

Abstract
INTRODUCTION
Foreign bodies in the urogenital tract are not uncommon. Hairpins, glass rods, umbilical tapes, ball point pen are described in lower urogenital tract. Retained gauze piece (gossypiboma) in posterior urethra may cause diagnostic dilemma. Symptoms and investigations may mimic stricture of posterior urethra.
PRESENTATION OF CASE
Two cases of retained gauze pieces in the urethra are described here. The micturating cystourethrogram was suggestive of posterior urethral stricture.
DISCUSSION
Two cases described here had retained gauze piece as a cause of filling defect and abnormal appearance in the micturating cystourethrogram. Gossypiboma may be a possibility where posterior urethral stricture are seen after previous surgery in paediatric age group.
CONCLUSION
In the setting of previous urogenital surgery gossypiboma should be kept in the differential diagnosis where posterior urethral stricture are seen in the paediatric age group.
Keywords: Gossypiboma, Posterior urethral stricture
1. Introduction
Gossypiboma (retained gauze piece) in the urinary bladder and urethra may give rise various clinical manifestations. Common presentations are lower urinary tract symptoms (LUTS), e.g. severe dysuria, frequency, urgency, pyuria, haematuria and foul smelling urine.1 Gossypiboma in the posterior urethra may give an appearance of urethral stricture. Two cases of gossypiboma are described who presented with features suggestive of posterior urethral stricture with a history of previous surgery and on exploration impacted gauze pieces were found.
2. Case report
2.1. Case 1
A five-year old male child presented complaining of not passing urine per urethra. He had undergone suprapubic cystolithotomy for bladder stone at another centre four months previously. The patient had developed retention of urine on removal of the Foleys catheter in the immediate post-operative period. Retention of urine was relieved by suprapubic cystotomy. He reported to our institution with a suprapubic cystotomy in situ complaining of not passing urine per urethra. Attempts were made to pass a urinary catheter per urethra into the bladder unsuccessfully. Routine blood and renal function tests were within normal limits. However, routine urine microscopy showed pus cells in abundance. Ultrasonography did not revealed any stone or suspicious foreign body in the urinary bladder. Contrast study done through suprapubic catheter showed contrast in urinary bladder but not in the urethra. Retrograde urethrogram revealed absence of contrast in the posterior urethra simulating urethral stricture (Fig. 1). We attempted to perform cystoscopy but were not able to negotiate beyond the bulbar urethra and during negotiation of the catheter through cystostomy, a big piece of gauge was found inside the posterior urethra causing bladder outflow obstruction (Fig. 2). It was removed. Patient was asymptomatic after removal of gauge piece. At the follow up of six months the patient had no complaints and was passing urine normally.
Fig. 1.
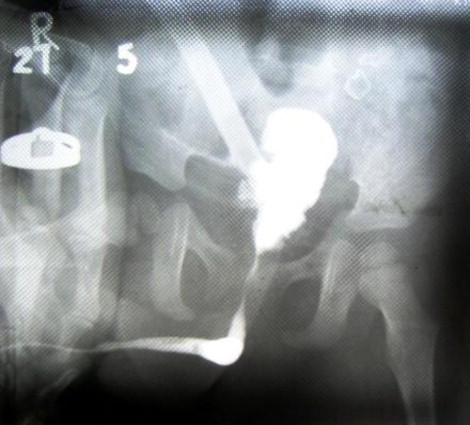
RGU showing stricture posterior urethra.
Fig. 2.

Gauge piece coming out from bladder.
2.2. Case 2
A six-year old boy reported with complaining of retention of urine for a day. Three month previously the patient had undergone surgery for bladder stone. Thereafter the patient complained of poor stream and straining during micturation. Routine blood, urine examinations and renal function tests were within normal limits. Retrograde urethrogram revealed a stricture in the posterior urethra with the irregular outline (Fig. 3). Ultrasonography showed bilateral renal stones with no bladder pathology. The patient was operated for the left renal stone and left sided DJ stent was inserted. In the immediate post operative period the patient passed urine along with a small size of gauge piece and the DJ stent (Fig. 4). Subsequently the patient passed urine normally with a good stream.
Fig. 3.
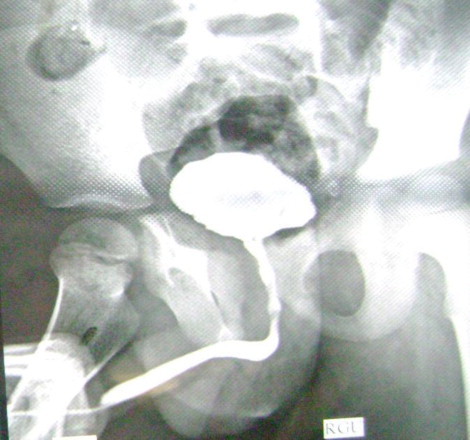
RGU showing stricture of posterior urethra.
Fig. 4.

Photograph showing piece of gauge piece expelled per urethra.
3. Discussion
Foreign bodies in the urethra and urinary bladder have been reported either due to self insertion for sexual gratification, psychological disorder, traumatic, migration from adjacent organs or inadvertently retained after previous surgical intervention.2,3 Some studies described leech as foreign body in the urinary bladder causing haematuria.4 The urethra and bladder forms common passages if foreign bodies are inserted into the urinary tract.5 Types of foreign bodies in the urinary bladder and urethra consists of glass rods, hairpins, umbilical tapes, ball point pen, pencil, rubber tube, penrose drain, bougie,6 retained gauze piece (gossypiboma) and even nonabsorbable sutures causing stone formation leading to persistent cystitis.7 Usually these foreign bodies give features of lower urinary tract symptoms like dysuria, pyuria, haematuria, urgency, frequency and foul smelling urine. Retained, forgotten and lost foreign bodies during previous operations have been retrieved in subsequent operations. Gossypiboma in the urinary bladder diagnosed by ultrasound can be endoscopically removed in large gossypibomas suprapubic cystostomy8 is required. In these case reports the gossypiboma was simulating a urethral stricture. In the first case cystourethroscope could not be negotiated beyond the anterior urethra hence, suprapubic cystostomy was performed and a gauze piece was impacted in the posterior urethra was removed. In the second case, an elongated gauze piece along with the double J stent was expelled per urethra while straining during micturition.
Both patients were passing urine normally in the routine follow up visits.
Delayed complications such as urethral stricture can occur, so close follow up is recommended.
4. Conclusion
A gossypiboma in the urethrovesical canal may simulate stricture in the posterior urethra causing diagnostic dilemma. In cases where there is history of previous surgery, in the differential diagnosis of urethral stricture gossypiboma should be considered.
Conflict of interest statement
None.
Funding
None.
Ethical approval
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Authors contributions
Bindey Kumar, Zaheer Hasan, Prem Kumar and Rajiv Nayan Priyadarshi contributed to study, design and writing. Vinit Kumar Thakur and Manish Mandal contributed to data collection. Neelam Sinha and Sanjay Kumar Sinha contributed to data analysis.
References
- 1.Santosh Kumar, Mavuduru R.S., Acharya N.C. Gossypiboma of the urinary bladder. International Journal of Gynaecology and Obstetrics. 2008;102(July (1)):79–80. doi: 10.1016/j.ijgo.2008.02.013. [DOI] [PubMed] [Google Scholar]
- 2.Walsh P., Moustafa M. Retention of urethrovesical foreign bodies: case report and literature review. The Journal of Emergency Medicine. 2000;19(3):241–243. doi: 10.1016/s0736-4679(00)00232-8. [DOI] [PubMed] [Google Scholar]
- 3.Moon S.J., Kim D.H., Chung J.H., Jo J.K., Son Y.W., Choi H.Y. Unusual foreign bodies in the urinary bladder and urethra due to autoerotism. International Neurourology Journal. 2010;14:186–189. doi: 10.5213/inj.2010.14.3.186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Alam S., Das Chaudhary M.K., Islam K. Leech in urinary bladder causing haematuria. Journal of Paediatric Urology. 2008;4(February (1)):70–73. doi: 10.1016/j.jpurol.2007.02.004. [DOI] [PubMed] [Google Scholar]
- 5.Cho D.S., Kim S.J., Choi J.B. Foreign bodies in urethra and bladder by implements used during sex behavior. Korean Journal of Urology. 2003;44:1131–1134. [Google Scholar]
- 6.Siva Prasad, Smith A.M., Uson A., Melicon M., Lattimer J.K. Foreign bodies in urinary bladder. Urology. 1973;2(3):B345–C3455. doi: 10.1016/0090-4295(73)90460-3. [DOI] [PubMed] [Google Scholar]
- 7.Lam C.-Y., Tsai S.-W., Chen C.-H. Foreign body in urinary bladder causing persistent cystitis. Formosan Journal of Surgery. 2011;44(August (4)):160–162. [Google Scholar]
- 8.Pal D.K., Bag A.K. Intravesical wire as foreign body in urinary bladder. International Brazilian Journal of Urology. 2005;31:472–474. doi: 10.1590/s1677-55382005000500010. [DOI] [PubMed] [Google Scholar]