

Abstract
INTRODUCTION
The aim of this study was to compare the functional outcome between the first and second knee replacement in patients undergoing staged bilateral total knee arthroplasty.
METHODS
We identified 64 patients who had bilateral knee replacements and had at least one year of postoperative outcome studies. Data on pain scores, walking ability, use of walking aids, range of movement, instability, muscle strength, WOMAC® (Western Ontario and McMaster Universities) scores, SF-12 (Short Form 12) scores, American Knee Society radiological scores and length of hospital stay (LOS) were recorded. The difference in data between the first and second knee was assessed.
RESULTS
Groups remained statistically comparable between the first and second operation. Four outcomes showed a significant difference between the second and first knee. The mean score for postoperative walking ability was 4.83 (second knee) vs 4.51 (first knee) (p=0.03). The mean score for postoperative walking aid requirement was 5.73 (second knee) vs 5.46 (first knee) (p=0.01). The mean postoperative SF-12 score was 54.26 (second knee) vs 52.45 (first knee) (p=0.04). The mean LOS was 4.73 days (second knee) vs 6.16 days (first knee) (p=0.05). All other data comparisons were statistically insignificant.
CONCLUSIONS
Patients have a reduced LOS and continue to improve after the second procedure with regards to walking ability, use of walking aids and psychological wellbeing.
Keywords: Knee, Replacement, Arthroplasty, Bilateral, Staged
Osteoarthritis is a common disorder of the joints that affects more than 2 million people in the UK and studies suggest that this number will double in the next 20 years. The condition is associated strongly with ageing and is believed to affect up to 30% of people over 60 years of age.1 Primary total knee replacement (TKR) is most commonly performed for osteoarthritis of the knee. Other indications include rheumatoid arthritis, juvenile chronic arthritis, osteonecrosis and other types of inflammatory arthritis. The aims of TKR are pain relief and improvement in function. Candidates for elective TKR should have radiographic evidence of joint damage, moderate to severe persistent pain that is not relieved adequately by an extended course of non-surgical management and clinically significant functional limitation resulting in diminished quality of life.2
A total of 71,527 primary knee replacement procedures were performed in the UK in 2008.3 A significant proportion of such patients present with bilateral knee osteoarthritis and require bilateral TKRs. This can be done simultaneously under the same anaesthetic setting or as a staged operation with a variable length of time between each arthroplasty.
The advantages of having a simultaneous procedure include reduced cost, exposure to the risk of only one anaesthetic, earlier return to baseline function and convenience for the patient.4 However, having a TKR causes a stress response and the response is directly related to the proportion of tissue damage.5,6 There is also increased blood loss and this can lead to a higher risk of serious cardiac complications, pulmonary complications and mortality compared with staged bilateral procedures, especially in the older group of patients.4,7
The optimal time interval between the two operations of staged bilateral procedures has yet to be identified. Recent studies have shown that an interval of as little as one week is safe and effective.8,9 However, patients are often recommended to wait a few months to gain maximum function from the initial procedure before embarking on the second arthroplasty. After the initial knee replacement, patients are generally keen to know whether the second knee will functionally be as good as the first.
There is no literature comparing the outcomes of the first and second knee in patients undergoing staged bilateral procedures. Therefore, the aim of this study was to compare the functional outcome between the first and second knee replacement in patients undergoing staged bilateral procedures, with a view to improve understanding of the postoperative recovery and rehabilitation and to allow an improvement in consenting patients with regard to addressing commonly asked questions about functional outcomes for the second TKR.
Methods
A prospective database of outcomes of knee replacements performed at Broadgreen Hospital in Liverpool was commenced in 2003. Data were collected preoperatively, at three and twelve months postoperatively and every two years thereafter. The assessments and scores were all recorded by one senior physiotherapist.
The data collected included: pain scores including pain at rest, on walking and on climbing stairs (scored 1—4); walking ability and use of walking aids (scored 1—6); stair walking ability (scored 1—5) (Table 1); range of movement; instability; muscle strength; WOMAC® (Western Ontario and McMaster Universities) scores; SF-12 (Short Form 12) scores; American Knee Society total knee arthroplasty roentgenographic evaluation scores;10 length of postoperative hospital stay (LOS); and overall satisfaction.
Table 1.
The scoring scale used in this study to assess pain, stair walking ability, walking ability and requirement for walking aids
| Score | Pain | Stairs | Walking | Walking aids |
| 1 | None | Unable | Unable | Wheelchair |
| 2 | Mild | Up with rail and unable down | Inside house | Frame |
| 3 | Moderate | Up and down with rail | 400 yards | Crutches |
| 4 | Severe | Normal up and rail down | 800 yards | Sticks |
| 5 | Normal | 1,600 yards | One stick | |
| 6 | Unlimited | Unaided |
The WOMAC® osteoarthritis index is a valid, reliable scoring method that measures pain, stiffness and physical function.11 The SF-12 health survey is also a validated test12 with 12 items that measure patient-assessed outcome including physical and mental wellbeing.
We identified 64 patients (26 male, 38 female) from the database who had staged primary bilateral knee replacements between 2003 and 2008 and who had at least one year of postoperative outcome studies performed after the second knee replacement. Data from the preoperative assessment and the one year of postoperative assessment for both knees were compared. A second subanalysis was undertaken to compare those patients who had the second operation within six months of the first with those having the second operation after six months.
Of the 128 TKRs performed, 121 (95%) were carried out by two consultant knee surgeons while 7 (5%) were performed by senior orthopaedic trainees under consultant supervision. Each patient was under the same consultant for both knee arthroplasty operations. Osteoarthritis was the primary diagnosis in 56 patients (88%) while 8 patients (12%) had rheumatoid arthritis as the indication for the knee arthroplasty.
The results were analysed using the Mann—Whitney U test for comparisons between first and second knees, and the Wilcoxon test for comparisons between patients having surgery on their second knee before or after six months from their first TKR.
Results
Groups remained statistically comparable between the first and second operation. The mean score for postoperative walking ability was 4.83 (second knee) vs 4.51 (first knee) (p=0.03) (Fig 1). The mean score for postoperative walking aid requirement was 5.73 (second knee) vs 5.46 (first knee) (p=0.01) (Fig 1). The patients’ mean postoperative SF-12 mental scores were 54.26 (second knee) vs 52.45 (first knee) (p=0.04) (Fig 2). The mean postoperative LOS was 4.73 (second knee) vs 6.16 (first knee) (p=0.05) (Fig 3). Therefore, patients were in hospital on average one day less, had a reduced walking aid requirement and coped better psychologically.
Figure 1.
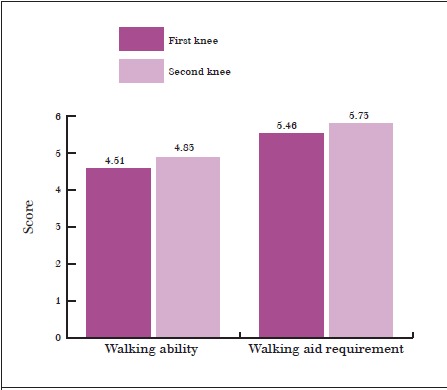
Mean post-operative walking ability and walking aid requirement
Figure 2.
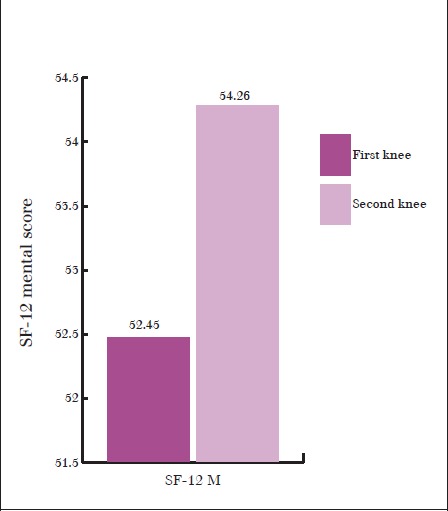
Mean post-operative SF-12 mental scores
Figure 3.
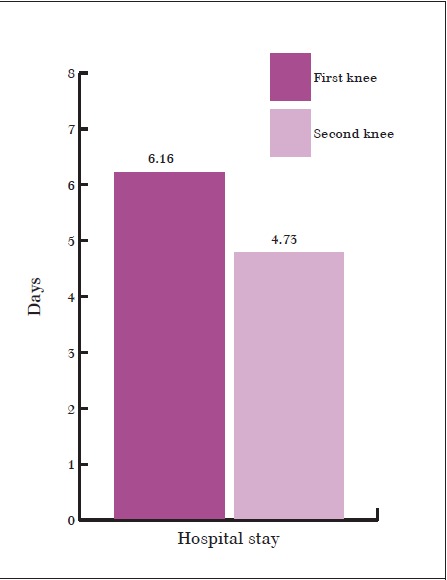
Mean length of post-operative hospital stay
The differences between the first and second operation regarding postoperative pain, stair-walking ability, range of movement, instability, muscle strength, WOMAC® scores, satisfaction with the operation, Knee Society radiological scores and SF-12 physical scores were statistically insignificant.
In addition, we looked at the timing between the two knee replacements and whether this affected the functional outcome. The interval between the two operations of staged knee replacements ranged from 105 to 734 days with a mean of 290 days. Out of the 64 patients included in our study, 16 patients (33.3%) had their second TKR within 6 months of their first (Group A) while 48 patients (66.7%) had their second TKR more than 6 months after the first (Group B).
The functional outcomes between these two subgroups were assessed using the same scores. Comparing results for Groups A and B respectively, the mean score for postoperative walking ability was 5.14 vs 4.74 (p=0.23), the mean score for postoperative walking aid requirement was 5.86 vs 5.70 (p=0.46) (Fig 4), the mean maximum flexion was 100.63 vs 98.54 (p=0.53), the mean range of motion was 101.00 vs 97.23 (p=0.35) (Fig 5) and the mean LOS was 4.25 vs 4.90 days (p=0.32). Hence, no significant difference was detected between these two groups.
Figure 4.
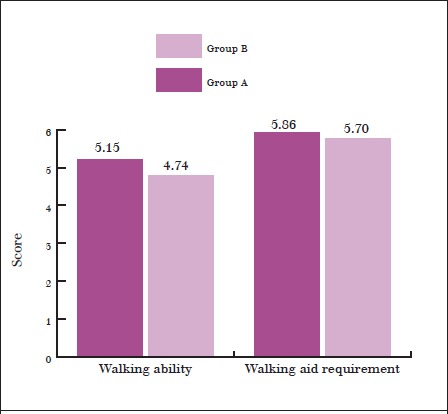
Mean post-operative walking ability and walking aid requirement in patients who had their second knee replacement within six months of the first (Group A) and those who had their second knee replacement after more than six months (Group B)
Figure 5.
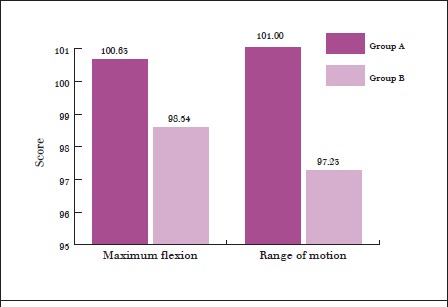
Mean post-operative maximum flexion and range of motion in patients who had their second knee replacement within six months of the first (Group A) and those who had their second knee replacement after more than six months (Group B)
Discussion
Knee arthritis is a common problem that may require treatment with TKR at its end stage. For patients requiring bilateral TKRs, controversy remains whether a simultaneous or staged procedure is better. In terms of functional outcomes of simultaneous and staged bilateral TKRs, there is some evidence of comparable prosthetic survival rates and knee scores,13 with patients undergoing simultaneous procedures having an overall shorter LOS.9 However, due to the increased risks involved when performing both simultaneously, it has been suggested to perform staged procedures.4,7 In staged procedures patients have their worst knee operated on first and after complete recovery they proceed to having their second knee replaced. It is unclear how long to delay the timing between procedures for bilateral staged TKRs although there have been some studies suggesting that an interval of between 4 and 7 days is a viable and safe option.8,9,14
Most of the literature on bilateral TKRs compares simultaneous and staged procedures. However, with the evidence pointing to staged procedures being the safer option, there have been no studies comparing what the functional outcomes are between the first and second TKR in a staged procedure. It was our aim to provide this information and therefore help with preoperative planning and consent. Our study shows that patients have a reduced LOS by an average of 1.43 days (4.73 vs 6.16 days) after their second TKR when compared with the first. This finding aids preoperative planning and gives an indication of the extent of nursing care required in the postoperative period. It is also useful information for hospital budgeting.
There was no change in practice in our hospital over the years that could account for the decrease in LOS. Postoperative hospital stay was measured from the date of surgery to the date of discharge, which was not affected by changes in preoperative admission policy. The data between 2003 and 2008 were also analysed and the average LOS for the procedures performed before 2006 and those performed after 2006 (data not shown) were compared. No statistically significant difference between the two groups was found, suggesting that the reduction in LOS in our study was not due to time progression.
As our department policy was not to perform simultaneous procedures, we cannot make a comparison of LOS for such cases. However, other studies have compared the difference in LOS between simultaneous and staged bilateral and unilateral TKRs. The conclusion was that simultaneous bilateral TKR reduces LOS compared with staged bilateral TKR.15,16 Nevertheless, patients who had simultaneous bilateral TKR had a longer LOS than patients who had a unilateral TKR only. Bullock et al reviewed 255 patients with simultaneous bilateral TKRs and 514 patients with unilateral TKRs.17 An increase in the LOS of 0.69 days was recorded for patients who had simultaneous bilateral TKRs (average: 5.11 days) compared with patients who had a unilateral TKR (average: 4.42 days).
The patients in our study continued to improve after the second procedure with regards to walking ability, use of walking aids and psychological wellbeing. The reason for these findings is unclear but it may be because having the worst knee replaced first results in an improved walking ability and therefore a decreased need for walking aids after the second operation. Also patients have already experienced one knee replacement and are therefore less apprehensive and more familiar with the postoperative physiotherapy and rehabilitation programme.
In terms of patients having a second TKR before or after 6 months after the first, there was no significant difference in any of the outcomes. However, as there were only 16 patients in one group and 48 in the other, any significant difference is harder to prove. We therefore suggest that further studies are carried out on outcomes related to timing between both TKRs.
Conclusions
Many patients are curious to know whether their second TKR will be the same as their first. Our results allow us to inform these patients reliably prior to having their second knee replaced that they can expect to have a shorter stay in hospital and better walking ability. They are also likely to feel better psychologically compared with after their first TKR. These results may help surgeons in the consent process for patients undergoing bilateral TKRs. Our study is the first to provide such information.
References
- 1.Arden NK, Arden E, Hunter D. Osteoarthritis. New York, US: Oxford University Press; 2008. [Google Scholar]
- 2.National Institutes of Health. NIH Consensus Development Conference on Total Knee Replacement. Bethesda, MA: NIH; 2003. [Google Scholar]
- 3. National Joint Registry. 6th Annual Report. Hemel Hempstead; NJR; 2009.
- 4.Stefánsdóttir A, Lidgren L, Robertsson O. Higher early mortality with simultaneous rather than staged bilateral TKAs: results from the Swedish Knee Arthroplasty Register. Clin Orthop Relat Res. 2008;466:3,066–3,070. doi: 10.1007/s11999-008-0404-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Leopold SS, Casnellie MT, Warme WJ, et al. Endogenous cortisol production in response to knee arthroscopy and total knee arthroplasty. J Bone Joint Surg Am. 2003;85:2,163–2,167. doi: 10.2106/00004623-200311000-00016. [DOI] [PubMed] [Google Scholar]
- 6.Desborough JP. The stress response to trauma and surgery. Br J Anaesth. 2000;85:109–117. doi: 10.1093/bja/85.1.109. [DOI] [PubMed] [Google Scholar]
- 7.Restrepo C, Parvizi J, Dietrich T, Einhorn TA. Safety of simultaneous bilateral total knee arthroplasty. A meta-analysis. J Bone Joint Surg Am. 2007;89:1,220–1,226. doi: 10.2106/JBJS.F.01353. [DOI] [PubMed] [Google Scholar]
- 8.Forster MC, Bauze AJ, Bailie AG, et al. A retrospective comparative study of bilateral total knee replacement staged at a one-week interval. J Bone Joint Surg Br. 2006;88:1,006–1,010. doi: 10.1302/0301-620X.88B8.17862. [DOI] [PubMed] [Google Scholar]
- 9.Sliva CD, Callaghan JJ, Goetz DD, Taylor SG. Staggered bilateral total knee arthroplasty performed four to seven days apart during a single hospitalization. J Bone Joint Surg Am. 2005;87:508–513. doi: 10.2106/JBJS.D.02193. [DOI] [PubMed] [Google Scholar]
- 10.Ewald FC. The Knee Society total knee arthroplasty roentgenographic evaluation and scoring system. Clin Orthop Relat Res. 1989;248:9–12. [PubMed] [Google Scholar]
- 11.Bellamy N, Buchanan WW, Goldsmith CH, et al. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. 1988;15:1,833–1,840. [PubMed] [Google Scholar]
- 12.Jenkinson C, Layte R. Development and testing of the UK SF-12 (short form health survey). J Health Serv Res Policy. 1997;2:14–18. doi: 10.1177/135581969700200105. [DOI] [PubMed] [Google Scholar]
- 13.Ritter MA, Harty LD, Davis KE, et al. Simultaneous bilateral, staged bilateral, and unilateral total knee arthroplasty. A survival analysis. J Bone Joint Surg Am. 2003;85:1,532–1,537. doi: 10.2106/00004623-200308000-00015. [DOI] [PubMed] [Google Scholar]
- 14.Hashmi FR, Barlas K, Mann CF, Howell FR. Staged bilateral hip or knee arthroplasties. J Orthop Surg (Hong Kong) 2007;15:159–162. doi: 10.1177/230949900701500206. [DOI] [PubMed] [Google Scholar]
- 15.Jankiewicz JJ, Sculco TP, Ranawat CS, et al. One-stage versus 2-stage bilateral total knee arthroplasty. Clin Orthop Relat Res. 1994;309:94–101. [PubMed] [Google Scholar]
- 16.Brotherton SL, Roberson JR, de Andrade JR, Fleming LL. Staged versus simultaneous bilateral total knee replacement. J Arthroplasty. 1986;1:221–228. doi: 10.1016/s0883-5403(86)80011-0. [DOI] [PubMed] [Google Scholar]
- 17.Bullock DP, Sporer SM, Shirreffs TG. Comparison of simultaneous bilateral with unilateral total knee arthroplasty in terms of perioperative complications. J Bone Joint Surg Am. 2003;85:1,981–1,986. doi: 10.2106/00004623-200310000-00018. [DOI] [PubMed] [Google Scholar]