

Abstract
Background:
Limited data are available indicating associates of stunting among Iranian children. This study was conducted to investigate determinants of stunting in first grade primary school children of Tehran in 2007.
Method:
In this case-control study, 3147 school children were selected by multistage cluster random sampling method from 5 districts of Tehran. Anthropometric measurements were done and stunting was defined as height for age less than the 5th percentile of CDC2000 cut-off points. Eighty six stunted children were identified and considered as case group. After matching for age, sex and residence area, 308 non-stunted children were randomly selected as control group. Required data were collected by trained nutritionists using questionnaires.
Results:
Stunting was prevalent among 3.7% of the study population (girls 4.4% vs. boys 2.8%, P < 0.05). Mean age of the studied children was 82.3 month. Children with a birth weight of >3000 g were less likely to be stunted (OR: 0.25: 95% CI: 0.11-0.54) compared with those with a birth weight of <3000 g. Being born to older mothers (>35 years) was associated with greater odds of being stunted (3.01; 1.19-7.60) compared with being born to younger mothers (<35 years). Those with fathers’ height of >160 cm were less likely to be stunted (0.04; 0.005-0.37) than those whose fathers’ height was less than 160 cm.
Conclusions:
We found that birth weight, maternal age and fathers’ height are the major contributing factors to stunting in this group of Iranian children. Taking into account the determinants of stunting might help policy makers designing appropriate interventions.
Keywords: Birth weight, breast feeding, children, stunting
INTRODUCTION
Linear growth retardation, or stunting, which is a manifestation of chronic malnutrition, is highly prevalent in under-developed and developing countries.[1–4] According to the World Health Organization, 215 million children were stunted in 2000 throughout the world. The national data from “Iranian National Study of Malnutrition Prevalence” in 2005 has indicated that 4.7% of Iranian children are affected by stunting.[5] Earlier studies have shown that child's stunting is associated with concurrent, and possibly later, delayed mental and motor development.[6,7] The adverse effects of stunting could affect the adulthood by limiting work capacity owing to reduced muscle mass[8] and increasing obstetric risks in women.[9]
Height is influenced by genetic, socioeconomic, and dietary factors.[1] Although, several studies have identified determinants of stunting in different populations,[5,10–15] limited data are available indicating its associates among Iranian children. Earlier studies have identified low birth weight, inadequate child care, feeding practice and birth order as a probable correlates of stunting[16,17] #94; Wamani, 2007 #82). It also has been shown that birth weight, breast feeding status, mothers’ age, family size, socio-economic status and birth order are associated with a higher prevalence of stunting among Iranian children.[5,18–22] Previous studies have been limited in sample size[20,22,23] and their sampling procedure;[18,19,21] such that their findings cannot be easily extrapolated to other parts of the country. Furthermore, most have reported the prevalence of stunting, not its determinants.[5,10,24,25] It remains unknown if the determinants of stunting in a metropolitan area like Tehran are different from those in deprived regions of the country. This study was, therefore, conducted to investigate determinants of stunting in first grade primary school children of Tehran.
METHODS
Participants
In this case-control study, participants were selected by multistage cluster random sampling method from 5 districts of Tehran in 2007. (Northern, Southern, Western, Eastern and central parts). First, 42 public schools (19 schools for girls and 23 for boys) were randomly selected based on proportional to size method in each district. In each selected school, all first grade pupils aged 7 years old were invited to participate in the study (n = 3147, 1343 boys and 1804 girls). Stunting was defined as height for age less than the 5th percentile of CDC2000 cut-off points.[1] Based on this definition, 86 stunted children were identified and considered as case group in the current study. After matching for age, sex and residence area, 308 non-stunted children (height for age more than the 5th percentile of CDC2000 cut-off points) were randomly selected as control group. The study was approved ethically by Research Ethics Committee of National Nutrition and Food Technology Research Institute, Tehran, Iran and all participants provided informed written consent forms.
Data collection
Required data about children's birth weight and height, duration of breastfeeding and family demographic characteristics (including family size, parity, parents’ job, parents;’ education, marital status, mothers’ age, and home ownership) were collected by trained nutritionists using questionnaires. Anthropometric measurements were done in all participants by two trained nutritionists and were randomly re-checked by a senior investigator (FE). Weight was measured by means of a portable calibrated digital scale (Breuer, Germany) to the nearest 0.1 kg in light clothing without shoes. Height was measured according to a standard protocol to the nearest 0.1 cm using Height Measure (Seca 214, Germany). Body mass index was calculated afterwards. Mothers’ weight and height were measured by standard methods[26] and fathers’ weight and height were collected through self-reporting.
Statistical analysis
Data were analyzed using statistical package for social science (SPSS Inc, version 14). To ensure normal distribution of variables, Kolmogrov-Smirnov test was applied. Continuous variables were compared using independent samples t-test between stunted and non-stunted children. Distribution of participants in terms of categorical variables was examined through the use of Chi-square test. Multivariate logistic regression analysis was applied to identify the determinants of stunting. In these analyses, first the continuous variables were entered into the models and then these variables were treated as categorical variables. P <0.05 was considered as statistically significant.
RESULTS
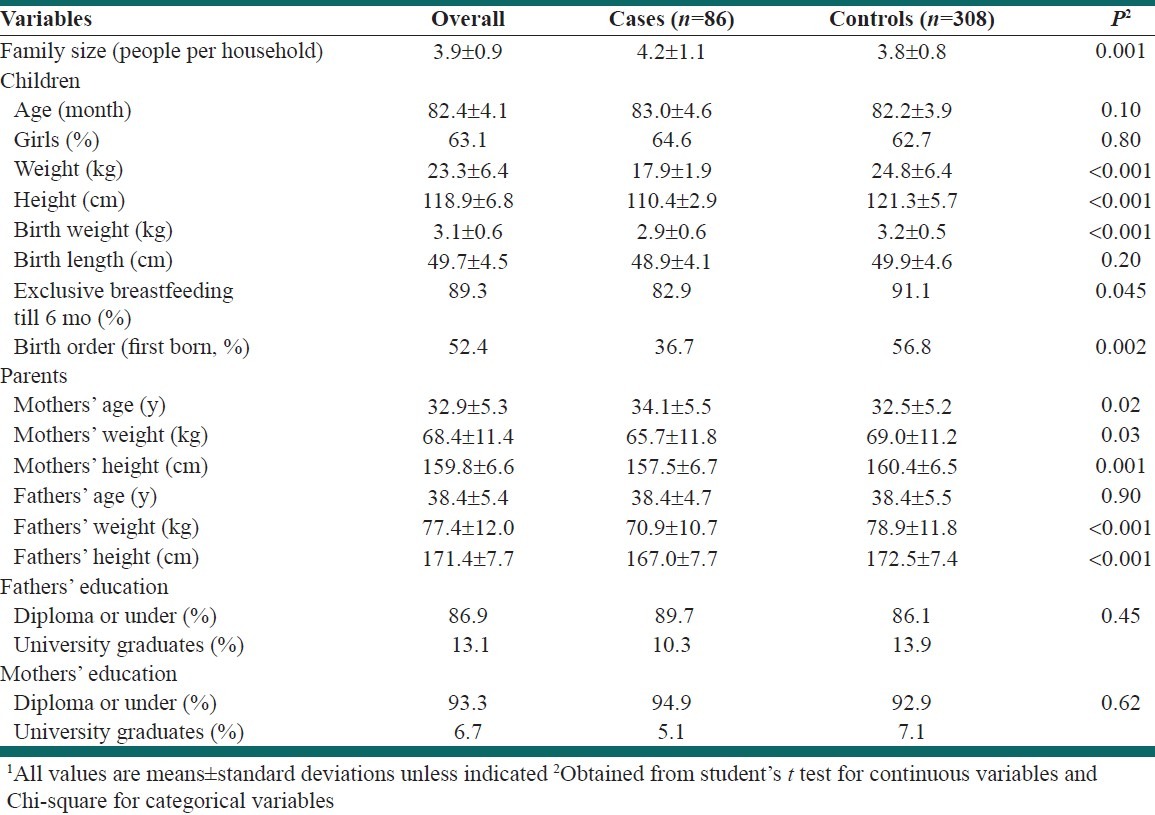
Stunting was prevalent among 3.7% of the studied population (n = 3147). It was more prevalent in girls (4.4%) than boys (2.8%, P < 0.05). Characteristics of the studied population are provided in Table 1. Mean age of the studied children was 82.3 month with no significant difference between cases and controls. Stunted children were more likely to be thin compared with non-stunted children (weight: 17.9 ± 1.8 vs. 24.8 ± 6.3, P < 0.001). Mean birth weight (2860 ± 570 vs. 3230 ± 530 g, P < 0.001) was also lower in stunted children than non-stunted counterparts; however, their mean birth length was not significantly different (48.9 ± 4.0 vs. 49.8 ± 4.6 cm, P = 0.19). Stunted children were less likely to be exclusively breastfed for the first 6 months of their life (83% vs. 91%, P = 0.045) and less likely to be first born in terms of birth order (36.7 vs. 56.8%, P = 0.002) compared with non-stunted children. They were born to older mothers and to parents with lower weight and height than non-stunted children. Most stunted children were from families with more than 4 people per household. No significant differences were found between cases and controls in terms of parental education.
Table 1.
Characteristics of the study participants1
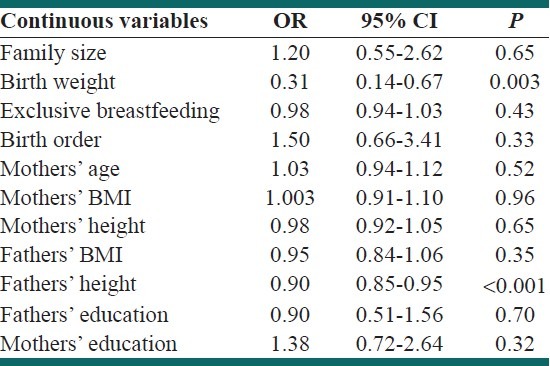
Multivariate adjusted odds ratios of stunting for different contributing factors are presented in Table 2. All variables in these models were treated as continuous. It has been found that birth weight (odds ratio: 0.31; 95% CI: 0.14-0.66) and fathers’ height (odds ratio: 0.89; 95% CI: 0.84-0.95) were protectively associated with stunting. No significant associations were seen between other factors and stunting when these factors were treated as continuous variables.
Table 2.
Determinants (continuous variables) of stunting among school-aged children
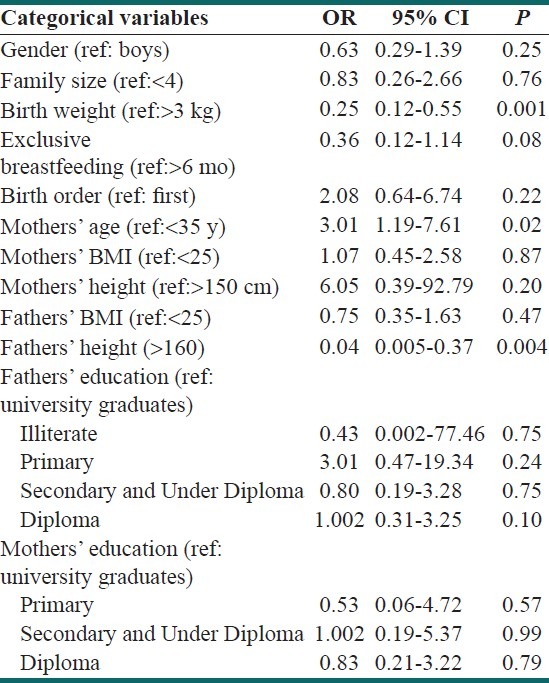
When the variables were treated as categorical [Table 3], we found that children with a birth weight of >3000 g were less likely to be stunted (OR: 0.25: 95% CI: 0.11-0.54) compared with those with a birth weight of <3000 g. Being born to older mothers (>35 years) was associated with greater odds of being stunted (3.01; 1.19-7.60) compared with being born to younger mothers (<35 years). Those with a fathers’ height of >160 cm were less likely to be stunted (0.04; 0.005-0.37) than those whose fathers’ height was less than 160 cm. No overall significant associations were found between stunting and other factors.
Table 3.
Determinants (categorical variables) of stunting among school-aged children
DISCUSSSION
In this study, we found that the prevalence of stunting was 3.7%. Birth weight, fathers’ height and maternal age were the main contributing factors to stunting in the studied population.
The prevalence of stunting in this study was in agreement with the one reported by National Study of Malnutrition Prevalence in Iranian children. It seems that the prevalence of stunting has been decreased in the past decade in the country. The decreasing trend of stunting has been reported in South East Asia, where the stunting has reduced in elementary school children from 52.4%in 1998 to 32.8% in 2000.[27] Worldwide stunting prevalence has also decreased from 48.8% in 1980 to 39.9% in 1995.[28,29] This can be explained by improved primary health care during pregnancy and early childhood, breastfeeding and growth monitoring.
In this study, the prevalence of low birth weight and short duration of breastfeeding (<6 mo) was higher in cases than that in controls. The same findings have been reached by Lwambo et al.,[30] Marshall et al.[31] and Ricci et al.[13] Low birth weight infants have inadequate nutrient stores required for height growth. Due to increased requirements in these infants, additional amounts of nutrients are needed for these babies to reach normal height growth.[32] Findings of the current study about breastfeeding are in agreement with those of Marquis et al., in Peru[33] and Semba et al., in Indonesia and Bangladesh which indicated that short duration of breastfeeding was positively related to prevalence of stunting. Short duration of breastfeeding would prohibit adequate dietary intakes of energy, protein and micronutrients required for normal height growth.[34]
Low birth weight was found as a contributing factor to stunting in this study. This finding is in line with earlier studies among Brazilian,[35] Mexican[36] and Pakistani children.[37] Birth weight has also been reported as a strong predictor of child size in later life among children with Intra-Uterine Growth Retardation (IUGR). Most IUGR infants do not catch-up to normal size during childhood. Low birth weight and subsequent stunting could be induced by maternal under-nutrition during pregnancy. In the current study, we did not collect data about dietary intakes of mothers during their pregnancy. Adequate nutrition during pregnancy would result in increased birth weight and in turn would improve child growth in later life.
Another determinant of stunting in the current study was maternal age. This finding is in agreement with previously reported ones. In Egypt, children born to mothers aged ≥35 years showed a higher prevalence of stunting than children born to mothers in other age groups.[15] Maternal age has also been reported as a determinant factor of stunting in South African children.[38] The effect of the age of the mother on child health outcomes has also been explored in several studies.[39,40] In the case of India, Raj et al., showed that children born to mothers who were married below the age of 18 were at a higher risk of stunting and underweight compared to children of women who had married at age 18 or older. Although, several studies have reported the importance of mothers’ young age at pregnancy on health outcomes of children, limited data have focused on older age. The current findings highlight the importance of old age of mothers as a contributing factor to stunting.[41]
As we all know socioeconomic status and dietary intakes are two important contributing factors to stunting.[42] We tried to collect data on economical status of the households; however, after completion of the study, we found that these data are not reliable. So, we used educational status of parents as a proxy of socioeconomic status. One might suggest the use of living district as a proxy of socioeconomic status. In the current study, when we explored the frequency of stunting in different districts of Tehran (5 districts were selected in this study), we failed to find a significant difference. Due to the inclusion of children from different socioeconomic status in the current study, the findings can easily be extrapolated to the Tehrani children, however, more caution are required about the generalizability of the findings to the whole country.
CONCLUSIONS
We found that birth weight, maternal age and fathers’ height are the major contributing factors to stunting in this group of Iranian children. Stunting, an irreversible situation, is an important index of chronic malnutrition. Therefore fetal, infant and child growth monitoring is necessary to prevent stunting. Furthermore, taking into account the determinants of stunting might help policy makers designing appropriate interventions.
ACKNOWLEDGEMENTS
The authors would like to appreciate the Research Council of National Nutrition and Food Technology Research Institute, Faculty of Nutrition Science and Food Technology, Shahid Beheshti University of Medical Sciences for financial support of this study.
In addition, we would like to thank all school deans, teachers, students and their parents for their valuable support in conducting this study. Also, we thank Seyedeh Marjan Khalafi and Maliheh Zahedi Rad for their technical help.
Footnotes
Source of Support: National Nutrition and Food Technology Research Institute, Faculty of Nutrition Science and Food Technology, Shahid Beheshti University of Medical Sciences (Grant No: 3572)
Conflict of Interest: None declared
REFERENCES
- 1.Ibrahim SA, Abd el-Maksoud A, Nassar MF. Nutrition stunting in Egypt: Which nutrient is responsible? East Mediterr Health J. 2002;8:272–80. [PubMed] [Google Scholar]
- 2.Kiliç I, Özalp I, Coskun T, Tokatli A, Emre S, Saldamli I, et al. The effect of zinc-supplemented bread consumption on school children with asymptomatic zinc deficiency. J Pediatr Gastroenterol Nutr. 1998;26:167–71. doi: 10.1097/00005176-199802000-00008. [DOI] [PubMed] [Google Scholar]
- 3.Ninh NX, Thissen JP, Collette L, Gerard G, Khoi HH, Ketelslegers JM. Zinc supplementation increases growth and circulating insulin- like growth factor 1 (IGF-1) IN growth- related Vietnamese children. Am J Clin Nutr. 1996;63:514–9. doi: 10.1093/ajcn/63.4.514. [DOI] [PubMed] [Google Scholar]
- 4.Rosado JL, López P, Muñoz E, Martinez H, Allen LH. Zinc supplementation reduced morbidity, but neither zinc nor iron supplementation affected growth or body composition of Mexican preschoolers. Am J Clin Nutr. 1997;65:13–9. doi: 10.1093/ajcn/65.1.13. [DOI] [PubMed] [Google Scholar]
- 5.Sheikholeslam R, Naghavi M, Abdollahi Z, Zarati M, Vaseghi S, SadeghiGhotbabadi F. Current status and trends in the 10-years indices of malnutrition in children under 5 years. Iran J Epidemiol. 2008;4:21–8. [Google Scholar]
- 6.Mendez MA, Adair LS. Severity and timing of stunting in the first two years of life affect performance on cognitive tests in late childhood. J Nutr. 1999;129:1555–62. doi: 10.1093/jn/129.8.1555. [DOI] [PubMed] [Google Scholar]
- 7.Ong LC, Chandran V, Lim YY, Chen AH, Poh BK. Factors associated with poor academic achievement among urban primary school children in Malaysia. Singapore Med J. 2010;51:247–52. [PubMed] [Google Scholar]
- 8.Haas JD, Murdoch S, Rivera J, Martorell R. Early nutrition and later physical work capacity. Nutr Rev. 1996;54(2 Pt 2):S41–8. doi: 10.1111/j.1753-4887.1996.tb03869.x. [DOI] [PubMed] [Google Scholar]
- 9.Martorell R, Rivera J, Kaplowitz H, Pollitt E. Long-term consequences of growth retardation during early childhood. In: Hernandez M, Argente J, editors. Human Growth: Basic and clinical aspects. Amsterdam: Elsevier Science; 1992. pp. 143–8. [Google Scholar]
- 10.Houshyarrad A, Dorosti Motlagh A, Kalantari N, Abtahi M. Prevalence of stunting, underweight, wasting and overweight among iranian under-five-year-old children (2000-2002) Iran J Nutr Sci. 2009;4:49–56. [Google Scholar]
- 11.Kanao B, Abu-Nada O, Zabut B. Nutritional status correlated with sociodemographic and economic factors among preparatory school-aged children in the Gaza Strip. J Public Health. 2009;17:113–9. [Google Scholar]
- 12.Khuwaja S, Selwyn BJ, Shah SM. Prevalence and correlates of stunting among primary school children in rural areas of southern Pakistan. J Trop Pediatr. 2005;51:72–7. doi: 10.1093/tropej/fmh067. [DOI] [PubMed] [Google Scholar]
- 13.Ricci JA, Becker S. Risk factors for wasting and stunting among children in Metro Cebu, Philippines. Am J Clin Nutr. 1996;63:966–75. doi: 10.1093/ajcn/63.6.966. [DOI] [PubMed] [Google Scholar]
- 14.Wamani H, Åstrøm AN, Peterson S, Tumwine JK, Tylleskär T. Boys are more stunted than girls in sub-Saharan Africa: A meta-analysis of 16 demographic and health surveys. BMC Pediatr. 2007;7:17–26. doi: 10.1186/1471-2431-7-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zottarelli LK, Sunil TS, Rajaram S. Influence of parental and socioeconomic factors on stunting in children under 5 years in Egypt. East Mediterr Health J. 2007;13:1330–42. doi: 10.26719/2007.13.6.1330. [DOI] [PubMed] [Google Scholar]
- 16.Onis M, Frongillo EA, Blössner M. Is malnutrition declining. An analysis of changes in levels of child malnutrition since 1980? Bull World Health Organ. 2000;78:1222–33. [PMC free article] [PubMed] [Google Scholar]
- 17.Ali SS, Balaji P, Goudar SS, Dhaded S. A Cross sectional study to assess the impact of nutrition on child development at three years in a rural community of India. Int J Prev Med. 2012 [In press] [PMC free article] [PubMed] [Google Scholar]
- 18.Ansari H, Nourouzi M, Falah S, Lotfi MB. Predictors of malnutrition among zahedans's children, age ranging from 2-5 years old in 2007-2008. Shahrekord Univ Med Sci J. 2009;11:46–54. [Google Scholar]
- 19.Lakeh MM, Bahreini S. Stunting Trends in under 6 year old children living in rural area of Robat-Karim from 1997 to 2007: An Age-Period-Cohort effect analysis. Iran J Epidemiol. 2009;5:27–34. [Google Scholar]
- 20.Mahyar A, Ayazi P, Fallahi M, Javadi TH, Farkhondehmehr B, Javadi A, et al. Prevalence of Underweight, stunting and wasting among children in Qazvin, Iran. Iran J Pediatr Soc. 2010;2:37–43. [Google Scholar]
- 21.Taheri F, Fesharakinia A, Joe AS. The prevalence of underweight, wasting and stunting in 6-12 years old children of Birjand. J Birjand Univ Med Sci. 2001;8:22–7. [Google Scholar]
- 22.Ziaei Kajbaf T, Taheri M, Razapour A. Prevalence of short stature among first year primary school students in Ahvaz in year 2003. Sci Med J. 2007;6:39–45. [Google Scholar]
- 23.Najm-Abadi S. Risk analysis of growth failure in under-5-year children. Arch Iran Med. 2004;7:195–200. [Google Scholar]
- 24.Fesharakinia A, Sharifzadeh GR, Zarban A. Investigation of nutritional status in elementary school students of South Khorasan Province: East of Iran. Qom Univ Med Sci J. 2008;2:47–52. [Google Scholar]
- 25.Veghari G, Asadi J, Eshghinia S. Impact of ethnicity upon body composition assessment in Iranian Northern children. J Clin Diagn Res. 2009;3:1779–83. [Google Scholar]
- 26.WHO Expert Commitee. WHO Technical Report Series 854. Vol. 854. Geneva: World Health Organ Tech Rep Ser; 1995. Physical status: The use and interpretation of anthropometry; pp. 1–452. [PubMed] [Google Scholar]
- 27.De Onis M, Blössner M. The World Health Organization global database on child growth and malnutritin: Methodology and applications. Int J Epidemiol. 2003;32:518–26. doi: 10.1093/ije/dyg099. [DOI] [PubMed] [Google Scholar]
- 28. [Last accessed on 2012 Jan 25]. Available from: http://www.unsystem.org/SCN/archives/rwns03/CH05.htm .
- 29.Abtahi M, Doustmohammadian A, Abbdollahi M. construction of national standards of weight and height and growth charts of iranian children: A review article. Int J Prev Med. 2011;2:122–6. [PMC free article] [PubMed] [Google Scholar]
- 30.Lwambo NJ, Brooker S, Siza JE, Bundy DA, Guyatt H. Age patterns in stunting and anaemia in African school children: A cross-sectional study in Tanzania. Eur J Clin Nutr. 2000;54:36–40. doi: 10.1038/sj.ejcn.1600890. [DOI] [PubMed] [Google Scholar]
- 31.Marshall WA, Tanner JM. Variations in the pattern of pubertal changes in boys. Arch Dis Child. 1970;45:13–23. doi: 10.1136/adc.45.239.13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Eric M. Nutrition during Pregnancy and Lactation. In: Mahan LK, Scott Stump S, editors. Krause's Food and Nutrition Therapy. St. Louis, Missouri: Saunders, Elsevier Inc; 2008. pp. 160–98. [Google Scholar]
- 33.Marquis GS, Habicht JP, Flanata CF, Black RE, Rasumussen KM. Association of Breastfeeding and Stunting in peruvian toddlers: An example of reverse Causality. Int J Epidemiol. 1997;26:349–56. doi: 10.1093/ije/26.2.349. [DOI] [PubMed] [Google Scholar]
- 34.Semba RD, de Pee S, Sun K, Sari M, Akhter N, Bloem MW. Effect of parental formal education on risk of child stunting in Indonesia and Bangladesh: A cross-sectional study. The Lancet. 2008;371:322–8. doi: 10.1016/S0140-6736(08)60169-5. [DOI] [PubMed] [Google Scholar]
- 35.Menezes RC, Lira PI, Leal VS, Oliveira JS, Santana SC, Sequeira LA, et al. Determinants of stunting in children under five in Pernambuco, Northeastern Brazil. Rev Saúe Pública. 2011;45:1079–87. doi: 10.1590/s0034-89102011000600010. [DOI] [PubMed] [Google Scholar]
- 36.Varela-Silva MI, Azcorra H, Dickinson F, Bogin B, Frisancho AR. Influence of maternal stature, pregnancy age, and infant birth weight on growth during childhood in Yucatan, Mexico: A test of the intergenerational effects hypothesis. Am J Hum Biol. 2009;21:657–63. doi: 10.1002/ajhb.20883. [DOI] [PubMed] [Google Scholar]
- 37.Saleemi MA, Ashraf RN, Mellander L, Zaman S. Determinants of stunting at 6, 12, 24 and 60 months and postnatal linear growth in Pakistani children. Acta Paediatr. 2001;90:1304–8. doi: 10.1080/080352501317130371. [DOI] [PubMed] [Google Scholar]
- 38.Kimani-Murage EW, Norris SA, Pettifor JM, Tollman SM, Klipstein-Grobusch K, Gómez-Olivé XF, et al. Nutritional status and HIV in rural South African children. BMC Pediatr. 2011;11:23. doi: 10.1186/1471-2431-11-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Finlay JE, Özaltin E, Canning D. The association of maternal age with infant mortality, child anthropometric failure, diarrhoea and anaemia for first births: Evidence from 55 low-and middle-income countries. BMJ Open. 2011;1:1–24. doi: 10.1136/bmjopen-2011-000226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Vitolo MR, Gama CM, Bortolini GA, Campagnolo PD, Drachler Mde L. Some risk factors associated with overweight, stunting and wasting among children under 5 years old. J Pediatr (Rio J) 2008;84:251–7. doi: 10.2223/JPED.1776. [DOI] [PubMed] [Google Scholar]
- 41.Raj A, Saggurti N, Winter M, Labonte A, Decker MR, Balaiah D, et al. The effect of maternal child marriage on morbidity and mortality of children under 5 in India: Cross sectional study of a nationally representative sample. BMJ. 2010;340:b4258. doi: 10.1136/bmj.b4258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Esfarjani F, Hajifaraji M, Roustaee R, Mohammadi-Nasrabadi F, Zowghi T. Schools’ Cafeteria Status: Does it affect snack patterns? A qualitative study. Int J Prev Med. 2012 [In press] [PMC free article] [PubMed] [Google Scholar]