

This review presents an overview of breast cancer care, burden, and outcomes in Latin America, as well as the challenges and opportunities for improvement. The burden of breast cancer in the region may be growing because of demographic changes and socioeconomic development. Early diagnosis and population-wide access to evidence-based treatment are ongoing concerns.
Keywords: Breast cancer, Latin America, Burden, Treatment, Outcomes, Access
Learning Objectives
Describe associations between epidemiologic factors and breast cancer risk in the countries included in this review.
Compare presentation profiles among the countries studied and discuss implications for outcomes.
Abstract
This review presents an overview of breast cancer care, burden, and outcomes in Latin America, as well as the challenges and opportunities for improvement. Information was gleaned through a review of the literature, public databases, and conference presentations, in addition to a survey of clinical experts and patient organizations from the region. Breast cancer annual incidence (114,900 cases) and mortality (37,000 deaths) are the highest of all women's cancers in Latin America, and they are increasing. Twice as many breast cancer deaths are expected by 2030. In Peru, Mexico, Colombia, and Brazil, diagnosis and death at younger ages deprives society of numerous productive years, as does high disease occurrence in Argentina and Uruguay. Approximately 30%–40% of diagnoses are metastatic disease. High mortality-to-incidence ratios (MIRs) in Latin America indicate poor survival, partly because of the late stage at diagnosis and poorer access to treatment. Between 2002 and 2008, MIRs decreased in all countries, albeit unevenly. Costa Rica's change in MIR outpaced incidence growth, indicating impressive progress in breast cancer survival. The situation is similar, although to a lesser extent, in Colombia and Ecuador. The marginal drops of MIRs in Brazil and Mexico mainly reflect incidence growth rather than progress in outcomes. Panama's MIR is still high. Epidemiological data are scattered and of varying quality in Latin America. However, one could ascertain that the burden of breast cancer in the region is considerable and growing due to demographic changes, particularly the aging population, and socioeconomic development. Early diagnosis and population-wide access to evidence-based treatment remain unresolved problems, despite progress achieved by some countries.
Implications for Practice:
Breast cancer imposes a heavy epidemiological, clinical, and economic burden on Latin American societies, and the situation will only worsen in the foreseeable future. Physicians and decision makers alike need to prepare to provide better care to more women as incidence of the disease grows and health care coverage expands. The main challenges to be addressed are barriers to early diagnosis and access to evidence-based treatment alternatives in a multidisciplinary way. Because breast cancer in Latin America affects women at younger ages than in Europe or North America and frequent population-based mammographic screening is not a reality, raising awareness is everyone's job, from the general practitioners to the oncologists, from the non-governmental organizations to the policy makers, from every woman to every man.
Introduction
The burden of breast cancer, as well as the management and organization of breast cancer care in 18 countries, was presented recently in the Global Breast Cancer Report [1]. Breast cancer is the most common form of cancer in women; with 5.2 million survivors (5 years following diagnosis), it remains the most prevalent cancer in the world. In 2008, a total of 1.38 million new breast cancer cases were diagnosed, representing 23% of all cancers [2]. The difference in incidence rates between developed and developing countries is still remarkable. Age-standardized incidence rates in Western Europe are still almost 5 times higher than those in Eastern Africa (89.9 per 100,000 woman compared with 19.3 per 100,000). Latin America and the Caribbean are ranked in the middle, with an age-standardized incidence rate of 40 per 100,000 women [2]. As documented in the literature, a mixture of demographic, hereditary, economic, environmental, and lifestyle risk factors account for this variability [3]. However, differences in the capacity of a country's health system for detection and diagnosis, as well as case and death registration, also affect the disease burden.
This report reviews the burden of breast cancer and breast cancer care and outcomes in Latin American countries, focusing on those countries that had available information for this study: Argentina, Brazil, Chile, Colombia, Costa Rica, Ecuador, Mexico, Panama, Peru, Uruguay, and Venezuela.
Materials and Methods
Multiple sources of information were used for this report, including a review of the literature and public databases, a survey completed by clinical experts and patient organizations from the 11 Latin American countries, and epidemiological data from the Pan American Health Organization (PAHO) and the International Agency for Research on Cancer. The literature review was conducted in Medline, Literatura Latinoamericana en Ciencias de la Salud, and the Scientific Electronic Library Online between December 2001 and December 2011 using the terms: (breast OR mama) AND cancer AND (Argentina OR Brazil OR Chile OR Colombia OR [Costa AND Rica] OR Ecuador OR Mexico OR Peru OR Uruguay OR Venezuela); combined with each of the following strings: (inciden* OR prevalen* OR mortality OR survival OR “quality of life” OR [stage AND diagnosis]) OR (age OR parity OR [first AND {pregnan* OR child OR birth}]) OR menarche OR breastfeed* OR contraceptive* OR menopause OR (reproductive AND [life OR health]) OR obes* OR Cost* OR dollar* peso* OR real* OR absenteeism OR presenteeism OR (productivity AND loss) OR spen* OR ([treatment AND {practice OR pattern} OR management OR guideline* OR program OR “care pathway*” OR “service configuration” OR [{specialist OR quality}] AND care]). The review also included a search of the grey literature, targeting data and information on epidemiology and outcomes of breast cancer in the region, as well as treatment guidelines, cancer control plans, and additional documentation on the social and economic burden of breast cancer.
A structured survey, developed for the Global Breast Cancer Report [1], was conducted with two oncologists from each study country, as well as a number of patient organizations. Their responses to the survey were used to complement and validate the findings from the literature review and the analyses of the different databases. Information and data were also provided by the PAHO, the American Cancer Society (ACS) and the Latin American and Caribbean Society of Medical Oncology and extracted from a variety of secondary sources and multinational databases.
Epidemiological and Social Burden
Breast cancer is the most common form of cancer in women worldwide, and Latin America is no exception. An estimated 114,900 women are diagnosed every year, and 37,000 die of the disease in the region [2]. The large variability in incidence and mortality within the region is shown in Figure 1. Incidence seems to cluster geographically, with the northern countries of Latin America (Mexico, Panama, Ecuador, Colombia) presenting with a lower incidence that is comparable to Asia and Africa and slightly lower than Central and Eastern Europe; the high incidence in the south of Latin America (Uruguay, Argentina, Chile) is similar to that of Europe or the U.S. Costa Rica, with its high incidence, appears as an exception. This is probably due to the demographic structure of the country, which is similar to that of the southern cone rather than Central America.
Figure 1.

Breast cancer incidence and mortality in Latin America and other regions. Adapted from [2] with permission.
Abbreviations: ASR, age-standardized rate; CEE, Central and Eastern Europe; LAC, Latin America and the Caribbean; Eur, Europe; US, United States.
Mortality in the region is also dissimilar. Driven by the high incidence, mortality rates in Argentina and Uruguay are very high and surpass those of the countries with the highest incidence in Europe and the U.S. The other Latin American countries converge around 10–13 deaths per 100,000 women, which is not significantly lower than in Southern Europe, Oceania, or the U.S., where incidence is much higher.
Breast cancer incidence and mortality have been increasing steadily in the region throughout the past 25–30 years [4]. For example, Brazil's incidence rate has tripled in 15 years; it is estimated that the crude breast cancer incidence rate in the state of Goiás in Brazil has increased at an average of 7.6% compound annual growth rate (CAGR): from 22.9 per 100,000 in 1988 to 68.2 per 100,000 in 2003 [5]. Similarly, Chile's Ministry of Health reports that the crude incidence rate has been growing at an average of 10.7% CAGR: from 28.9 per 100,000 in 2000 to 39.2 per 100,000 in 2003 [6]. Costa Rica's incidence has also been increasing steadily since the mid-1990s at an average of 5.1% CAGR: from 23.64 per 100,000 in 1995 to 35.2 per 100,000 in 2003 [7]. In contrast, Uruguay's incidence seems to have stabilized, according to the data published by the National Cancer Registry. Between 1996 and 1997, an averaged total of 1,730 annual new cases were reported [8], and between 2002 and 2006, an averaged total of 1,760 annual new cases were reported [9], representing incidence rates of 106 and 105 per 100,000 women, respectively.
Risk factors that may affect breast cancer incidence in different countries have been investigated in several studies [10–19]. The most relevant risk factors include demographic, socioeconomic, genetic, and lifestyle-related risk factors, as well as reproductive behavior. To explore the association between risk factors and breast cancer incidence in different Latin American countries, we collected a series of variables that correspond to these factors in the countries considered in the study and evaluated the linear correlation between each of them and GLOBOCAN 2008 age-standardized incidence rates [2]. Table 1 shows the resulting pairwise correlation coefficients of breast cancer incidence and each risk factor. The main contributing factor to breast cancer incidence remains age. The associations of education and wealth with breast cancer occurrence are also statistically significant, while reproductive and lifestyle-related risk factors are not significant. However, because women in different socioeconomic strata from the countries under study are exposed differently to these risk factors, this correlation may not be best measured at a country level.
Table 1.
Pairwise correlation coefficients between breast cancer incidence [2] and risk factors in Latin American countries
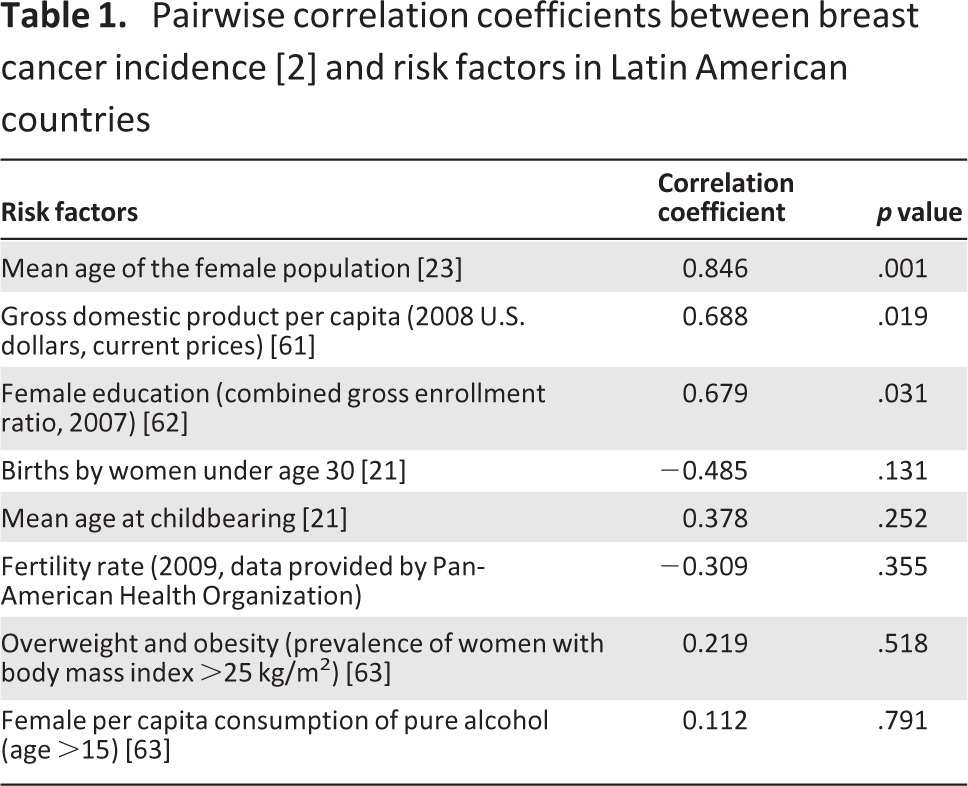
The population level and fertility rates are inversely associated with breast cancer incidence in Latin America [20]. Because fertility has been decreasing steadily in all of the countries included in the study [21], breast cancer incidence is expected to increase. Several studies considered the impact of diet on the incidence of breast cancer in Latin America. A review of the literature by Torres-Sánchez et al. concluded that the evidence of the impact of specific foods and nutrients on the incidence of the disease in the region is inconclusive [22].
Demographic changes in the region are creating an epidemiological transition, as most Latin American countries are shifting to an older population age structure. Today, 10.5% of the population of Argentina and 13.9% of the population of Uruguay are 65 years and older, whereas in Mexico and Brazil only 6.6% and 6.9% of the population are 65 years and older, respectively. The Demographic Observatory published by the Latin American and Caribbean Demographic Center forecasts that by 2050 people 65 years and older will represent 19% of the population in Argentina, 21% in Uruguay, 21.4% in Mexico, and 22.6% in Brazil [23]. The number of women aged 60 and older will double by 2030, thus significantly increasing the number of cases of breast cancer. The World Health Organization (WHO) estimated that the number of deaths from breast cancer in Latin America is expected to double by 2030 to 73,542, twice as many as in 2008 [24].
Breast cancer has the highest mortality among women's cancers in Latin America, accounting for 14% of all cancer deaths [25]. As shown in Figure 1, Colombia, Ecuador, Mexico, and Peru have very similar age-adjusted mortality rates (around 10 per 100,000), followed by Chile and Panama (11 per 100,000), Costa Rica and Brazil (12 per 100,000), Venezuela (13 per 100,000), and as a result of their higher incidence rates, Argentina (20 per 100,000) and Uruguay (24 per 100,000). The variability within the region is much less than that registered in the incidence estimates. Unlike in Europe and North America, breast cancer mortality is still on the rise in Latin America, with very few exceptions. This is confirmed by numerous country specific studies and reports [8, 9, 26–30] and by the WHO [24].
The social burden of breast cancer can be described in terms of disability-adjusted life years (DALYs) per 100,000 women. This indicates the years of potential life lost to premature mortality, as well as years of full health lost to disability. Figure 2 presents the lost DALYs from breast cancer, from relevant WHO regions. The overall social burden of breast cancer is highest in developed countries, where incidence rates are highest. However, the proportion of losses due to mortality is greater in Latin America.
Figure 2.
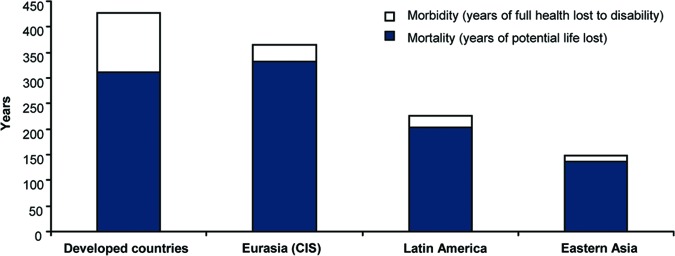
Burden of breast cancer in different regions: disability-adjusted life years lost. Adapted from [24] with permission.
Abbreviation: CIS, Commonwealth of Independent States.
Table 2 shows WHO's estimates of the DALYs lost due to breast cancer in Latin American countries [24] in correlation with age at diagnosis and age of death. A total of 613,000 DALYs are lost in Latin American countries due to breast cancer, with great variability within the region. The countries with the highest number of breast cancer cases (Argentina and Uruguay) display the highest rates of DALYs lost. Up to 3% of the total DALYs lost in the female populations of Uruguay and Argentina are due to breast cancer, which is between two and three times higher than in any of the seven countries with lower incidence, such as Ecuador, Colombia, and Mexico.
Table 2.
Estimates of the burden of breast cancer in 2004 [24] and women's mean age at diagnosis and death from breast cancer [2] in Latin American countries
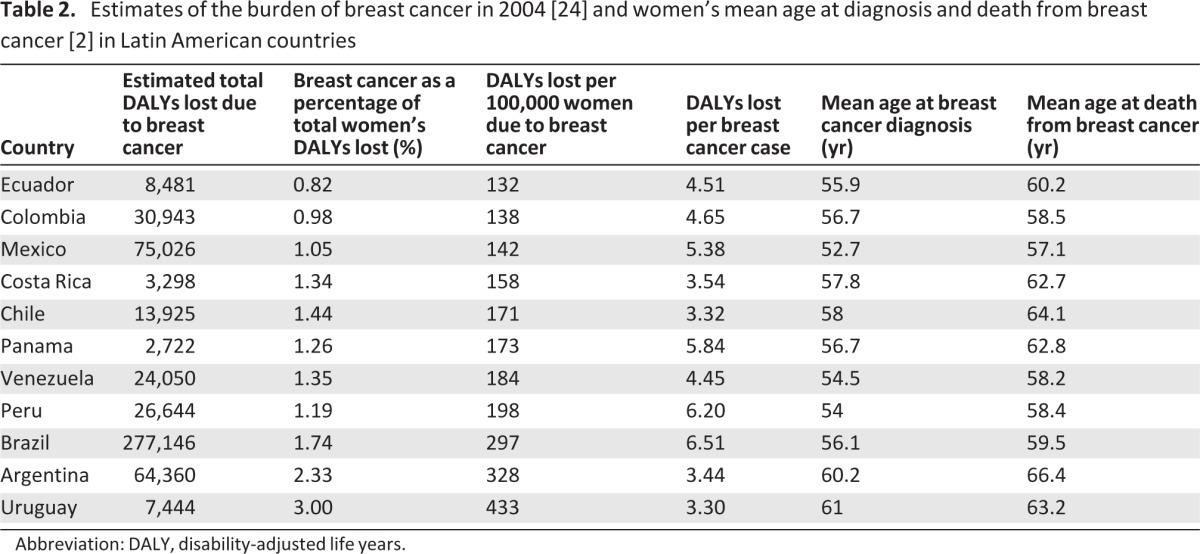
Abbreviation: DALY, disability-adjusted life years.
Different aspects seem to influence social burden of disease in Latin American countries. In Argentina and Uruguay, high breast cancer incidence results in a heavy burden on society, whereas young age at diagnosis and death are the cause in Brazil, Peru, and Mexico (Table 2). In Brazil, in spite of the relatively low breast cancer incidence, the DALYs lost per 100,000 women are nearly double that of most countries in the region. The high and increasing breast cancer mortality in Brazil, paired with the fact that both incidence and mortality among young women (<40 years old) have been reported to be on the rise [5, 31], may account for the DALYs lost. If more women of working age are being diagnosed, more productive years are being lost. Similarly, in Mexico, productivity losses due to young age at death are exacerbated by the increased morbidity due to young age at diagnosis.
Chile and Costa Rica have moderate DALYs lost (Table 2) because of the more moderate breast cancer incidence rates and age distribution, which is between that of Mexico and Uruguay. However, in Uruguay as in Chile, this situation is changing over time. Chile's mean age of patients diagnosed was 57.6 years in 2000 and 59.2 years in 2003, whereas the age in Uruguay increased from 62.8 years in 1996–1997 [8] to 64 years in 2002–2006 [9]. It can be expected that the social burden of breast cancer will increase rapidly in the countries with younger populations as life expectancies improve and lifestyles change. Aging populations, in countries like Mexico and Brazil, may lower the average DALYs lost per breast cancer case because of an older age at diagnosis and death. However, this factor will certainly increase the absolute number of DALYs lost due to breast cancer as incidence approaches the rates of Argentina or Uruguay.
Clinical Burden
The long-term prognosis for patients with breast cancer has improved significantly over the past 50 years. Benchmark countries in Europe and North America achieve 5-year survival rates greater than 80% [32]. This progress is explained by the combination of positive developments with enhanced treatment and earlier diagnosis. Regarding enhanced treatment, it has been estimated that the introduction of adjuvant systemic chemotherapy, endocrine therapy, and biologic therapy account for a 25% increase in overall survival rate and an almost 50% increased survival rate in women younger than 70 years of age [33]. As for earlier diagnosis, the largest improvements in outcome have been seen during the last 20–30 years. This improvement is mainly due to the introduction of population-based mammography screening, which has led to earlier diagnosis.
Data concerning Latin American countries are partial and fragmented. A lack of cancer registries also affects the assessment of breast cancer care outcomes. However, the few reliable estimations indicate that 5-year survival in Latin America is approximately 70% [34–39], which is considerably less than Northern Europe, France, Italy, Spain, North America, Japan, and Australia. This rate is also below Central European countries, such as Poland and Slovenia, which are reaching 75% 5-year overall survival [1].
Stage at diagnosis is an important predictor for overall survival in breast cancer. A number of studies from Latin American countries have been published showing an inverse correlation between late-stage diagnosis of breast cancer and survival [37, 40–47]. Because the stage at diagnosis affects outcomes and consequently the burden of disease on societies, we looked at the proportion of women diagnosed in each stage (in countries where data were available) and compared it with data from Sweden—one of the countries with the best breast cancer outcomes, where less than 10% of breast cancer patients presented with stage III or IV at diagnosis [48]. In contrast, in Latin American countries such as Peru, Colombia, and Mexico, approximately 50% of detected breast cancer cases are in advanced stages (Table 3). Chile, on the other hand, has improved breast cancer diagnosis: early breast cancer cases increased from representing 43% of all cases in 1999 to 70% of all cases in 2003 [6]. Likely, the introduction of mammography screening in the primary care program in 2001 and the setting of quality standards have been major factors in the improvement of diagnosis in Chile. Uruguay and certain wealthier regions in Brazil diagnose women earlier, albeit far below Sweden's benchmark.
Table 3.
Breast cancer stage at diagnosis in Latin American countries
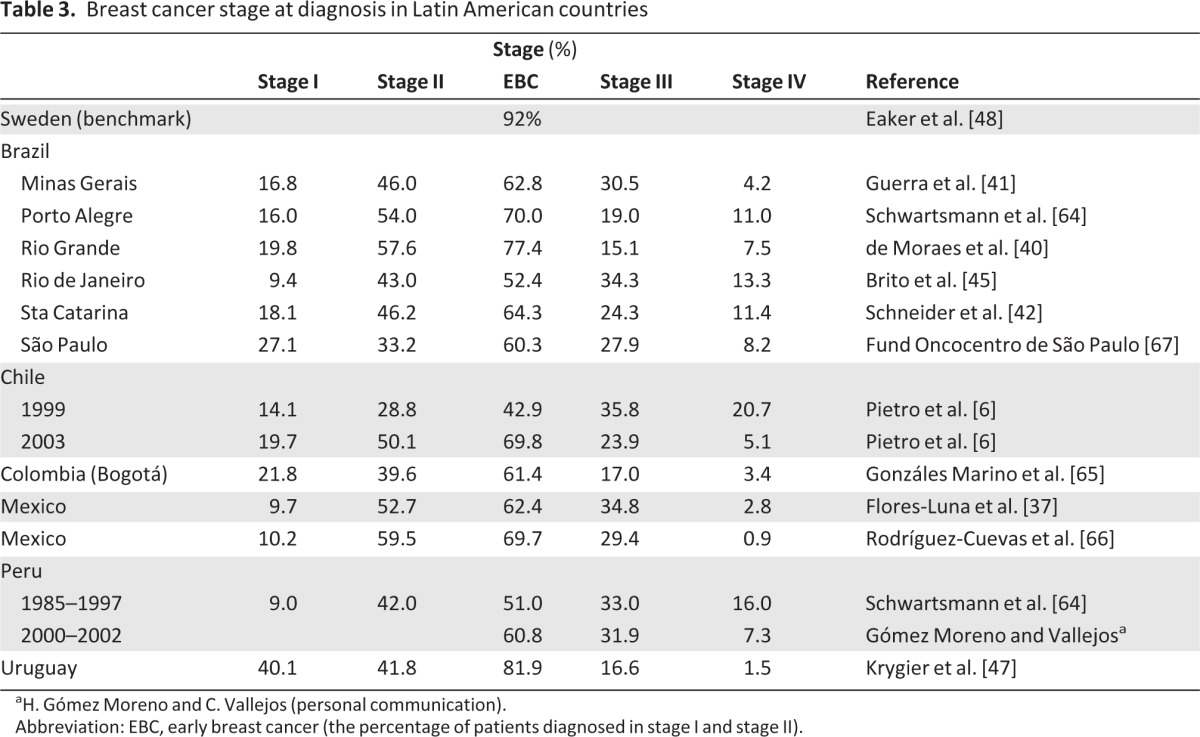
aH. Gómez Moreno and C. Vallejos (personal communication).
Abbreviation: EBC, early breast cancer (the percentage of patients diagnosed in stage I and stage II).
The mortality-to-incidence ratio (MIR) of the countries included in the study is shown in Figure 3, using data adapted from GLOBOCAN 2002 [49] and GLOBOCAN 2008 [2]. For every 100 women diagnosed with breast cancer, only 27 will die of the disease in Argentina and Uruguay, whereas 37 and 40 will die in Mexico and Panama, respectively. In general, the treatment and care for patients with breast cancer in Argentina or Uruguay saves comparatively more lives than in Mexico or Panama. As illustrated in Figure 3, when data are compared from 2002 to 2008, a positive trend is evident for the whole region. However, this proxy-survival evolved more favorably in some countries than in others. Costa Rica shows a dramatic improvement in MIR, dropping closer to the levels of Uruguay, Argentina, and Chile. Colombia, Ecuador, and Peru are also improving, but still lag behind. Brazil demonstrated the least progress.
Figure 3.
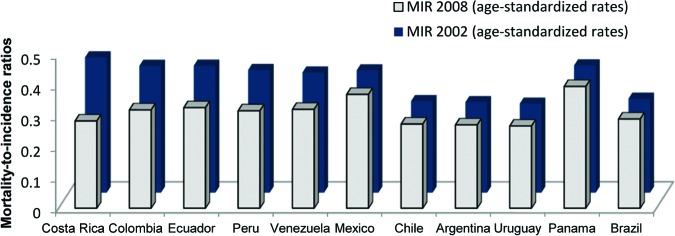
Mortality-to-incidence ratios in 2002 and 2008. Adapted from [49] and [2] with permission.
Abbreviation: MIR, mortality-to-incidence ratio.
Economic Burden
The health burden of breast cancer also has an economic impact, which has been described for several European countries [1]. Unfortunately, the economic burden of breast cancer in Latin American countries is not well documented and is difficult to estimate. The overall cost of breast cancer can be estimated by identifying and measuring all costs incurred by the health care systems, patients and their families, and those in other sectors, such as social security and pensions. Little or no data are available for most countries. Here, we report the case studies estimating the direct medical cost of breast cancer care in Brazil and Mexico.
Table 4 summarizes the results of a retrospective study of 199 women with breast cancer treated at a private practice in Rio de Janeiro, Brazil [50], and a cohort study of 1,175 women with breast cancer treated by the Mexican Social Security Institute [51]. Annual costs for treating patients with stage IV breast cancer are three to four times higher than for patients with stage I breast cancer. Estimates for Brazil are higher than those for Mexico, which can be partly explained by the different treatment configuration in the private and public settings. In the Mexican public setting, almost 50% of patients are diagnosed in metastatic stages, compared with less than 20% of patients included in the Brazilian study.
Table 4.
Costs of breast cancer treatment by stage at diagnosis in a private clinic in Brazil [50] and in the public sector in Mexico [51]
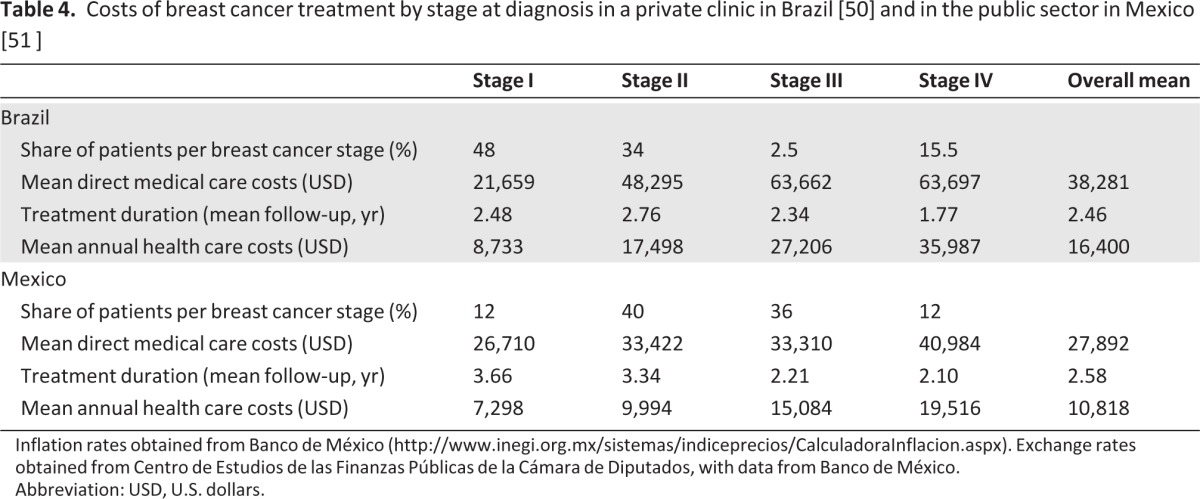
Inflation rates obtained from Banco de México (http://www.inegi.org.mx/sistemas/indiceprecios/CalculadoraInflacion.aspx). Exchange rates obtained from Centro de Estudios de las Finanzas Públicas de la Cámara de Diputados, with data from Banco de México.
Abbreviation: USD, U.S. dollars.
According to the National Agency of Supplementary Health, 75% of women diagnosed with breast cancer in Brazil have no private insurance and depend exclusively on the public system [52]. By adding the cost of discharges associated with breast cancer in 2010, we estimated that the total annual public expenditure of Brazil on breast cancer treatment was U.S. $151,861,847. Thus, the mean per-patient public expenditure was U.S. $4,757 in that year; far from the more than U.S. $40,000 spent in Europe annually per breast cancer case [1].
In Mexico in 2004, popular health insurance was introduced to cover medical care for the 50 million uninsured citizens and, by doing so, to reduce the prevalence of catastrophic health expenditures. However, according to the National Committee for Health and Social Protection of the Secretary of Health, the treatment of 11,468 breast cancer cases for a total of MEX $1.302 million had been authorized by June 30, 2010 [53]. On average, the insurance covers U.S. $8,940 per patients with breast cancer—only enough to cover 1 year of the treatment of stage I breast cancer in Mexico, according to an estimate by Knaul et al. [51] adjusted to 2010 (Table 4).
In Mexico, as in Brazil, the health care budget may not be enough to pay for the treatment of all patients with breast cancer with the same standard, and ensuring sufficient public funding for breast cancer care remains a key issue. As we can see, Latin America's tendency to diagnose patients in late stages of disease not only impacts survival rate negatively, but also increases per-case health expenditure.
The increased morbidity and mortality of patients with metastatic cancer greatly amplifies overall costs by raising expenditure throughout the health care system, including primary care facilities, and by increasing indirect costs. In Europe, indirect costs are estimated to be 110%–200% of direct costs [54–56], but no information is available for Latin America. However, indirect costs must be significant because the majority of women are diagnosed and die at a relatively young age, thus depriving society of many productive years.
Care and Access to Treatment
Health care in Latin America has been improving over the past 5 to 10 years, driven by reforms toward more universal health care access, based on primary care. Giedion and Ávila reviewed the structure of the health care systems in Latin America, highlighting the marked differences across countries in terms of their level of decentralization as well as the role of the private sector [57]. They found that access to breast cancer care depends mainly on insurance type and geographical location. Even within a particular insurance type or country, great differences in access exist depending on the wealth of the region (i.e., state) and the willingness to invest in breast cancer care. In this section, we provide a few examples.
In Argentina, the compulsory medical plan establishes that the reimbursement of drugs will reach at least 40% in acute conditions, 70% in chronic diseases, and 100% in hospital drugs, as well as special treatments such as oncology therapies. So, all Argentinian patients with breast cancer have free access to oncology treatment by law. However, a survey of 95 medical oncologists revealed that there is much heterogeneity in what medical oncologists think is the best treatment option and what they could prescribe to their patients [58].
In Brazil, inequalities exist among insurance types and regions. The reimbursement of cancer treatment governed by the High Complexity Discharge Authorization covers reimbursement for surgery and chemotherapy but does not cover biological therapy. Thus, patients often pursue lawsuits to get access to specific medications. Cruz Lopez et al. estimated that the amount spent in such lawsuits in 2007 exceeded R$500 million [59], considerably more than the R$307 million spent in the care of breast cancer patients by the public health system. Furthermore, due to the restricted federal reimbursement, some states provide additional treatments for cancer care, such as the wealthier state of São Paulo. Since 2009, the Secretary of Health of this particular state incorporated seven new oncological drugs into the treatments offered in their hospitals. However, São Paulo is an exception. The majority of the other states do not provide additional coverage to the federal package, thus resulting in strong regional differences in Brazilian breast cancer health care.
In Colombia, the public and private sectors are explicitly integrated to extend health care coverage. The government's goal is to attain a coverage rate of 94% by 2012, from 85% in 2008 [60]. Since 2004, the Colombian universal health insurance has included cancer treatment in the mandatory health plan with a subsidized scheme providing specific entitlements for the poor.
In Peru, 64% of the population depends on the public health insurance [57], which only covers breast cancer diagnosis but not treatments. Not surprisingly, health outcomes in Peru are far below average and among the lowest in the region.
Conclusions
Breast cancer is the leading cause of cancer deaths in women in Latin America. An estimated 114,900 women are diagnosed and an estimated 37,000 women die of breast cancer every year in this region. In addition, both incidence and mortality are increasing. The number of deaths from breast cancer is expected to double by 2030, to 74,000 every year [24]. Aging is the main risk factor of breast cancer. It is expected that demographic changes in the region will cause epidemiological shifts and increase breast cancer incidence.
Survival rates are more than 85% in those countries with best outcomes (international benchmark), whereas in Latin America the breast cancer survival rate hardly exceeds 70%. Reduced survival correlates with late diagnosis. Approximately 30%–40% of patients in the countries included in the study are diagnosed in metastatic phases III and IV; in Mexico, Colombia, and Peru, this rate is as high as 40%–50% of the patients. Meanwhile, in Northern Europe, late diagnosis accounts for only 10% of breast cancer cases. Breast cancer outcomes have improved during the last decade, as evidenced by comparison of the MIRs between 2002 and 2008. Costa Rica has shown the most progress, whereas Brazil, Mexico, and Panama have not seen significant improvements in MIR ratios in recent years.
The economic burden is also significant. Most countries allocate insufficient resources to tackle the disease. Women are not diagnosed early enough and do not get access to optimal therapies, resulting in high morbidity and the associated societal costs. Universal health care coverage is still lacking in many countries in the region; even in those countries where the entitlement to breast cancer health services is guaranteed by law, it is not accompanied by the necessary resources.
Survival rates are more than 85% in those countries with best outcomes (international benchmark), whereas in Latin America the breast cancer survival rate hardly exceeds 70%. Reduced survival correlates with late diagnosis. Approximately 30%–40% of patients in the countries included in the study are diagnosed in metastatic phases III and IV; in Mexico, Colombia, and Peru, this rate is as high as 40%–50% of the patients.
This review clearly demonstrates that more investments are needed in Latin American health systems for breast cancer screening, earlier diagnosis, and accessible and affordable treatment for all women.
This article is available for continuing medical education credit at CME.TheOncologist.com.
Acknowledgments
This work was funded by Hoffmann-La Roche International.
We thank the many clinical experts who provided us with their valuable input on breast cancer treatment, service configuration, and outcomes in their countries, including Dr. Maria Viniegra (Argentina), Dr. Antonio Bassani and Dr. Antonio Buzaid (Brazil), Dr. José Miguel Reyes and Dr. Roberto Torres Ulloa (Chile), Dr. Hernán Carranza (Colombia), Dr. Gonzalo Vargas and Dr. Denis Landaverde Recinos (Costa Rica), Dr. Hernán Lupera and Dr. Fernando Checa (Ecuador), Dr. Flavia Morales-Vásquez and Dr. Benito Sánchez (Mexico), Dr. Henry Gómez Moreno and Dr. Carlos Vallejos (Peru), Dr. Graciela Sabini and Dr. Gabriel Krygier (Uruguay), and Dr. Carlos Montesino Acosta and Dr. Karen Kubicek (Venezuela). We also thank the patients' organizations that assisted with this study, including Instituto Oncoguia, Asociación Mexicana de Lucha contra el Cáncer de Mama; Asociación Mexicana de Lucha contra el Cáncer, Yo Mujer, Esperantra, Fundación Nacional de Solidaridad contra el Cáncer de Mama, Fundación Anna Ross, Rehabilitación Integral en Patología Mamaria, Fundación de Lucha contra el Cáncer de Mama, and FUNDASENO.
All opinions expressed in this report, along with the conclusions and recommendations, are those of the primary authors and may not reflect the views of the clinical experts and patient organizations that were surveyed for this study.
AUTHOR CONTRIBUTIONS
Conception/Design: Nahila Justo, Nils Wilking, Bengt Jönsson
Provision of study materials or patients: Nahila Justo, Silvana Luciani, Eduardo Cazap
Collection and/or assembly of data: Nahila Justo, Silvana Luciani
Data analysis and interpretation: Nahila Justo, Nils Wilking, Bengt Jönsson, Silvana Luciani, Eduardo Cazap
Manuscript writing: Nahila Justo, Silvana Luciani
Final approval of manuscript: Nahila Justo, Nils Wilking, Bengt Jönsson, Silvana Luciani, Eduardo Cazap
Disclosures
Nahila Justo: Roche (RF); Eduardo Cazap: Bayer, Schering Pharma (C/A); Bayer, Bristol-Myers Squibb, Fresenius (H); Poniard Pharmaceuticals, Daiichi Sankyo Pharma (RF). The other authors indicated no financial relationships.
Section editors: Gabriel Hortobágyi: Antigen Express, Galena Biopharma, Novartis, Rockpointe (C/A); Novartis (RF); Taivex (O); founder and member of the board of directors for Citizen's Oncology Foundation; Kathleen Pritchard: Novartis, Roche, AstraZeneca, Pfizer, Abraxis, Boehringer-Ingelheim, GlaxoSmithKline, Sanofi, Ortho-Biotech, YM Biosciences, Amgen, Bristol-Myers Squibb, Bayer Schering Pharma (C/A, H)
Reviewer “A”: None
C/A: Consulting/advisory relationship; RF: Research funding; E: Employment; H: Honoraria received; OI: Ownership interests; IP: Intellectual property rights/inventor/patent holder; SAB: scientific advisory board
References
- 1.Wilking N, Kasteng F. A review of breast cancer care and outcomes in 18 countries in Europe, Asia and Latin America. [Accessed December 10, 2012]. Available at http://www.comparatorreports.se/A_review_of_breast_cancer_care_and_outcomes_26Oct2009.pdf.
- 2.Ferlay J, Shin H, Bray F, et al. GLOBOCAN 2008 v1.2: Cancer incidence and mortality worldwide. Lyon, France: International Agency for Research on Cancer; 2010. [Google Scholar]
- 3.Tirona MT, Sehgal R, Ballester O. Prevention of breast cancer (part I): Epidemiology, risk factors, and risk assessment tools. Cancer Invest. 2010;28:743–750. doi: 10.3109/07357907.2010.494321. [DOI] [PubMed] [Google Scholar]
- 4.Lozano-Ascencio R, Gómez-Dantés H, Lewis S, et al. Breast cancer trends in Latin America and the Caribbean. Salud Publica Mex. 2009;51(suppl 2):S147–S156. doi: 10.1590/s0036-36342009000800004. [DOI] [PubMed] [Google Scholar]
- 5.Freitas R, Jr, Freitas NM, Curado MP, et al. Incidence trend for breast cancer among young women in Goiânia, Brazil. Sao Paulo Med J. 2010;128:81–84. doi: 10.1590/S1516-31802010000200007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Prieto MTS. Situación epidemiológica del cáncer de mama en Chile 1994–2003. Rev Med Clin Condes. 2006;17:142–148. [Google Scholar]
- 7.Ortiz Barboza A, Vargas Alvarado RM, Muoz Leiva G. Unidad de Estadística del Registro Nacionalde Tumores, Dirección Vigilancia de la Salud. San José, Costa Rica: Ministerio de Salud de Costa Rica; 2005. Incidencia y Mortalidad del Cáncer en Costa Rica 1990–2003. [Google Scholar]
- 8.Vassallo JA, De Stefani E, Barrios E, et al. Atlas de incidencia de cáncer en el Uruguay, 1996–1997: Programa de Vigilancia Epidemiológica. Montevideo, Uruguay: Registro Nacional de Cáncer Uruguay; [Accessed December 2010]. Available at http://www.urucan.org.uy/uilayer/ve/inc_96_97/pve_datos_inc_96_97_m_mama.pdf. [Google Scholar]
- 9.Barrios E, Vassallo JA, Alonso R, et al. Programa de Vigilancia Epidemiológica. Montevideo, Uruguay: Registro Nacional de Cáncer Uruguay; 2010. Atlas de incidencia del cáncer en el Uruguay, 2002–2006. [Google Scholar]
- 10.Vainshtein J. Disparities in breast cancer incidence across racial/ethnic strata and socioeconomic status: A systematic review. J Natl Med Assoc. 2008;100:833–839. doi: 10.1016/s0027-9684(15)31378-x. [DOI] [PubMed] [Google Scholar]
- 11.Igene H. Global health inequalities and breast cancer: An impending public health problem for developing countries. Breast J. 2008;14:428–434. doi: 10.1111/j.1524-4741.2008.00618.x. [DOI] [PubMed] [Google Scholar]
- 12.Ravera R, Medina E, López IM. Breast cancer epidemiology. Rev Med Chil. 1991;119:1059–1065. [PubMed] [Google Scholar]
- 13.Fejerman L, Romieu I, John EM, et al. European ancestry is positively associated with breast cancer risk in Mexican women. Cancer Epidemiol Biomarkers Prev. 2010;19:1074–1082. doi: 10.1158/1055-9965.EPI-09-1193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nasir A, Shackelford RE, Anwar F, Yeatman TJ. Genetic risk of breast cancer. Minerva Endocrinol. 2009;34:295–309. [PubMed] [Google Scholar]
- 15.Petrucelli N, Daly MB, Feldman GL. Hereditary breast and ovarian cancer due to mutations in BRCA1 and BRCA2. Genet Med. 2010;12:245–259. doi: 10.1097/GIM.0b013e3181d38f2f. [DOI] [PubMed] [Google Scholar]
- 16.Baquet CR, Mishra SI, Commiskey P, et al. Breast cancer epidemiology in blacks and whites: Disparities in incidence, mortality, survival rates and histology. J Natl Med Assoc. 2008;100:480–488. doi: 10.1016/s0027-9684(15)31294-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Aaman TB, Stalsberg H, Thomas DB. Extratumoral breast tissue in breast cancer patients: A multinational study of variations with age and country of residence in low- and high-risk countries. WHO Collaborative Study of Neoplasia and Steroid Contraceptives. Int J Cancer. 1997;71:333–339. doi: 10.1002/(sici)1097-0215(19970502)71:3<333::aid-ijc4>3.0.co;2-z. [DOI] [PubMed] [Google Scholar]
- 18.Martin RM, Middleton N, Gunnell D, et al. Breast-feeding and cancer: The Boyd Orr cohort and a systematic review with meta-analysis. J Natl Cancer Inst. 2005;97:1446–1457. doi: 10.1093/jnci/dji291. [DOI] [PubMed] [Google Scholar]
- 19.Chlebowski RT, Chen Z, Anderson GL, et al. Ethnicity and breast cancer: Factors influencing differences in incidence and outcome. J Natl Cancer Inst. 2005;97:439–448. doi: 10.1093/jnci/dji064. [DOI] [PubMed] [Google Scholar]
- 20.Robles SC, Galanis E. Breast cancer in Latin America and the Caribbean. Rev Panam Salud Publica. 2002;11:178–185. doi: 10.1590/s1020-49892002000300007. [DOI] [PubMed] [Google Scholar]
- 21.Pan American Health Organization. World population prospects: The 2008 revision (CD-ROM edition) Washington, DC: Pan American Health Organization; 2009. [Google Scholar]
- 22.Torres-Sanchez L, Galvan-Portillo M, Lewis S, et al. Diet and breast cancer in Latin-America. Salud Publica Mex. 2009;51:S181–S90. doi: 10.1590/s0036-36342009000800008. [DOI] [PubMed] [Google Scholar]
- 23.Bay G, Jaspers Faijer D. Latin American and Caribbean demographic observatory: population projection. Quito, Ecuador: Latin American and Caribbean Demographic Centre; 2007. [Google Scholar]
- 24.World Health Organization. Geneva, Switzerland: World Health Organization; 2008. The global burden of disease: 2004 summary tables. October 2008 update. [Google Scholar]
- 25.Ferlay J, Shin HR, Bray F, et al. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127:2893–2917. doi: 10.1002/ijc.25516. [DOI] [PubMed] [Google Scholar]
- 26.Chatenoud L, Bertuccio P, Bosetti C, et al. Trends in cancer mortality in Brazil, 1980–2004. Eur J Cancer Prev. 2010;19:79–86. doi: 10.1097/CEJ.0b013e32833233be. [DOI] [PubMed] [Google Scholar]
- 27.Bosetti C, Malvezzi M, Chatenoud L, et al. Trends in cancer mortality in the Americas, 1970–2000. Ann Oncol. 2005;16:489–511. doi: 10.1093/humrep/mdi086. [DOI] [PubMed] [Google Scholar]
- 28.Malvezzi M, Bosetti C, Chatenoud L, et al. Trends in cancer mortality in Mexico, 1970–1999. Ann Oncol. 2004;15:1712–1718. doi: 10.1093/annonc/mdh424. [DOI] [PubMed] [Google Scholar]
- 29.Barrios E, Ronco A, Fierro L, et al. Tendencias de la mortalidad por cáncer en Uruguay, 1953–1997. Rev Med Uruguay. 2002;18:167–174. [Google Scholar]
- 30.Niclis C, Del Pilar DM, La VC. Breast cancer mortality trends and patterns in Cordoba, Argentina in the period 1986–2006. Eur J Cancer Prev. 2010;19:94–99. doi: 10.1097/CEJ.0b013e328333fb52. [DOI] [PubMed] [Google Scholar]
- 31.Ortega Jacome GP, Koifman RJ, Rego Monteiro GT, et al. Environmental exposure and breast cancer among young women in Rio de Janeiro, Brazil. J Toxicol Environ Health A. 2010;73:858–865. doi: 10.1080/15287391003744773. [DOI] [PubMed] [Google Scholar]
- 32.Allemani C, Sant M, Weir HK, et al. Breast cancer survival in the US and Europe: A CONCORD high-resolution study. Int J Cancer. 2013;132:1170–1181. doi: 10.1002/ijc.27725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Peto R. The worldwide overview: New results for systemic adjuvant therapies. Paper presented at: San Antonio Breast Cancer Symposium; December 13–16, 2007; San Antonio, Texas. [Google Scholar]
- 34.Sankaranarayanan R, Swaminathan R, Brenner H, et al. Cancer survival in Africa, Asia, and Central America: A population-based study. Lancet Oncol. 2010;11:165–173. doi: 10.1016/S1470-2045(09)70335-3. [DOI] [PubMed] [Google Scholar]
- 35.Coleman MP, Quaresma M, Berrino F, et al. Cancer survival in five continents: A worldwide population-based study (CONCORD) Lancet Oncol. 2008;9:730–756. doi: 10.1016/S1470-2045(08)70179-7. [DOI] [PubMed] [Google Scholar]
- 36.Serra I, Martinez R, Mimica X, et al. Cáncer de mama en Chile. Un aporte clínico y epidemiológico según un registro poblacional metropolitano: 1.485 pacientes. Rev Chilena de Cirugía. 2009;61:507–514. [Google Scholar]
- 37.Flores-Luna L, Salazar-Martinez E, Duarte-Torres RM, et al. Prognostic factors related to breast cancer survival. Salud Publica Mex. 2008;50:119–125. doi: 10.1590/s0036-36342008000200005. [DOI] [PubMed] [Google Scholar]
- 38.Vallejos C, Gomez H, Abugattas J, et al. Clinicopathologic, molecular subtype, and survival prognostic features in premenopausal breast cancer patients by age at diagnosis. J Clin Oncol. 2010;28(suppl 15):653. [Google Scholar]
- 39.Cintra JR, Guerra MR, Bustamante-Teixeira MT, et al. Breast cancer survival in developing countries: The reminder disparities in health service access. J Clin Oncol. 2010;28(suppl 15):12015. [Google Scholar]
- 40.de Moraes AB, Zanini RR, Turchiello MS, et al. Survival study of breast cancer patients treated at the hospital of the Federal University in Santa Maria, Rio Grande do Sul, Brazil. Cad Saude Publica. 2006;22:2219–2228. doi: 10.1590/s0102-311x2006001000028. [DOI] [PubMed] [Google Scholar]
- 41.Guerra MR, Mendonca GA, Bustamante-Teixeira MT, et al. Five-year survival and prognostic factors in a cohort of breast cancer patients treated in Juiz de Fora, Minas Gerais State, Brazil. Cad Saude Publica. 2009;25:2455–2466. doi: 10.1590/s0102-311x2009001100015. [DOI] [PubMed] [Google Scholar]
- 42.Schneider IJ, d'Orsi E. Five-year survival and prognostic factors in women with breast cancer in Santa Catarina State, Brazil. Cad Saude Publica. 2009;25:1285–1296. doi: 10.1590/s0102-311x2009000600011. [DOI] [PubMed] [Google Scholar]
- 43.Iturbe J, Leone JP, Zwenger AO, et al. Treatment of stage I breast cancer (T1N0M0): A long-term follow-up. J Clin Oncol. 2008;26(suppl 15):11509. [Google Scholar]
- 44.Iturbe J, Zwenger AO, Lacava JA, et al. Treatment of early breast cancer: A long-term follow-up study—GOCS experience. J Clin Oncol. 2009;27(suppl 15):11610. [Google Scholar]
- 45.Brito C, Portela MC, Vasconcellos MT. Survival of breast cancer women in the state of Rio de Janeiro, Southeastern Brazil. Rev Saude Publica. 2009;43:481–489. doi: 10.1590/s0034-89102009000300012. [DOI] [PubMed] [Google Scholar]
- 46.Cardona Arcila JP, Chacon Cardona JA, Sanchez Villegas T, et al. Breast cancer stage IV from a specific city in a developing country like Colombia. J Clin Oncol. 2008;26(suppl 15):12017. [Google Scholar]
- 47.Krygier G, Barrios E, Cataldi S, et al. Breast cancer experience in Uruguay: A 21-year follow up of 1,906 patients in the same institution. J Clin Oncol. 2007;25(suppl 18):21163. [Google Scholar]
- 48.Eaker S, Halmin M, Bellocco R, et al. Social differences in breast cancer survival in relation to patient management within a National Health Care System (Sweden) Int J Cancer. 2009;124:180–187. doi: 10.1002/ijc.23875. [DOI] [PubMed] [Google Scholar]
- 49.Parkin DM, Bray F, Ferlay J, et al. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. doi: 10.3322/canjclin.55.2.74. [DOI] [PubMed] [Google Scholar]
- 50.Teich N, Pepe C, Vieira FM, et al. Retrospective cost analysis of breast cancer patients treated in a Brazilian outpatient cancer center. J Clin Oncol. 2010;28(suppl 15):11026. [Google Scholar]
- 51.Knaul FM, Arreola-Ornelas H, Velazquez E, et al. The health care costs of breast cancer: The case of the Mexican Social Security Institute. Salud Publica Mex. 2009;51:S286–S295. doi: 10.1590/s0036-36342009000800019. [DOI] [PubMed] [Google Scholar]
- 52.Agência Nacional de Saúde Suplementar. Caderno de Informação da Saúde Suplementar: Março 2012. 2011. [Accessed March 1, 2011]. Available at http://www.ans.gov.br/images/stories/Materiais_para_pesquisa/Perfil_setor/Dados_e_indicadores_do_setor/20120517_perfil_do_setor_caderno_de_informacoes.xls.
- 53.Cortés Gallo G. International Conference on Localizing MDGs Local Agendas for Human Development: United Nations Development Programme: Mexico, 2010. [Accessed March 1, 2011]. Available at http://www.mdgconference.chiapas.mx/media/papers/4.2_Gabriel_Cortes.pdf.
- 54.Lidgren M, Wilking N, Jonsson B. Cost of breast cancer in Sweden in 2002. Eur J Health Econ. 2007;8:5–15. doi: 10.1007/s10198-006-0003-8. [DOI] [PubMed] [Google Scholar]
- 55.Cost of Illness. Federal Health Monitoring Germany. [Accessed August 1, 2009]. Available at http://www.gbe-bund.de/oowa921-install/servlet/oowa/aw92/dboowasys921.xwdevkit/xwd_init?gbe.isgbetol/xs_start_neu/&p_aid=i&p_aid=41836111&nummer=556&p_sprache=E&p_indsp=-&p_aid=9843158.
- 56.Amaltic F. Analyse Économique des Coûts du Cancer en France. Institute Nacional du Cancer. 2007. [Accessed December 2010]. Available at http://www.e-cancer.fr/component/docman/doc_download/1185-etudeeconomieducancer.pdf.
- 57.Giedion Ú, Villar M, Ávila A, Seguro FM-IdCd Los sistemas de Salud en Latinoamérica y el papel del Seguro Privado FUNDACIÓN MAPFRE-Instituto de Ciencias del Seguro; 2010. [Accessed December 2010]. Available at: http://www.mapfre.com/ccm/content/documentos/fundacion/cs-seguro/libros/los-sistemas-de-salud-en-latinoamerica-y-el-papel-del-seguro-privado.pdf.
- 58.Costanzo MV, Nervo A, Lopez C, Chacon R. Adjuvant breast cancer in Argentina: Disparities between prescriptions and funding requirements—A survey. J Clin Oncol. 2008;26(15):17571. [Google Scholar]
- 59.Lopes LC, Barberato-Filho S, Costa AC, et al. Rational use of anticancer drugs and patient lawsuits in the state of Sao Paulo, Southeastern Brazil. Rev Saude Publica. 2010;44:620–628. doi: 10.1590/s0034-89102010000400005. [DOI] [PubMed] [Google Scholar]
- 60.Clavijo S, Torrente C Centro de Estudios Económicos-Asociación Nacional de Instituciones. The Health Care System and its Fiscal Impact in Colombia 2008. [Accessed December 2010]. Available at: http://ssrn.com/abstract=1997229.
- 61.United Nations Statistics. Per capita GDP at current prices - US dollars. [Accessed August 1, 2009]. Available at http://data.un.org.
- 62.United Nations Statistics. Human development indices: A statistical update 2009. [Accessed August 1, 2009]. Available at http://data.un.org/DocumentData.aspx?id=185#15.
- 63.Ono T. WHO global comparable estimates: Risk factors. [Accessed October 5, 2005]. Available at https://apps.who.int/infobase/Comparisons.aspx.
- 64.Schwartsmann G. Breast cancer in South America: Challenges to improve early detection and medical management of a public health problem. J Clin Oncol. 2001;19(suppl 18):118S–124S. [PubMed] [Google Scholar]
- 65.Gonzalez-Marino MA. Breast cancer in the Pedro Claver hospital in Bogota, 2004. Rev Salud Publica (Bogota) 2006;8:163–169. doi: 10.1590/s0124-00642006000200004. [DOI] [PubMed] [Google Scholar]
- 66.Rodríguez-Cuevas S, Macías C, Franceschi D, et al. Breast carcinoma presents a decade earlier in Mexican women than in women in the United States or European countries. Cancer. 2001;91:863–868. [PubMed] [Google Scholar]
- 67.Fundação Oncocentro de São Paulo, Registro de Câncer de São Paulo - Departamento de Epidemiologia da Faculdade de Saùde Pública da USP. [Accessed December 2010]. Available at: http://ww2.prefeitura.sp.gov.br/cgi/deftohtm.exe?secretarias/saude/TABNET/CA/cancer.def.