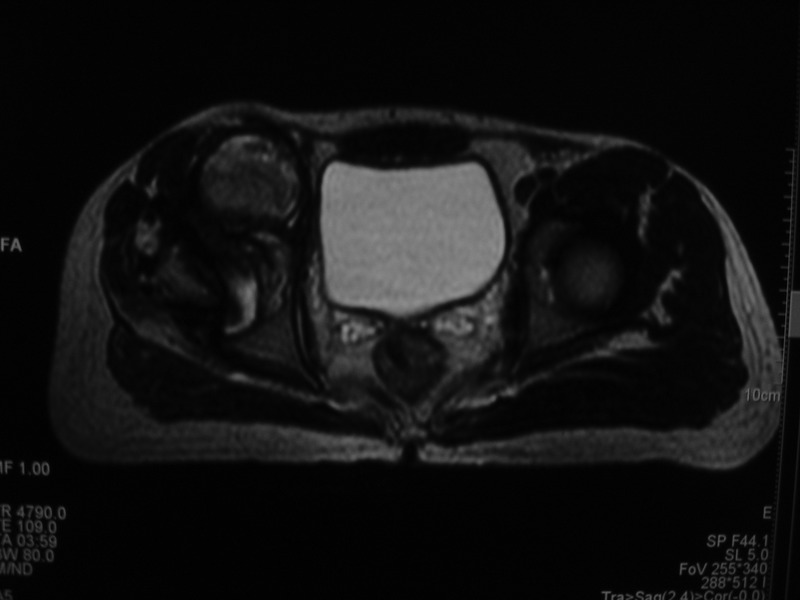
MRI image showing avascular necrosis of the dislocated head of femur.
Treatment
A modified girdlestone arthroplasty (modified by Nagi et al)2 was performed. An anterolateral approach was used by the surgeon. The superior aspect of the capsule was found to be damaged with an intact anterior portion. The anterosuperior aspect of the head showed collapse and articular damage. A subcapital osteotomy was performed, leaving behind majority of the femoral neck which was then displaced into the acetabulum. Postoperative skeletal traction of 5 kg was maintained for 6 weeks. Physiotherapy was started 10 days after surgery and gradual weight bearing at 10 weeks.
Outcome and follow-up
At 36 months postsurgery, the patient has a satisfactory range of motion and a fairly stable hip (figure 3) with 120 degrees of flexion and 30 degrees of internal and external rotation. 2.5 cm limb shortening, restriction of terminal 15°s of abduction and Trendelenburg gait is present. He uses a 2.5 cm shoe raise and is able to walk independently outdoors and is active again as a farmer.
Figure 3.
36 months postoperative x-ray.
Discussion
Old unreduced anterior dislocation of the hip is a rare entity. If the delay is greater than 3 months, open reduction ceases to be a viable option. Surgical treatment options include total hip arthroplasty, modified girdlestone procedure (by Nagi) and trochanteric osteotomy. Persisting pain, trendelenbergs gait, fixed flexion deformity and shortening have been noted following surgical treatment reported in the past.2–6
Although total hip arthroplasty is currently a good option, previously described treatment methods like trochanteric osteotomy and modified girdlestone may be relevant in situations where expert care may be unavailable or when a sedentary patient may wish to undergo total hip arthroplasty at a later date. In the case described above, since the femoral neck is intact, a total hip arthroplasty may be performed easily in future should the patient develop any pain.
Learning points.
Neglected dislocation of hip can present in a rural setting.
An MRI can be used to ascertain viability of the femoral head in such a situation.
Where joint replacement surgery may not be feasible modified girdlestone procedure may be utilised with good results.
Footnotes
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Thompson VP, Epstein HC. Traumatic dislocation of the hip. J Bone Joint Surg 1951;33-A:746. [PubMed] [Google Scholar]
- 2.Nagi ON, Dhillon MS, Gill SS. Chronically unreduced traumatic anterior dislocation of the hip. A report of four cases. J Ortho Trauma 1992;6:433–6 [DOI] [PubMed] [Google Scholar]
- 3.Aggarwal ND, Singh H. Unreduced anterior dislocation of the hip. A report of 7 cases. J Bone Joint Surg (Br) 1967;49:288–92 [PubMed] [Google Scholar]
- 4.Hamada G. Unreduced anterior dislocation of the hip. J Bone Joint Surg (Am) 1957;39:471–6 [DOI] [PubMed] [Google Scholar]
- 5.Rai J, Singal V, Saikia K. Neglected unusual obturator dislocation of the hip (a case report). Int J Surg 1983;45:363–5 [Google Scholar]
- 6.Scadden WJ, Dennyson WG. Unreduced obturator dislocation of the hip. A case report. S Afr Med J 1978;53:601–2 [PubMed] [Google Scholar]