

Abstract
Background. The breech extraction of the fetus through the vagina has a greater risk of hip fracture compared with the extraction by abdominal route. Case. A 2390 g female infant was delivered at 39 weeks by elective cesarean section for breech presentation. The newborn sustained a fracture of the right femur. A simple immobilization of the limb in extension led to a complete healing of the fracture without sequelae. Conclusion. Caesarean delivery reduces the risk of causing a traumatic injury of the newborn compared to vaginal delivery, especially with breech presentation but does not eliminate this possible accidental complication.
1. Introduction
The vaginal breech birth, even if rarely, can lead to traumatic outcome as a fracture of the femur [1]. For cesarean section with breech presentation, such cases are even if more rare, but still possible, as reported in the literature [2–8]. The multicenter, randomized study of Hannah et al. [9] showed that the fracture of long bones occurred in 0.1% of cases during caesarean section and 0.5% for vaginal delivery.
Planning caesarean section reduces the risk of fracture of long bones but does not eliminate the possibility [10–13].
We present a case of right femur fracture that occurred in the course of cesarean section performed because of breech presentation.
2. The Case
The case concerns a 31-year-old Caucasian patient who underwent a cesarean section for breech presentation at 39 weeks of gestation with a history of hysterotomy because of multiple myomas in 2005.
The patient underwent a vaginal delivery in 2003. The patient was subjected to epidural anesthesia to obtain an adequate analgesia and muscle relaxation. The incision was performed on the lower uterine segment, with adequate width. The fetus showed a frank transverse situation, the iliac crest of the podex fetal found to be below the incision. The operator has engaged the left thigh and performed a pull to extract the fetus as usual in a breech extraction during cesarean section. The breech was engaged without difficulty, and the fetus was extracted directly by the lower limbs. During the extraction, we did not hear any suspicious sounds (crack) [12]. A 2390 g female infant was delivered with Apgar scores of 9 and 10 at 1 and 5 min, respectively.
At the time of extraction, we did not pay particular attention to the right thigh of the newborn. The baby was subjected to careful clinical examination, and routine laboratory tests showed no abnormalities.
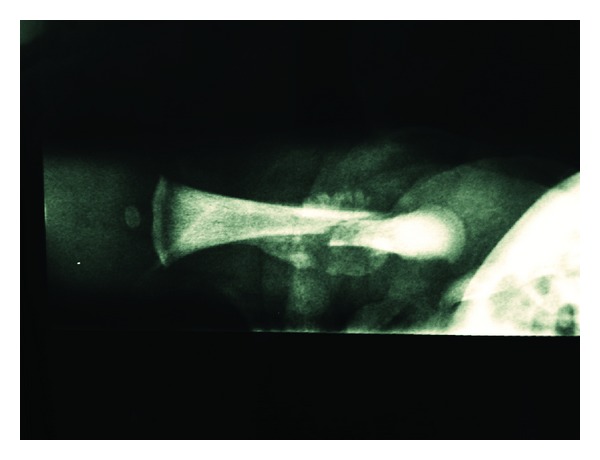
On the day after birth, the neonate remained irritable and was disinterested in feeding; the right thigh had a step on palpation and reduced mobility. The clinical signs led the neonatology team to perform an X-ray of the legs of the newborn. The examination revealed a fracture of the right femur in which the proximal segment displaced anteriorly compared to the middle and distal segment (Figure 1). The bone structure and mineralization were visibly normal; there was no indication of any other fracture/bone deformities or anomalies osteo-articular (blue sclera, osteogenesis imperfecta, or hypotonia). In particular, Welding-Hofmann disease, the pathology that promotes bone atrophy and facilitates pathologic fractures of long bones, was excluded.
Figure 1.

Rx showing right femur fracture.
The newborn was treated with immobilization in extension (Figure 2).
Figure 2.

Immobilization of the right leg in extension.
On the tenth day after birth, the radiogram control showed the formation of a callus at the level of the margins of fracture. At 20 days a further control radiogram showed progression of the callus (Figure 3). It was decided to remove the immobilization 23 days after birth; the child was able to move his right leg actively in all planes of space. At the 75th day after birth, the fracture was found to be fully welded.
Figure 3.
Rx showing the healing of the fracture.
At 20 weeks after the birth, both lower limbs showed a proper mobility with no dysmetria.
3. Discussion
We have already demonstrated that cesarean section induced 3.12% accidental fetal lacerations [14]. In the medical literature, there are only nine articles reporting cases of hip fracture during cesarean section [1–5, 7, 10, 12, 13]. This possibility, as is reported in the literature, is extremely rare. Some conditions that can be regarded as favoring the above complications are mainly represented by twin pregnancy, inadequate uterine relaxation, the presence of myomas, inadequate incision in the lower uterine segment, and also the presentation of breech well engaged in the pelvis. The current lack of available data and the extreme rarity of this complication do not detect an adequate and precise maneuvering to avoid fracture of the femur. An appropriate set of rules and procedures may prevent the occurrence of such an incident. These rules are represented by an adequate analgesia, extraction by exercising a delicate traction, by performing an uterine incision that is sufficiently wide to allow a smooth extraction. In this regard, it is recommended an extension of the uterine incision rather than continue to exert traction difficult and/or dangerous. The occurrence of characteristic sound (crack) [12] may be regarded as an important sign to put on suspicion of breaking the femur of the newborn during extraction. This finding should prompt when warned to carry out further investigations such as X-rays of the lower limbs of the newborn, all in accordance with the neonatologists. These recommendations represent the process more correctly for early detection of this complication, in order to prepare an early treatment of the condition. In our case, there were no predisposing conditions. The extraction was apparently simple, without particular or excessively energetic tractions. The occurrence of fracture of the femur in the neonatal was a real surprise. This case increases the awareness of the clinical complications in the course of cesarean section.
4. Conclusion
Cesarean delivery reduces the risk of causing a traumatic injury of the newborn compared to vaginal delivery, especially with breech presentation, but does not eliminate this possible accidental complication [15].
Conflict of Interests
The authors hereby declare that they have no conflict of interests to declare.
Disclaimer
The authors alone are responsible for the content and writing of the paper.
Ethical Approval
Ethical consent for the work has been given.
Consent
The authors confirm that the patient described in this paper has given her informed consent for the paper to be published.
References
- 1.Ehrenfest H. Birth Injuries of the Child. New York, NY, USA: Appleton-Century Crofts; 1922. [Google Scholar]
- 2.Kellner KR. Neonatal fracture and cesarean section. American Journal of Diseases of Children. 1982;136(9, article 865) doi: 10.1001/archpedi.1982.03970450107027. [DOI] [PubMed] [Google Scholar]
- 3.Barnes AD, Van Geem TA. Fractured femur of the newborn at cesarean section. A case report. Journal of Reproductive Medicine for the Obstetrician and Gynecologist. 1985;30(3):203–205. [PubMed] [Google Scholar]
- 4.Vasa R, Kim MR. Fracture of the femur at cesarean section: case report and review of literature. American Journal of Perinatology. 1990;7(1):46–48. doi: 10.1055/s-2007-999445. [DOI] [PubMed] [Google Scholar]
- 5.Awwad JT, Nahhas DE, Karam KS. Femur fracture during cesarean breech delivery. International Journal of Gynecology and Obstetrics. 1993;43(3):324–326. doi: 10.1016/0020-7292(93)90524-z. [DOI] [PubMed] [Google Scholar]
- 6.Morris S, Cassidy N, Stephens M, McCormack D, McManus F. Birth-associated femoral fractures: incidence and outcome. Journal of Pediatric Orthopaedics. 2002;22(1):27–30. [PubMed] [Google Scholar]
- 7.Cebesoy FB, Cebesoy O, Incebiyik A. Bilateral femur fracture in a newborn: an extreme complication of cesarean delivery. Archives of Gynecology and Obstetrics. 2009;279(1):73–74. doi: 10.1007/s00404-008-0639-y. [DOI] [PubMed] [Google Scholar]
- 8.Burke SW, Jameson VP, Roberts JM. Birth fractures in spinal muscular atrophy. Journal of Pediatric Orthopaedics. 1986;6(1):34–36. doi: 10.1097/01241398-198601000-00007. [DOI] [PubMed] [Google Scholar]
- 9.Hannah ME, Hannah WJ, Hewson SA, Hodnett ED, Saigal S, Willan AR. Planned caesarean section versus planned vaginal birth for breech presentation at term: a randomised multicentre trial. Lancet. 2000;356(9239):1375–1383. doi: 10.1016/s0140-6736(00)02840-3. [DOI] [PubMed] [Google Scholar]
- 10.Jain R, Bielski RJ. Fracture of lower femoral epiphysis in an infant at birth: a rare obstetrical injury. Journal of Perinatology. 2001;21(8):550–552. doi: 10.1038/sj.jp.7210540. [DOI] [PubMed] [Google Scholar]
- 11.O’Connell A, Donoghue VB. Can classic metaphyseal lesions follow uncomplicated caesarean section? Pediatric Radiology. 2007;37(5):488–491. doi: 10.1007/s00247-007-0445-x. [DOI] [PubMed] [Google Scholar]
- 12.Matsubara S, Izumi A, Nagai T, Kikkawa I, Suzuki M. Femur fracture during abdominal breech delivery. Archives of Gynecology and Obstetrics. 2008;278(2):195–197. doi: 10.1007/s00404-008-0655-y. [DOI] [PubMed] [Google Scholar]
- 13.Campolat FE, Kose A, Yurdakok M. Bilateral femur fracture in a neonate after cesarean delivery. Archives of Gynecology and Obstetrics. 2010;281:967–969. doi: 10.1007/s00404-009-1256-0. [DOI] [PubMed] [Google Scholar]
- 14.Dessole S, Cosmi E, Balata A, et al. Accidental fetal lacerations during cesarean delivery: experience in an Italian level III university hospital. American Journal of Obstetrics and Gynecology. 2004;191(5):1673–1677. doi: 10.1016/j.ajog.2004.03.030. [DOI] [PubMed] [Google Scholar]
- 15.Capobianco G, Angioni S, Dessole M, Cherchi PL. Cesarean section: to be or not to be, is this the question? Archives of Gynecology and Obstetrics. 2013 doi: 10.1007/s00404-013-2736-9. [DOI] [PubMed] [Google Scholar]