

Abstract
Objective:
This study compares the Center for Disease Control (CDC) and International Obesity Task Force (IOTF) references in assessment of overweight and obesity among Iranian adolescents.
Methods:
The data of this study was drawn from a cross sectional study of a representative sample of 1200 adolescents aged 12-17 years in Babol, northern Iran. A standard procedure was used to measure height and weight and the body mass index was calculated. Each subject was classified as overweight and obese based on IOTF cut off values of BMI and CDC references BMI percentile sets by age and sex. The kappa coefficients were estimated for the degree of agreement.
Results:
In assessment of obesity/overweight prevalence, the CDC and IOTF references produced a similar estimate by age group and sex. The maximum differences was about 1% and the kappa coefficients was 0.96 to 1 (P = 0.001). While for assessment of obesity, the CDC reference produced slightly a higher rate of obesity and the difference in prevalence between the two sets of references was ranged from 1.4% to 3.2% with kappa coefficients: 0.90 to 0.70 (P = 0.001) depending on the age group and sex and a greater difference was observed among younger age group.
Conclusion:
The findings suggest an excellent agreement between the TOTF and CDC references in assessment of overall overweight/obesity prevalence among adolescent boys and girls. While in assessment of obesity prevalence alone the degree of agreement between the two sets of references slightly diminished. Overall, the two references are comparable and the agreement varies a little with respect to age and sex.
Keywords: Adolescents, Babol, center for disease control, international obesity task force, obesity, overweight
INTRODUCTION
During the two recent decades, high prevalence rates of overweight and obesity particularly among children and adolescents have become a concern in both the developed and the developing countries.[1–4] Nevertheless, the prevalence of obesity in children is increasing worldwide. The evidence from the United States suggests that this upward trend has continued into the 21st century.[5] Obesity in children is a major public health challenge and greater burden during the future years and it is associated with numerous short and long term health hazards including the higher prevalence of metabolic syndrome and cardiovascular diseases resulting from lifestyles changes.[6–16]
Body mass index (BMI) is widely used to classify obesity in children and adolescents and it is closely related to body fat and long term health hazard outcome.[17,18] However, there is need to use a classification system which can define obesity in children and to provide a consistent assessment of obesity across life span.[19] In the diagnosis of adulthood obesity and overweight, a general consensus exists based on WHO criteria that were defined for overweight and obesity with cutoff value of body mass index of 25 and 30 respectively for both sexes that has been widely used.[20] These cutoff values are the best indicator of health hazard outcome in adulthood. While for the children and adolescent, BMI is widely changed by age and sex . Thus, these cutoff values can not be considered for definition of obesity in children. Most previous studies used different definitions of child and adolescent obesity and there is no global agreement to use them in different countries. With this regard, at least three different definitions for child and adolescent overweight and obesity have been proposed. First, it was the WHO criteria that use BMI for adolescents and weight for height Z-score for children.[21] The second was the criteria of Center for Disease Control and prevention (CDC 2000) that produced the sets of percentiles of BMI by age and sex specific in the United States for children and adolescents aged 2-18 years.[22] Third, the cut off values of BMI by age and sex have been produced recently by the International Obesity Task Force (IOTF) that has passed the adult cut off values at age of 18.[23] The CDC and IOTF criteria are the most commonly used in diagnosis of obesity and overweight among the children and adolescent aged 2-18 years.[24] In previous studies, although there is an overall consensus between these two criteria, the discrepancy with regard to age, gender and country is noticeable.[24] This discrepancy makes the estimated prevalence rates of overweight and obesity become non-comparable across the different studies all over the world.
Although, a marked increase in the prevalence of overweight and obesity have been reported among the Iranian children and adolescents,[25–27] but the results of the studies are not consistent. Discordant in obesity prevalence may be attributed to the different criteria used for defining overweight and obesity. There are no data to compare the ability of CDC and IOTF criteria in estimating obesity among the Iranian youth and adolescent. Thus, the objective of this study was to compare the prevalence of overweight and obesity in Iranian children and adolescents by using IOTF and CDC references, and to explore their discrepancy in accordance with age and sex.
METHODS
The data of this study was drawn from a cross sectional study of 1200 representative random sample of youth of 20 elementary schools and 20 high schools performed in 2008 in Babol, a geographic area located in the northern Iran. This allocated sample size allows estimating the rate of obesity/overweight in which, with presumption of prevalence of 15%, the maximum marginal error would not be exceeded more than 0.03 with 95% confidence level. Using a cluster sampling technique, 600 boys and 600 girls aged 12-18 years were recruited randomly in the study and all selected samples included in the study with no refusal rate. The details of description of sampling technique were described elsewhere.[28] A standardized protocol was used to measure height and weight and for interview as well. Body weight was assessed by using a digital scale of Seca while the subjects stood in light clothing with no shoes. Standing height was measured without shows using a portable stadiometer. The body mass index (BMI) was calculated by weight in kg divided by square of height in m2.
CDC references percentiles: The new growth charts for percentiles of BMI from the US Center for Disease Control (CDC) and Prevention with age and sex specific percentile reference values have been provided as screening tools of overweight and obesity among children and adolescents aged 2-18 years in 2000.[22] In this study, the diagnosis of obesity and overweight in children and adolescents were assessed by comparing BMI of the subject under study with CDC reference sets of percentiles of BMI index for age and sex.
International obesity task force reference
The International Obesity Task Force (IOTF) has also provided as international reference for sex and age specific values of BMI cut off for classification of overweight and obesity among children and adolescent aged 2-18 years.[23] These proposed cut off values of BMI for diagnosis of overweight and obesity in children and adolescents is linked with adult cut off values of 25 and 30 for risk of overweight and obesity respectively at age 18 years for adolescents. The IOTF criteria have been justified internationally using dataset specific percentiles linked to adult cut off points.[23,24] It is based on the large data sets from six countries including Brazil, Britain, Hong Kong, the Netherland, Singapore and the USA. We also used the IOTF cut off values of BMI for diagnosis of overweight and obesity by age and sex.
Statistical analysis
In statistical analysis, we used SPSS software version 16.0. First, each subject was classified as overweight or obese by comparing his/her BMI with CDC percentiles for age and sex. The BMI within 85th and 95th CDC percentiles were considered as overweight and >95th percentile as obese. Second, similarly, each subject was classified as overweight and obese based on IOTF cut off values of BMI for age and sex. We also categorized the participants in two age groups of 12-14 years and 15-17 years. The prevalence of overweight and obesity using the two CDC and IOTF references was determined in each age group and compared with respect to age. We determine the rate of agreement of the two criteria for estimating obesity alone, as well as obesity/overweight by calculation of kappa statistics that measures the agreement in individual levels by calculating kappa = (Po-Pe)/(1-Pe) where Po = the observed probability of agreement and Pe = the probability of expected agreement by chance. Kappa statistics becomes to 0 when the observed agreement is equal to expected agreement and 1 when the agreement is perfect. The McNemar Chi-square test was used to evaluate the degree of agreement between two criteria and the P value less than 0.05 were considered as significant level.
RESULTS
The mean of age, height, weight and BMI of study sample are presented by sex in Table 1. The corresponding values for mean (SD) age for adolescent boys and girls were 14.3 (1.7), 14.2 (1.6) years respectively. The boys had significantly higher body weight, and higher height but identical BMI compared with girls of similar age group.
Table 1.
The mean (SD) of different characteristics of adolescents with respect to sex in elementary and high schools of Babol (2008)
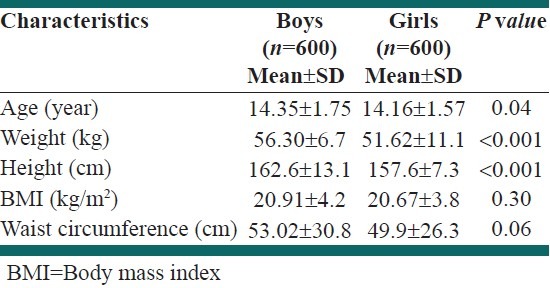
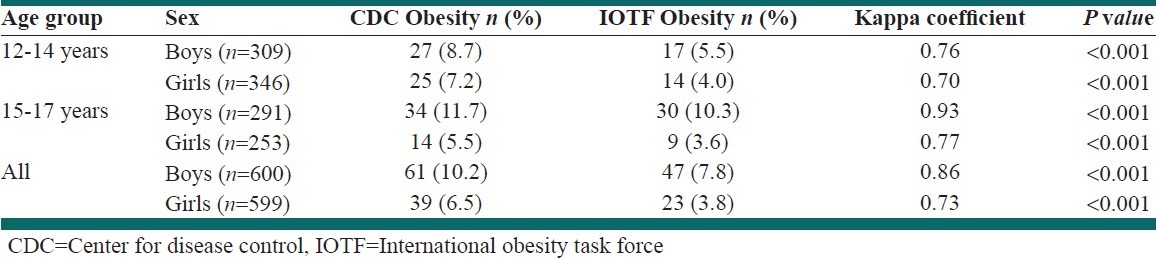
Table 2 shows that both CDC and IOTF references have demonstrated a similar estimate of overweight/obesity prevalence among adolescent irrespective to age and sex. There was an excellent agreement with a high degree of agreement by kappa coefficients were ranged from 0.97 to 1 (P = 0.001). A complete agreement (kappa = 1) was observed among adolescent boys in age group of 12-14 years. The overall agreement coefficient of kappa was 0.79 and 0.96 for boys and girls respectively indicating a similar ability in estimating overweight/obesity prevalence by the two sets of references. Table 3 compares the prevalence of obesity by CDC and IOTF criteria by age and sex group. The CDC reference recognized higher rate of obesity than IOTF across both age and sex group. The differences (CDC-IOTF) ranged from 1.4% to 3.2%. In age group of 12-15 year old children, the prevalence rate of obesity in both sexes was 3.2% higher by CDC reference compared with IOTF. In older age group of 15-17 year, also CDC was more sensitive than IOTF in the diagnosis of obesity with prevalence rates of obesity at 11.7%; 10.3% in boys compared with 5.5% and 3.6% in girls. The respective differences in prevalence rates of obesity were 1.4% and 1.9% in boys and girls indicating slightly higher sensitivity of CDC for diagnosis of obesity in older girls. The kappa coefficients for the least and the highest agreement between the two sets of references for diagnosis of obesity ranged from 0.70 to 0.93, (P = 0.001). Overall, CDC reference was more sensitive than IOTF in estimating obesity and there was a higher agreement between the two references in recognizing obesity in boys than in girls (kappa = 0.86 versus 0.73).
Table 2.
The prevalence of overweight/obesity according to center for disease control and international obesity task force references in adolescents with respect age group and sex and the kappa coefficients in elementary and high schools of Babol (2008)
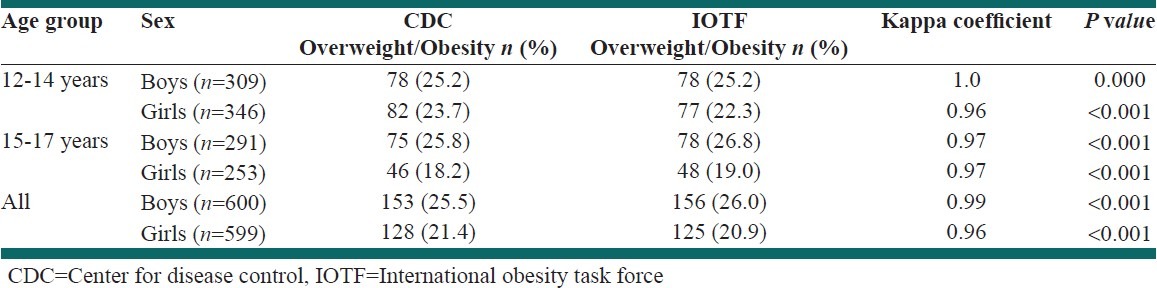
Table 3.
The prevalence of obesity according to center for disease control and international obesity task force references in adolescents with respect age group and sex and the kappa coefficients in elementary and high schools of Babol (2008)
DISCUSSION
This study which evaluated the ability of CDC and IOTF references for estimating obesity and obesity/overweight in children demonstrated that CDC reference was more sensitive than IOTF in estimating obesity in both boys and girls particularly in the age group of 12-14 years old. In this study, the estimate of obesity prevalence rate in the age group of 12-14 years using CDC was higher than IOTF reference by 3.2 percentage points in both boys and girls. Similarly, the estimates of obesity prevalence rate in older age group of 15-17 years old was also greater using CDC compared with IOTF in both boys and girls. However, the absolute difference in estimates of obesity in this age group was different between the two sexes with slightly greater in the girls than the boys by 1.9 and 1.4 percentage points, respectively. The sensitivity of CDC and IOTF criteria in estimating obesity varies by increasing age across sexes. Both, criteria yielded a lower estimate of obesity among girls by age. This difference may be partially explained by the difference in age of onset of puberty between the two sexes. Nevertheless, the values for kappa suggest a good agreement between the two criteria in particular excellent agreement in boys.
On the other hand, both criteria produced comparable results with excellent agreement in estimating the combined overweight/obesity prevalence rate among adolescent boys and girls with slight variations in the agreement coefficients values across the age and sex groups. These observations indicate that either CDC or IOTF are appropriate when overall prevalence rate of overweight and obesity is intended to be determined but in case of obesity alone, there is marked discrepancy between the two methods.
The findings of our study are consistent with the results of many previously published studies, which addressed overweight or obesity in children. In most studies, the combination of overweight and obesity was estimated similarly by both CDC and IOTF with slight variations but the estimated prevalence of obesity by CDC was greater than IOTF.[29–32] In a study of 2-17 years old children from the Health Survey for England and the US National Health and Nutrition Examination Survey by Long et al., CDC estimated the highest prevalence of obesity in younger children.[31] The estimates of obesity prevalence in another study of Argentinean children, was even much greater than IOTF by 5.4 times whereas both criteria produced comparable estimation of overweight prevalence.[30] Similarly, in a study by Vidals et al., both criteria estimated overweight comparably, but CDC produced significantly higher estimate of obesity particularly in the boys and the girls under 5 years.[32] Nevertheless, in some studies the estimate of overweight prevalence rate using CDC was lower than IOTF.[33,34] In contrast to our study, Klishadi et al. reported that the estimated prevalence of overweight among the Iranian children and adolescents produced by the CDC reference was lower than IOTF but the rate of obesity was higher and the kappa correlation coefficient between CDC and IOTF was 0.71.[33] A similar result was observed in a study of Chilean school children that the estimated prevalence of overweight using CDC was lower, but the prevalence of obesity was higher than IOTF.[34] In all studies, CDC criteria resulted to higher prevalence of obesity than IOTF, but in a few studies, the estimated obesity prevalence by CDC was much higher than IOTF.[7,29,30] In a study of Canadian preschool children, while both criteria produced similar estimates for prevalence of overweight similar to our findings, the estimates, however, for obesity prevalence using CDC was two times greater than IOTF.[29] In another study of school children, the prevalence of overweight, as well as obesity estimated by CDC was higher than IOTF but the prevalence of obesity particularly in the girls estimated by CDC was significantly higher compared with IOTF references.[35]
These observations indicate that the results of epidemiologic studies which addressed the prevalence rate of obesity or overweight in children should be interpreted with caution because the prevalence of obesity varies according to the criteria applied for the definition of obesity. In addition, the results may be affected by several other factors such as age, sex, ethnicity and distribution of overweight across the study population.[24,36–38] In a study of Wang et al., the results of different references assessing child and adolescent overweight and obesity were compared and a remarkable absolute difference in the estimates according to different references was attributed to prevalence rate of overweight and the difference increased by raising the overweight prevalence.[24] In addition, the results of classification using CDC or IOTF can be affected by BMI distribution.[36] Moreover, one might argue the difference of coverage rate of adolescents in elementary and high schools. This difference would not be a bias the comparison of two criteria in assessment of overweight/obesity since both criteria applied on the same subjects under study.
Since in children, the future complications of obesity is strongly associated with body fatness distribution and the percentage of adiposity, so references that showed higher correlation with adiposity are expected to have greater predictive ability of future complications. In addition, earlier identification of obesity in children is also very important. In one study of children under 5 years, using CDC criteria resulted in earlier identification of larger number of children with weight problem.[32]
Although, BMI can also offer a reasonable measure of adiposity in both children and adolescents, the criteria selected to identify children obesity should supply appropriate assessment of obesity across life span particularly in adulthood.[19] The utility of both CDC and IOTF in prediction of future outcome was shown in a study of 4-15 years old boys and girls by Johnssen et al. In this study, over a follow-up period of 13-24 years, both criteria predicted obesity and metabolic disorders in young adulthood. However, CDC was more sensitive but slightly less specific than IOTF references.[7]
The diagnostic accuracy of CDC and IOTF against the percentage of body fat greater or equal to 95 percentiles was assessed. In a study of 12-18 years old children, CDC and IOTF criteria demonstrated very high specificity but low sensitivity.[39] However, the sensitivity for CDC in this study was optimal.[39] In another study of Afro-Caribbean adolescent population, CDC cutoffs had a higher sensitivity than the IOTF cutoffs in screening excess fat. Both, criteria had high specificity with few false negative rates.[40]
CONCLUSION
In conclusion the results of this study in agreement with several previous studies indicate that both CDC and IOTF can be used for classification of overweight and obesity in youth. Based on our study, both criteria are useful for estimating excess weight in adolescents but in case of obesity CDC produce higher estimate particularly in older boys. Both, criteria indicated the high level of agreement in diagnosis of obesity and demonstrated comparable ability in predicting future outcomes. However, CDC has an ability to identify further cases of adolescents with obesity at earlier age.
ACKNOWLEDGMENTS
The authors would like to acknowledge the Deputy of Research of Babol University of Medical Sciences for their supports and to the nursing students of Babol University of Medical Sciences and school health care givers for their assistance in the data collection.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Vereecken CA, Todd J, Roberts C, Mulvihill C, Maes L. Television viewing behaviour and associations with food habits in different countries. Public Health Nutr. 2006;9:244–50. doi: 10.1079/phn2005847. [DOI] [PubMed] [Google Scholar]
- 2.Eichen DM, Conner BT, Daly BP, Fauber RL. Weight perception, substance use, and disordered eating behaviors: Comparing normal weight and overweight high-school students. J Youth Adolesc. 2012;41:1–13. doi: 10.1007/s10964-010-9612-8. [DOI] [PubMed] [Google Scholar]
- 3.Rafraf M, Gargari BP, Safaiyan A. Prevalence of pre hypertension and hypertension among adolescent high school girls in Tabriz, Iran. Food Nutr Bull. 2010;31:461–5. doi: 10.1177/156482651003100308. [DOI] [PubMed] [Google Scholar]
- 4.Liou YM, Iou TH, Chang LC. Obesity among adolescents: Sedentary leisure time and sleeping as determinants. J Adv Nurs. 2010;66:1246–56. doi: 10.1111/j.1365-2648.2010.05293.x. [DOI] [PubMed] [Google Scholar]
- 5.Wang Y, Beydoun MA. The obesity epidemic in the united State-gender, age, socioepidemic, racial/ethnic and geographic characteristics: A systematic review and meta analysis. Epidmiol Rev. 2007;29:6–28. doi: 10.1093/epirev/mxm007. [DOI] [PubMed] [Google Scholar]
- 6.Must A. Morbidity and mortality associated with elevated body weight in children and adolescents. Am J Clin Nutr. 1996;63:445S–7S. doi: 10.1093/ajcn/63.3.445. [DOI] [PubMed] [Google Scholar]
- 7.Janssen I, Katzmarzyk PT, Boye WF, Vereecken C, Mulvihill C, Roberts C, et al. Health Behaviour in School-Aged Children Obesity Working Group. Comparison of overweight and obesity prevalence in school-aged youth from 34 countries and their relationship with physical activity and dietary patterns. Obes Rev. 2005;6:123–32. doi: 10.1111/j.1467-789X.2005.00176.x. [DOI] [PubMed] [Google Scholar]
- 8.Baratta R, Degano C, Leonardi D, Vigneri R, Frittitta L. High prevalence of overweight and obesity in 11-15 -year -old children from Sicily. Nutr Metab Cardiovasc Dis. 2006;16:249–55. doi: 10.1016/j.numecd.2005.07.009. [DOI] [PubMed] [Google Scholar]
- 9.Steinbeck K. Obesity and nutrition in adolescents. Adolesc Med State Art Rev. 2009;20:900–14, ix. [PubMed] [Google Scholar]
- 10.Mirmiran P, Sherafat-Kazemzadeh R, Jalali-Farahani S, Azizi F. Childhood obesity in the Middle East. East Mediterr Health J. 2010;16:1–16. [PubMed] [Google Scholar]
- 11.Kelishadi R. Childhood overweight, obesity and the metabolic syndrome in developing countries. Epidemiol Rev. 2007;29:62–76. doi: 10.1093/epirev/mxm003. [DOI] [PubMed] [Google Scholar]
- 12.Anderson K, Patton GC, McKercher C, Dwyer T, Venn AJ. Overweight and obesity in childhood and risk of mental disorder: A 20-year cohort study. Aust N Z J Psychiatry. 2011;45:384–92. doi: 10.3109/00048674.2011.570309. [DOI] [PubMed] [Google Scholar]
- 13.Hamidi A, Fakhrzadeh H, Moayyeri A, Pourebrahim R, Heshmat R, Noori M, et al. Obesity and associated cardiovascular risk factors in Iranian children: A cross-sectional study. Pediatr Int. 2006;48:566–71. doi: 10.1111/j.1442-200X.2006.02273.x. [DOI] [PubMed] [Google Scholar]
- 14.Reilly JJ, Kelly J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: Systematic review. Int J Obes (Lond) 2010;35:891–8. doi: 10.1038/ijo.2010.222. [DOI] [PubMed] [Google Scholar]
- 15.Guijarro De Armas MG, Monereo Megias S, Civantos Modino S, MontañoMartínez JM, Iglesias Bolaños P, et al. Prevalence of carbohydrate metabolism disturbances in a population of children and adolescents with severe obesity. Endocrinol Nutr. 2010;57:467–71. doi: 10.1016/j.endonu.2010.09.002. [DOI] [PubMed] [Google Scholar]
- 16.Wabitsch M, Hauner H, Hertrampf M, Muche R, Hay B, Mayer H, et al. Type II diabetes mellitus and impaired glucose regulation in Caucasian children and adolescents with obesity living in Germany. Int J Obes Relat Metab Disord. 2004;28:307–13. doi: 10.1038/sj.ijo.0802555. [DOI] [PubMed] [Google Scholar]
- 17.Dietz WH, Bellizzi MC. Introduction: The use of body mass index to assess in children. Am J Clin Nutr. 1999;70:123S–5S. doi: 10.1093/ajcn/70.1.123s. [DOI] [PubMed] [Google Scholar]
- 18.Zimmermann MB, Gübeli C, Püntener C, Molinari L. Detection of overweight and obesity in national sample of 6-12-y-old Swiss children: Accuracy and validity of reference values for body mass index from the US Centers for Disease Control and Prevention and International Obesity Task Force. Am J Clin Nutr. 2004;79:838–43. doi: 10.1093/ajcn/79.5.838. [DOI] [PubMed] [Google Scholar]
- 19.Dietz WH, Bellizzi MC. Introduction: The use of body mass index to assess obesity in children. Am J Clin Nutr. 1999;70:123S–5S. doi: 10.1093/ajcn/70.1.123s. [DOI] [PubMed] [Google Scholar]
- 20.Report of a WHO consultation on obesity. Geneva: WHO; 1998. Report of a WHO consultation on obesity. [Google Scholar]
- 21.Physical status, the use and interpretation of anthropometry, WHO technical report series. Geneva: WHO; 1995. WHO; p. 854. [PubMed] [Google Scholar]
- 22.CDC clinical growth charts. Atlanta, Georgia. Centres for disease control and prevention. 2000. [Last assessed on 2012 Feb 11]. Available from: http://www.cdc.gov/growthcharts .
- 23.Cole TJ, Bellizzi MC, Flegal M, Dietz WH. Establishing a standard definition for child overweight and obesity wordwidw: International survey. BMJ. 2000;320:1240–3. doi: 10.1136/bmj.320.7244.1240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Wang Y, Wang JQ. A comparison of international references for the assessment of child and adolescent overweight and obesity in different population. Eur J Clin Nutr. 2000;56:973–82. doi: 10.1038/sj.ejcn.1601415. [DOI] [PubMed] [Google Scholar]
- 25.Moayeri H, Bidad K, Aghamohammadi A, Rabbani A, Anari S, Nazemi L, et al. Overweight and obesity and their associated factors in adolescents in Tehran, Iran, 2004-2005. Eur J Pediatr. 2006;165:489–93. doi: 10.1007/s00431-006-0101-8. [DOI] [PubMed] [Google Scholar]
- 26.Mohammadpour-Ahranjani B, Rashidi A, Karandish M, Eshraghian MR, Kalantari N. Prevalence of overweight and obesity in adolescent Tehrani students, 2000-2001: An epidemic health problem. Public Health Nutr. 2004;7:645–8. doi: 10.1079/phn2003593. [DOI] [PubMed] [Google Scholar]
- 27.Maddah M, Nikooyeh B. Factors associated with overweight in children in Rasht, Iran: Gender, maternal education, skipping breakfast and parental obesity. Public Health Nutr. 2010;13:196–200. doi: 10.1017/S1368980009990589. [DOI] [PubMed] [Google Scholar]
- 28.Hajian-Tilaki K, Heidari B. Prevalence of overweight, obesity and their association with physical activity pattern among Iranian youth aged 12-17 years. J Public Health Nutr. 2012;14:1–7. doi: 10.1017/S1368980012001048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Twells LK, Newhook LA. Obesity prevalence estimates in a Canadian regional population of preschool children using variant growth references. BMC Pediatr. 2011;11:21. doi: 10.1186/1471-2431-11-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Padula G, Salceda SA. Comparison between references of the overweight and obesity prevalence, through the body mass index in Argentinean children. Arch Latinoam Nutr. 2008;58:330–5. [PubMed] [Google Scholar]
- 31.Lang IA, Kipping RR, Jago R, Lawlor DA. Variation in childhood and adolescent obesity prevalence defined by international and country-specific criteria in England and the united statees. Eur J Clin Nutr. 2011;65:143–50. doi: 10.1038/ejcn.2010.260. [DOI] [PubMed] [Google Scholar]
- 32.Vidal E, Carlin E, Driul D, Tomat M, Tenore A. A comparison study of the prevalence of overweight and obese Italian preschool children using different reference standards. Eur J Pediatr. 2006;165:696–700. doi: 10.1007/s00431-006-0152-x. [DOI] [PubMed] [Google Scholar]
- 33.Kelishadi R, Ardalan G, Gheiratmand R, Majdzadeh R, Hosseini M, Gouya MM, et al. Caspian Study Group. Overweight and obesity in a national sample of Iranian children and adolescents: CASPIAN Study. Child Care Health Dev. 2008;34:44–54. doi: 10.1111/j.1365-2214.2007.00744.x. [DOI] [PubMed] [Google Scholar]
- 34.Ulloa N, Sapunar J, Bustos P, Sáez K, Asenjo S, Taibo M, et al. Frequency of obesity and overweight among school age children living in southern Chile. Rev Med Chil. 2010;138:1365–72. [PubMed] [Google Scholar]
- 35.Pedrosa C, Correia F, Seabra D, Oliveira BM, Simões-Pereira C, Vaz-de-Almeida MD. Prevalence of overweight and obesity among 7-9-year-old children in Aveiro, Portugal: comparison between IOTF and CDC references. Public Health Nutr. 2011;14:14–9. doi: 10.1017/S1368980009991789. [DOI] [PubMed] [Google Scholar]
- 36.Tuan NT, Butte NF, Nicklas TA. BMI distributions affect discrepancies in weight classifications in children. Pediatr Int. 2012;54:256–65. doi: 10.1111/j.1442-200X.2011.03539.x. [DOI] [PubMed] [Google Scholar]
- 37.Freedman DS, Wang J, Thornton JC, Mei Z, Pierson RN, Jr, Dietz WH, et al. Racial/ethnic differences in body fatness among children and adolescents. Obesity (Silver Spring) 2008;16:1105–11. doi: 10.1038/oby.2008.30. [DOI] [PubMed] [Google Scholar]
- 38.Duncan JS, Duncan EK, Schofield G. Accuracy of body mass index (BMI) thresholds for predicting excess body fat in girls from five ethnicities. Asia Pac J Clin Nutr. 2009;18:404–11. [PubMed] [Google Scholar]
- 39.Deurenberg-Yap M, Niti M, Foo LL, Ng SA, Loke KY. Diagnostic accuracy of anthropometric indices for obesity screening among Asian adolescents. Ann Acad Med Singapore. 2009;38:3–6. [PubMed] [Google Scholar]
- 40.Nichols SD, Cadogan F. BMI-based obesity cutoffs and excess adiposity in a Caribbean adolescent population of African origin. Eur J Clin Nutr. 2009;63:253–8. doi: 10.1038/sj.ejcn.1602913. [DOI] [PubMed] [Google Scholar]