

Synopsis
The aim of this review was to summarize the findings of randomized controlled trials (RCTs) of progressive resistance strength training (PRT) by older people with osteoarthritis (OA). When data from 8 RCTs were synthesized using meta-analysis, a significant benefit from PRT was found on lower extremity extensor strength (standardized mean difference (SMD) 0.33, 95% confidence interval (CI) 0.12, 0.54), function (SMD 0.33, 95% CI 0.18) and pain reduction −0.35 (95% CI −0.52, −0.18). Across all three outcomes, the estimated effect size was moderate, which contrasted with trials of PRT in non-OA specific groups of older adults where a large effect was found on strength, but a small effect on function. This suggests that strength training has particularly strong functional benefits for older adults with OA. Older adults with osteoarthritis will benefit from a strength training program that provides progressive overload to maintain intensity throughout the exercise program. Clinicians should encourage participation in exercise training programs, even in the oldest old with OA.
Introduction
Muscle weakness is a common impairment in older adults, 1, 2 and osteoarthritis is one of the most frequently occurring chronic conditions in older people. 3 It therefore is not surprising that these conditions frequently co-exist in the elderly. Skeletal muscles produce all voluntary human movement. Changes in properties and performance of muscles can profoundly affect an older person’s ability to walk and function independently.4–6 Loss of muscle strength might be particularly problematic for an older person with OA who has pain, stiffness and mechanical changes to their joint that complicate their ability to mobilize and make them particularly vulnerable to small changes in their physical status.
Strength training has been the focus of a great deal of recent clinical research in many populations, including older adults and people with OA.7–13 While the benefits of strength training have been well explored in reviews focused on both populations, there has been little attention paid to the benefits and risks of strength training when undertaken by older people who have OA. In addition to being weaker, older people are more likely to have more advanced OA, including more severe pain and biomechanical changes to the joint which might change their response to exercise training.
Muscle Weakness in Older Adults
Most adults attain their peak muscle strength in their mid-twenties and maintain this level of strength relatively well until the sixth decade.14 By the age of eighty, strength declines on average to almost half that of a young adult.15 This decline in strength is consistent across muscle groups and all types of measurements – isometric strength (when the limb does not move), concentric strength (when the muscle shortens), eccentric strength (when a lengthening contraction occurs) and when strength is measured isokinetically (at a fixed speed).1, 16
In addition to a reduction in muscle strength, studies have shown enormous declines in muscle mass with age. One study found that the muscle mass of 80 year olds was 40% less than that of people in their twenties.17 The loss of muscle strength and mass that occurs with age was given the name ‘sarcopenia’ by Rosenberg in 1989, from the Greek “poverty of flesh”.18
The New Mexico Elder Health Survey, involving 883 people, is the most comprehensive study to date of the prevalence of sarcopenia in older people.19 This study defined sarcopenia as a loss of muscle mass of greater than two standard deviations (SD) below the mean appendicular muscle mass for healthy young adults. Among those aged 60 to 70 years, the prevalence of sarcopenia was about 17% for men and about 24% for women. Above the age of eighty, the figure rose to 53 to 58% for men and 43 to 60% for women. Although these findings need to be confirmed in other populations, the high prevalence of sarcopenia in this study suggests that sarcopenia is a common disorder among older people.
Muscle Weakness in OA
Muscle weakness, particularly of the knee extensors, is common in people with OA7, 20 and has been consistently shown to be associated with an increased risk of functional limitations and disability.20, 21 The Bristol Knee OA study found lower limb strength to be a stronger predictor of functional limitations than radiographic severity or knee pain.21
The nature of the cause –effect relationship between muscle weakness and OA is complex, and has been widely debated. While strength probably declines in people with OA as a secondary result of reduced activity, there is also evidence that muscle weakness directly contributes to the development and progression of OA.20 Muscle strength appears to have a protective effect against the disability associated with progressing OA. In a longitudinal study that monitored a cohort of women with for 6 years who had no functional limitations at baseline, knee extensor strength was protective against the development of functional limitations associated with OA.22
Benefits of Strength Training
In older adults, there is now strong evidence from randomized controlled clinical trials (RCTs) that even in the oldest old, muscle strength can be increased with a strength training program that uses a progressive overload.12, 13 There is also evidence that strength training improves mobility (i.e. increased gait speed), simple functional tasks (i.e. standing up from a chair) and self-rated daily function in older adults.13 However, while the effects of strength training are large, the impact on function and disability is much more modest.
There are also a large number of RCTs that support the benefits of exercise in general, and strength training in particular, in people with OA. Recent systematic reviews and guidelines have summarized the evidence for the effectiveness of strength training in people with osteoarthritis, and have found that strength training has a significant benefit in improving strength and function and in reducing pain.9–11 However, these reviews have also found that the reductions in pain and improvements in function are modest.
Strength Training by Older Adults with OA
While the positive benefits of strength training in the general population of older adults would suggest that it would be beneficial for older people with OA, there are reasons to think that this might not be the case. Because OA is a painful musculoskeletal condition, it is possible that strength training might cause stress on the joints which could exacerbate pain and result in decreased function and mobility. The biomechanical changes to the joint that occur with OA also have the potential to contribute to different responses to and risk factors from strength training.
No systematic review has focused specifically on strength training in older adults with OA. This review will explore the evidence from all identified randomized controlled trials (RCTs) of people with OA undertaking strength training to determine the strength of the evidence to answer several questions. These questions are:
Does strength training improve strength, function and reduce pain in older people with OA?
Are there differences in the effect of strength training in older adults with OA compared to the general population of older people?
There are other important questions about the benefits of strength training for older people with OA. Although there is inadequate data to allow a meta-analysis, the current evidence from randomized controlled trials will be explored to determine whether the design of the strength training program influences their response to strength training.
A. Systematic Review Methods
Criteria for Including Studies
This review includes only randomized controlled clinical trials (RCTs), which provide the highest level of evidence of treatment efficacy. Because the focus of this review is on older adults, only studies where the participants had a mean age of 65 or above in the overall group, or in the progressive resistance training (PRT) group, were included. This review did not include exercise programs in which there was not a treatment arm where the subjects received only PRT. Because of this criteria, all studies where the intervention group received exercise programs that combined different types of exercise training (e.g. aerobic and strength training) were excluded. This review also only included strength training programs that used progressive resistance strength training (PRT), because strength training programs that do not use this approach might be less effective. For this review, PRT was defined as strength training in which the overload increases during the training program to maintain or increase the intensity of the program.
Identifying Studies
To identify studies, we searched the Cochrane Bone, Joint and Muscle Trauma Group Specialised Register, the Cochrane Central Register of Controlled Trials, MEDLINE, EMBASE, CINAHL, SPORTDiscus, PEDro - The Physiotherapy Evidence Database and Digital Dissertations for all randomized controlled trials of strength training in older adults. Specific searches for osteoarthritis exercise trials were conducted. Reference lists from other reviews and guidelines that summarized the evidence for strength training by people with osteoarthritis were also reviewed. No language restrictions were applied.
The authors reviewed the titles, descriptors or abstracts identified from all literature searches to identify potentially relevant trials for full review. A copy of the full text of all trials that appeared to be potentially suitable for the review was obtained. The authors used previously defined inclusion criteria to select the trials. Data were extracted for lower extremity leg strength, pain and self-rated function outcomes. Information about the study methods, subject characteristics, exercise program, adverse events and exercise adherence were also recorded.
Data synthesis
When adequate data were provided for the outcomes of lower limb extensor strength, pain or function, the results from each study were entered into the database and combined. Data synthesis was carried out using MetaView in Review Manager version 5.0. Standardized units (i.e. standardized mean differences (SMD)) were created to allow the pooling of outcomes using different units and 95% confidence intervals (CI) were calculated. Random effects models were used for all analyses.
Meta-analysis Results
Summary of Included Studies
A total of 8 studies were included in this review (Table 1).23–30 Most studies that were not included in this review were excluded because the mean age was below 65 and/or the study included participants younger than 50; the exercise program included more types of exercises than PRT or the program was not a true progressive resistance training program.
Table 1.
Characteristics of included studies
| Study ID | Sample Size | Mean Age | Intervention | Control | Exercise Adheren ce | OA Group |
|---|---|---|---|---|---|---|
| Schilke 199629 | 20 | 65 | Type of Ex:1LL Equipment: isokinetic dynamometer Intensity: high Frequency: 3x pw Reps/Sets: 5/6 Duration: 8 weeks Setting: gym |
usual activities | Not reported(NR) | Knee OA |
| Ettinger 199724 | 295 (in PRT vs control) | 68 | Type of Ex: 4UL, 4LL, 1Tr Equipment: cuff-weights, dumb bells Intensity: moderate to high Frequency: 3x pw Reps/Sets: 12/2 Duration: 78 weeks Setting: facility-based group for 3 months, then home- based for 15 months |
health education program | 70% at 18 months | Knee OA |
| Maurer 199927 | 113 | 66.3 | Type of Ex: 1 LL Equipment: isokinetic dynamometer Intensity: high Frequency: 3x pw Reps/Sets: 3 reps at 3 speeds (total 9 reps) in 3 sets Duration: 8 weeks Setting: gym |
four classes on OA education and self-management | NR | Knee OA |
| Baker 200123 | 46 | 68 | Type of Ex: 2 functional exercises (squats and step-ups), 5 LL isotonic exercises Equipment: velcro ankle weights Intensity: initially low, progressed to hard Frequency: 3x pw Reps/ sets: 12/2 Duration: 16 weeks Setting: home-based |
given nutrition info, 7 home visits over 16 weeks, kept food logs 3/14 days | 84% | Knee OA |
| Topp 200230 | 35 | 65.6 | Type of Ex: 6 LL for 30 minutes Equipment: Theraband Intensity: mild fatigue after 8RM Frequency: 3x pw (2 at home 1 at gym) Reps/Sets: increasing reps and sets every week and then reached 12 reps/3sets at week 9 Duration: 16 weeks Setting: home and gym |
No intervention | NR | Knee OA |
| Foley 200325 | 70 | 69.8 | Type of Ex: 1UE/4 LL Equipment: weighted gaiters Intensity: 10 RM Frequency: 3x pw Reps/Sets: not reported Duration: 6 weeks Setting: gym |
telephone calls to record any changes in their condition | 75% | Hip or Knee OA |
| Mikesky 200628 | 221 | 69.4 | Type of Ex: 2UL/2LL Equipment: CYBEX machines at gym; Elastic bands at home, Intensity: 8–10 RM Frequency: 3x pw Duration: 1 year Setting: gym and home |
Flexibility exercise group: flexibility ex, 3x pw | 59% Gym 56% Home |
Knee OA |
| Lim 200826 – malaligned | 52 | 67.2 | Type of Ex: 5LL Equipment: theraband and cuff weights Intensity: 10 RM Frequency: 5x pw Reps/Sets: Initially 2 sets of 10 reps, progressed to 3 sets of 10 reps Duration: 12 weeks Setting: gym and home |
No intervention | 89% | Medial knee OA |
| Lim 200826 - neutral | 55 | 64.1 | Same program as above | No intervention | 86% | Medial knee OA |
Note: Ex=exercise, LL= lower limb, UL=upper limb, Tr=trunk, x pw= times per week, reps=repetitions, PRT= progressive resistance training
All of the studies focused on people with knee OA, with one study including people with both hip and knee OA.25 The size of the studies ranged from 20 to 295 people.
The number of exercises that were included in the program varied from 1 exercise to 9. Most of the exercise programs were conducted at a moderate to high intensity. All of the programs had participants exercise 3 times per week, except in the study by Lim et al,26 where people exercised 5 times per week. The duration of the programs ranged from 6 to 72 weeks. In 3 studies participants exercised only in a gym setting, 1 study used only home-based training and 4 studies used a combination of home-based and gym-based training. A wide variety of equipment was used, including therabands, cuff weights and isokinetic dynamometers.
In the study by Lim et al, 26 the subjects were divided the subjects into two groups prior to randomization, people with neutral knee alignment and people with more varus malalignment. Because these groups were separately randomized, they were treated as two different studies for the purpose of the meta-analysis.
Effect of Strength Training on Strength and Function in Older People with OA
Progressive resistance strength training improves strength in older adults with OA. The effect size for the impact that strength training has on leg extensor muscle strength of older adults with OA was moderate and the effect was statistically significant (Figure 1), with a SMD of 0.33 (95% Confidence Interval (CI) 0.12, 0.54).
Figure 1. Forest plot of leg extensor strength in trials of strength training by older adults with OA.
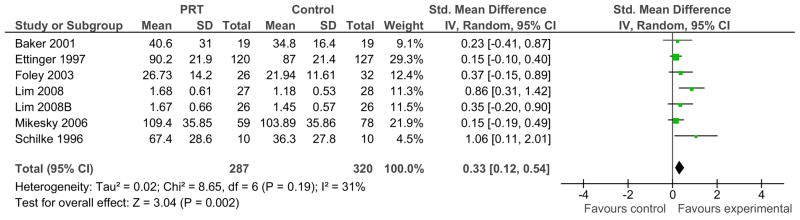
Note: PRT= progressive resistance training, sd=standard deviation, CI= confidence interval
Mean and SD are based on the final scores for each outcome measure in the PRT and control groups. Total refers to the sample size in each group for each outcome. The sample size is used to weight the contribution of each study to the overall estimate of treatment effect. The total standardized mean difference indicates what the overall effect size and the associated confidence interval is for this estimate. The test of statistical significance is provided by the test for overall effect and the associated P-value which is shown to the far left of the figure.
This review also found that strength training significantly improves function in older people with OA (Figure 2). The effect of strength training on function was almost identical to the effect size found for strength, with a SMD 0.33 (95% CI 0.18, 0.49), which is statistically significant.
Figure 2. Forest plot of function in trials of strength training by older adults with OA.
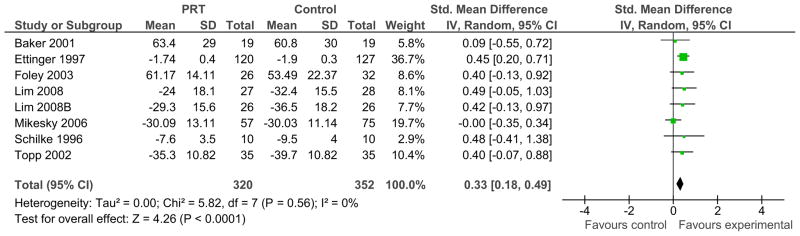
Note: PRT= progressive resistance training, sd=standard deviation, CI= confidence interval
Pain decreased in people who participated in PRT. This effect was negative, indicating a reduction in pain, with a SMD of −0.35 (95% CI −0.52, −0.18).
Comparison of Outcomes between Older People with and Without OA
To compare the effects of strength training on older people with and without OA, newly identified trials were added to a database that included all previously identified trials of PRT in older people. As described elsewhere, this database includes trials of healthy older adults, as well as older people with a variety of medical conditions.13
These analyses found that the studies of older adults that were not specifically focused on older people with OA had a much larger effect on strength than the OA-specific studies. (Table 2) When the studies OA-specific studies were excluded, the effect size for strength was 0.88 (95% CI 0.7, 1.05), which is significantly lower than the strength estimate for older people with OA.
Table 2.
Comparison of strength and functional outcomes between older adults with and without OA
| Outcome | Comparison | N | Effect Size (95% CI |
|---|---|---|---|
| Strength | |||
| All older adults | 3166 | 0.83 (0.67,0.98) | |
| Excluding OA-specific studies | 2559 | 0.88 (0.7, 1.05) | |
| Including only OA-specific studies | 607 | 0.33 (0.12, 0.54) | |
| Function | |||
| All older adults | 2279 | 0.15 (0.07, 0.23) | |
| Excluding OA-specific studies | 1607 | 0.07 (−0.02, 0.17) | |
| Including only OA-specific studies | 672 | 0.33 (0.18, 0.49) |
In contrast, the studies of strength training in the general population of older people had only a small effect on function (Table 2). In fact, when the OA-specific studies were removed from the analysis, the effect of strength training on function was no longer statistically significant with an effect size of 0.07 (−0.02, 0.17)). In contrast, the OA-specific studies had a moderate effect on function, which was significantly different from the small functional effect in the non-OA specific studies.
B. Design of Training Programs
From a clinical perspective, questions about the optimal design of a strength training program are important. There are fewer studies that have randomized comparisons of different strength training approaches in older adults with OA, so meta-analytic comparisons are not possible. Two studies with randomized comparisons of different strength training approaches are summarized below. Because so few studies exist in this area, the search was broadened to include studies where the mean age of participants was 60 or above.
High versus low-moderate intensity Strength Training
There has been debate about the most appropriate exercise intensity for strength training programs for people with OA. Larger training effects are usually seen when people participate in high-intensity strength training, but there is concern that a large overload might increase pain and joint stress in people with OA. Jan et al,31 conducted an RCT that compared high intensity and low intensity training in people with knee OA. The authors stated in the text that their original intent had been to have people exercising at an intensity of 80% of 1repetition maximum (1RM), but they found in pilot testing that 7/10 subjects were unable to complete the exercises at this intensity because of pain. Therefore, high intensity training was conducted at 60% of 1RM with 3 sets of 8 repetitions and low intensity training was set at 10% 1RM with 10 sets of 15 repetitions. After 8 weeks of training, both exercise groups had significantly reduced pain and improved function compared to the control group, but there were no significant differences in these outcomes between the high and low intensity training groups. No adverse events were reported.
Dynamic versus Isometric Resistance Training
Topp et al.30 compared a dynamic resistance training program where the exercises were performed through the range of motion using theraband to an isometric training program where the joint did not move as the subjects generated muscle tension against the maximum-resistance theraband while the joint angle did not change. After 16 weeks of training, both groups had improvements in function and pain compared to the control group, but the improvements were not significantly different between the two treatment groups.
Discussion
This review found that strength training is beneficial to older people with OA. Older adults in the strength training group had significant improvements in strength and function, and reductions in pain in the older adults. All of these outcomes had a moderate effect size.
These findings are consistent with what is known about the effect of strength training in the general older adult population and in the general population of people with OA, where strength training has been found to improve muscle strength and function.11, 13, 23 The effect on strength was smaller than that found by Fransen in the Cochrane review of knee OA which found an effect size of 0.53 (95% CI 0.79, 0.27), although the confidence intervals overlap.9 It is not clear why the results were different in this review. It is possible that the studies that included younger people with OA were more likely to use the highest intensity of training or had other differences in the program, but such differences in the training programs are not apparent in the study descriptions. It is also possible that the older people’s muscles were slightly less responsive overall or slower to respond to the training stimulus. Finally, it is possible that adherence to the exercise program was lower in older people with OA, but this can not be confirmed because adherence was poorly recorded or not recorded at all in many of these trials.
An interesting finding from this review was the difference in the magnitude of the effect on strength and function between studies with a general older adult population and OA-specific studies of older people. In the general older adult population, strength training has a very large effect on strength, and a much smaller, barely significant, effect on function. This is perhaps not surprising, since the intervention is targeting muscle and so the direct impact is on strength, while many factors can contribute to late-life functional problems. In OA, the effect on strength, function and pain was a moderate size, and almost an identical effect size across the three outcomes. These findings suggest that while strength training is beneficial for all older adults, it has a much larger functional impact on people with OA, and all of the improvements in muscle strength are directly translated into improvements in function. One reason for this could be that the impairments that limit function in older people with OA are more narrowly focused, and muscle weakness is a primary contributor to pain and functional problems in OA. When older people with OA participate in strength training the training directly targets one of the main barriers to their functional performance.
It is not clear why the strength gains in people with OA were smaller than those in the general older adult population. Given the larger strength gains observed in the general older adults studies, it would appear that larger strength gains are possible to achieve in older adults exercisers. It is possible that if strength gains could be increased in older people with OA, perhaps by changes to the type, intensity or duration of training, or by ensuring maximal adherence to the training, there might also be additional improvements in function and reductions in pain beyond the moderate effects currently seen.
A major limitation of this review is the fact that no appropriate RCTs were identified that explored the effects of strength training on older adults with hip or upper limb OA. Any studies that were identified could not be included because they focused on a younger population, did not use an RCT design or used either combined exercise training or a non-PRT approach. Studies in these groups of OA patients are clearly needed.
There is also very limited randomized data available about the comparative effectiveness of different strength programs or even the relative effectiveness of different training approaches. The existing evidence suggests that there are few differences in outcomes when different training approaches are used. In particular, Jan et al found no significant differences in strength and functional outcomes between high and low intensity training groups. However, caution is needed in interpreting these findings because the studies comparing training intensity or approaches have all had a short duration of follow-up so true training effects might not have occurred. They also have small sample sizes, and therefore might have failed to detect real differences that exist between the treatment groups because of a lack of statistical power.
The positive message from this review that should be clearly communicated to older people with OA is that no matter how old they are, they will probably benefit in clinically important ways from participating in a strength training program, as long as it provides some consistent overload to their muscles as they exercise. The biggest challenge with any exercise program is to maintain long-term adherence, because the benefits of exercise will diminish if people stop exercising. There is currently no evidence that one type of strength training program is superior to another as long as the program provides progressive overload, so older people should exercise at the intensity, location and using the equipment that they most prefer. Although not the focus of this review, aerobic training programs have been found to have a similar benefit to strength training in an RCT that had one of the largest sample sizes and longest follow-up of any trials in this area.24 If people prefer aerobic exercise, this mode of exercise should also be utilized by older people with OA.
Summary and Recommendations
Older adults with osteoarthritis will benefit from a strength training program that provides progressive overload to maintain intensity throughout the exercise program. Significant improvements in strength and function and pain reduction were seen when the data from 8 RCTs were synthesized, and there was a moderate effect size for all three outcomes.
Clinicians should encourage participation in exercise training programs, even in the oldest old with OA. There is no evidence that there is significantly decreased efficacy or increased risk of adverse events when older adults with OA participate in exercise programs compared to younger adults. People with OA should be reassured that it is unlikely to exacerbate their pain if performed using the appropriate methods and at the appropriate dose. In fact, the evidence suggests that it will decrease pain in most older people.
More information is needed about the comparative effectiveness of different training approaches. Specifically, trials with adequate sample size and duration of follow up are needed to comparing the effectiveness of different training intensities and types of strength training approaches. However, the current evidence suggests people can benefit from a wide variety of exercise programs, as long as the strength training program provides a progressive overload. Older people with OA should therefore select the type and style of strength training that best fits into their lifestyle. Long-term adherence is required in order to maintain the benefits of strength training, and studies to increase our understanding of the best way to achieve long-term compliance with exercise programs in this population would be very useful.
Finally, more evidence is needed about the benefits of strength training for older people with OA of the hip and upper limb. The current findings are almost completely based on studies of people with knee OA.
Figure 3. Forest plot of pain in trials of strength training by older adults with OA.

Note: PRT= progressive resistance training, sd=standard deviation, CI= confidence interval
Acknowledgments
The authors wish to acknowledge the contributions of Craig Anderson, Derrick Bennett and Caroline Stretton who were involved in the first Cochrane systematic review of strength training in older adults. They also wish to thank Kira Wilke and Amy Vertal for their assistance in the preparation of this manuscript. Dr. Latham was supported by the Boston Pepper Center Research Career and Development Core which is funded through the National Institute of Health.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Nancy Latham, Email: nlatham@bu.edu, Health and Disability Research Institute, Boston University School of Public Health, 5TW, 715 Albany St, Boston, MA, Phone: 617-638-1988, Fax: 617-638-1999.
Chiung-ju Liu, Email: liu41@iupui.edu, Department of Occupational Therapy, School of Health and Rehabilitation Sciences, Indiana University at Indianapolis, 1140 West Michigan St, CF 303, Indianapolis, Indiana 46202, Phone: 317 274-8006, Fax: 317 274-2150.
References
- 1.Vandervoort A. Effects of ageing on human neuromuscular function: implications for exercise. Canadian Journal of Sports Science. 1992;17(3):178–184. [PubMed] [Google Scholar]
- 2.Brooks SV, Faulkner JA. Skeletal muscle weakness in old age: underlying mechanisms. Medicine & Science in Sports & Exercise. 1994;26(4):432–439. [PubMed] [Google Scholar]
- 3.Seeman TE, Merkin SS, Crimmins EM, Karlamangla AS. Disability trends amoung older Americans: National Health and Nutrition Examination surveys, 1988–1994 and 1999–2004. Am J Public Health. 2010;100:100–107. doi: 10.2105/AJPH.2008.157388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Buchner DM, de Lateur BJ. The importance of skeletal muscle strength to physical function in older adults. Annals of Behavioural Medicine. 1991;13:91–98. [Google Scholar]
- 5.Buchner DM, Larson EB, Wagner EH, Koepsell TD, De Lateur BJ. Evidence for a nonlinear relationship between leg strength and gait speed. Age Ageing. 1996;25:386–391. doi: 10.1093/ageing/25.5.386. [DOI] [PubMed] [Google Scholar]
- 6.Jette A, Assmann S, Rooks D, Harris B, Crawford S. Interrelationships among disablement concepts. Journal of Gerontology: Medical Sciences. 1998;53A(5):M395–M404. doi: 10.1093/gerona/53a.5.m395. [DOI] [PubMed] [Google Scholar]
- 7.Baker K, McAlindon T. Exercise for knee osteoarthritis. Curr Opin Rheumatol. 2000;12:456–463. doi: 10.1097/00002281-200009000-00020. [DOI] [PubMed] [Google Scholar]
- 8.Fiatarone Singh MA. Exercise comes of age: rationale and recommendations for a geriatric exercise prescription. J Gerontol A Biol Sci Med Sci. 2002;57(5):M262–282. doi: 10.1093/gerona/57.5.m262. [DOI] [PubMed] [Google Scholar]
- 9.Fransen M, McConnell S. Exercise for osteoarthritis of the knee. Cochrane Database of Systematic Reviews. 2008;(4) doi: 10.1002/14651858.CD004376.pub2. [DOI] [PubMed] [Google Scholar]
- 10.Fransen M, McConnell S, Bell M. Exercise for osteoarthritis of the hip or knee. Cochrane Database of Systematic Reviews. 2003;(3):CD004286. doi: 10.1002/14651858.CD004286. [DOI] [PubMed] [Google Scholar]
- 11.Lange AK, Vanwanseele B, Fiatarone singh MA. Strength training for treatment of osteoarthritis of the knee: A systematic review. Arthritis Care & Research. 2008;59(10):1488–1494. doi: 10.1002/art.24118. [DOI] [PubMed] [Google Scholar]
- 12.Latham N, Bennet DA, Stretton CM, Anderson CS. A Systematic Review of Progressive Resistance Strength Training in Older Adults. Journal of Gerontology: Medical Sciences 2004. 2004;59(1):48–61. doi: 10.1093/gerona/59.1.m48. [DOI] [PubMed] [Google Scholar]
- 13.Liu CJ, Latham NK. Progressive resistance strength training for improving physical function in older adults. Cochrane Database of Systematic Reviews. 2009:3. doi: 10.1002/14651858.CD002759.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lindle RS, Metter EJ, Lynch NA, et al. Age and gender comparisons of muscle strength in 654 women and men aged 20–93 yr. Journal of Applied Physiology. 1997;83(5):1581–1587. doi: 10.1152/jappl.1997.83.5.1581. [DOI] [PubMed] [Google Scholar]
- 15.Doherty T, Vandervoort A, Brown W. Effects of ageing on the motor unit: a brief review. Canadian Journal of Applied Physiology. 1993;18(4):331–358. doi: 10.1139/h93-029. [DOI] [PubMed] [Google Scholar]
- 16.Hughes VA, Frontera WR, Wood M, et al. Longitudinal muscle strength changes in older adults: influence of muscle mass, physical activity and health. Journal of Gerontolgy: Biological Sciences. 2001;56A(5):B209–B217. doi: 10.1093/gerona/56.5.b209. [DOI] [PubMed] [Google Scholar]
- 17.Lexell J, Taylor CC, Sjostrom M. What is the cause of the ageing atrophy? Total number, size and proportion of different fiber types studied in whole vastus lateralis muscle from 15- to 83-year-old men. Journal of the Neurological Sciences. 1988;84(2–3):275–294. doi: 10.1016/0022-510x(88)90132-3. [DOI] [PubMed] [Google Scholar]
- 18.Rosenberg IH. Summary Comments. American Journal of Clinical Nutrition. 1989;50:1231–1233. [Google Scholar]
- 19.Baumgartner RN, Koehler KM, Gallagher D, et al. Epidemiology of sarcopenia among the elderly in New Mexico. Am J Epidemiol. 1998;147(8):755–763. doi: 10.1093/oxfordjournals.aje.a009520. [DOI] [PubMed] [Google Scholar]
- 20.Slemenda C, Brandt KD, Heilman DK, et al. Quadriceps weakness and osteoarthritis of the knee. Ann Intern Med. 1997;127:97–104. doi: 10.7326/0003-4819-127-2-199707150-00001. [DOI] [PubMed] [Google Scholar]
- 21.McAlindon TE, Cooper AC, Kirwan JR, Dieppe PA. Determinents of disability in osteoarthritis of the knee. Ann Rheum Dis. 1993;52:258–262. doi: 10.1136/ard.52.4.258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ling SM, Xue QL, Simonsick EM, et al. Transitions to mobility difficulty associated with lower extremity osteoarthritis in high functioning older women: Longitudinal data from the Women’s Health and Aging Study II. Arth Rheum. 2006;55:256–263. doi: 10.1002/art.21858. [DOI] [PubMed] [Google Scholar]
- 23.Baker KR, Nelson ME, Felson DT, Layne JE, Sarno R, Roubenoff R. The efficacy of home based progressive strength training in older adults with knee osteoarthritis: A randomized controlled trial. J Rheumatol. 2001;28(7):1655–1665. [PubMed] [Google Scholar]
- 24.Ettinger WH, Jr, Burns R, Messier SP, et al. A randomized trial comparing aerobic exercise and resistance exercise with a health education program in older adults with knee osteoarthritis. The Fitness Arthritis and Seniors Trial (FAST) JAMA. 1997;277:25–31. [PubMed] [Google Scholar]
- 25.Foley A, Halbert J, Hewitt T, Crotty M. Does hydrotherapy improve strength and physical function in patients with osteoarthritis - A randomised controlled trial comparing a gym based and a hydrotherapy based strengthening programme. Ann Rheum Dis. 2003;62 (12):1162–1167. doi: 10.1136/ard.2002.005272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Lim BW, Hinman RS, Wrigley TV, Sharma L, Bennell KL. Does knee malalignment mediate the effects of quadriceps strengthening on knee adduction moment, pain and function in medial knee osteoarthritis? A randomized controlled trial. Arth Rheum. 2008;59:943–951. doi: 10.1002/art.23823. [DOI] [PubMed] [Google Scholar]
- 27.Maurer BT, Stern AG, Kinossian B, Cook KD, Schumacher HR. Osteoarthritis of the knee: isokinetic quadriceps exercise versus an educational intervention. Arch Phys Med Rehabil. 1999;80(10):1293–1299. doi: 10.1016/s0003-9993(99)90032-1. [DOI] [PubMed] [Google Scholar]
- 28.Mikesky A, Mazzuca S, Brandt K, Perkins S, Damush T, Lane K. Effects of strength training on the incidence and progression of knee osteoarthritis. Arthritis Care & Research. 2006;55(5):690–699. doi: 10.1002/art.22245. [DOI] [PubMed] [Google Scholar]
- 29.Schilke JM, Johnson GO, Housh TJ, O’ Dell JR. Effects of muscle-strength training on the functional status of patients with osteoarthritis of the knee joint. Nurs Res. 1996;45(2):68–72. doi: 10.1097/00006199-199603000-00002. [DOI] [PubMed] [Google Scholar]
- 30.Topp R, Woolley S, Hornyak J, Khuder S, Kahaleh B. The effect of dynamic versus isometric resistance training on pain and functioning among adults with osteoarthritis of the knee. Arch Phys Med Rehabil. 2002;83(9):1187–1195. doi: 10.1053/apmr.2002.33988. [DOI] [PubMed] [Google Scholar]
- 31.Jan MH, Lin JJ, Liau JJ, Lin YF, Lin DH. Investigation of the clinical effects of high- and low-resistance trainign for patients with knee osteoarthritis: A randomized controlled trial. Phys Ther. 2008;88:427–436. doi: 10.2522/ptj.20060300. [DOI] [PubMed] [Google Scholar]