

Abstract
Objectives
The aim of this study was to evaluate the radiological and clinical features of adenomatoid odontogenic tumours (AOTs).
Methods
A total of 272 cases (267 from the English-language literature and 5 new cases) were analysed with special emphasis on their radiological features.
Results
The patients' ages at time of diagnosis ranged from 3 years to 82 years (mean 18.4 years). The maxilla-to-mandible ratio was 1.7:1. Mandibular lesions were significantly more frequent among patients older than 16 years (p = 0.032). Expansion of the cortex was significantly more prominent among patients older than 16 years (p = 0.045). There was a positive correlation between the size of the lesion and the age of the patient at the time of diagnosis (p = 0.016). The size was also associated with increased root resorption (p < 0.001), ill-defined borders (p < 0.001), expansion (p < 0.001) and perforation of the cortex (p < 0.001). Small opacities were present in 77% of lesions and were associated with expansion of the cortex (p = 0.043). The significant radiological features in patients aged 30 years and above were root resorption (p = 0.013) and lesions crossing the midline (p = 0.019).
Conclusions
The size of an AOT is influenced by the patient's age. It is also associated with root resorption, ill-defined borders, expansion and perforation of the cortex, but it cannot be ruled out that those changes reflect a longer duration of the lesion.
Keywords: adenomatoid odontogenic tumour, odontogenic tumours, radiology, jaws
Introduction
Adenomatoid odontogenic tumours (AOTs) are unique odontogenic lesions located either centrally within the jaws or peripherally in the soft tissue overlying the tooth-bearing area. Some authors consider AOTs to be true benign, non-aggressive non-invasive neoplasms, whereas others view them as developmental hamartomatous odontogenic growths.1 AOTs have three clinicopathologic variants: intraosseous follicular (pericoronal), intraosseous extrafollicular (extracoronal) and peripheral (extraosseous). The follicular type is associated with the crown and also often with part of the root of an unerupted tooth, whereas the extrafollicular type is not associated with unerupted teeth. The peripheral variant is associated with gingival structures.2
In 1971, the World Health Organization adopted the term “adenomatoid odontogenic tumour” to describe this entity, as had been proposed by Philipsen and Birn.3 It is estimated that AOTs constitute about 2.2–7.1% of all odontogenic tumours, and the increasing number of reports in the literature on AOT indicates that the tumour develops more frequently than was formerly expected.3,4 Based on radiographic findings, differentiating AOTs from dentigerous cysts, keratocystic odontogenic tumours, unicystic ameloblastomas, calcifying cystic odontogenic tumours and calcifying epithelial odontogenic tumours may pose diagnostic dilemmas.1
Most published papers on AOT have concentrated upon the epidemiological and clinical characteristics of the lesion. The purpose of this study is to analyse in detail the radiological features of AOTs described in the literature, and to add five new cases from our files. We present radiological diagnostic characterizations of this lesion that have not been reported before.
Materials and methods
The English-language literature was reviewed for adequately documented cases of AOT published between 1950 and 2010. Medline's PubMed interface and the Google Scholar search engine were searched using the keywords “adenomatoid odontogenic tumour” and “adenoameloblastoma”. Criteria for inclusion were clinical and histopathological diagnoses of AOT, and acceptable radiographic images or detailed radiological descriptions for each case. Not all data were available for all cases.
A total of 272 cases (267 from publications and 5 new cases) were analysed.5-133 The clinical and radiological data of the five new cases are described in Table 1 and Figures 1 and 2. Clinical data of age at time of diagnosis, gender, location, symptoms and radiological data of density, expansion, borders, locularity, size and impact on adjacent teeth134 were used to evaluate these cases. In the present study, incisors and canines were regarded as making up the anterior region, while the posterior region comprised premolars and molars. Lesions were considered unilocular when a single discrete radiolucent cavity was present and multilocular when septa divided the lesion into compartments. Lesions were considered as radiolucent when their content was dominantly radiolucent, including cases that contained small radio-opacities inside the radiolucent lesion. Lesions were considered as radio-opaque when their content was dominantly radio-opaque. The borders of the lesions were considered well defined when they were clearly defined or as being ill defined when the margin was not clearly delineated.135 The size of a lesion was determined by its greatest diameter. Lesions were considered small when the diameter was under 2 cm, medium-sized when it was between 2 cm and 3 cm, and large when it was above 3 cm. Teeth were considered as being involved in the lesion when they were impacted, displaced or resorbed by it. The lesion was referred to as follicular (pericoronal) when the tumour was associated with unerupted teeth, extrafollicular (extracoronal) when it had no association with unerupted teeth and peripheral (extraosseous) when it was attached to gingival structures.2
Table 1. Clinical and radiological data of five new cases of adenomatoid odontogenic tumoura.
| Case | Age (years) | Gender | Jaw | Variant (teeth involved) | Opacities | Size (cm) | Displacement | Resorption | Expansion | Perforation | Borders | Midline |
| 1 | 17 | Male | Mandible | EF (31–44) | + | 3.5 | + | – | + | - | WD | C |
| 2 | 24 | Female | Mandible | Fol (43) | – | 3.5 | – | – | – | - | WD | C |
| 3 | 22 | Male | Mandible | EF (36–43) | – | 5.5 | – | + | + | + | ID | C |
| 4 | 17 | Male | Maxilla | Fol (13) | – | 2 | + | – | – | - | WD | NC |
| 5 | 15 | Male | Maxilla | Fol (13) | – | 2 | + | – | – | - | WD | NC |
C, crossed; EF, extrafollicular; Fol, follicular; ID, ill-defined; NC, not crossed; WD, well-defined.
aAll five tumours were unilocular and radiolucent.
Figure 1.
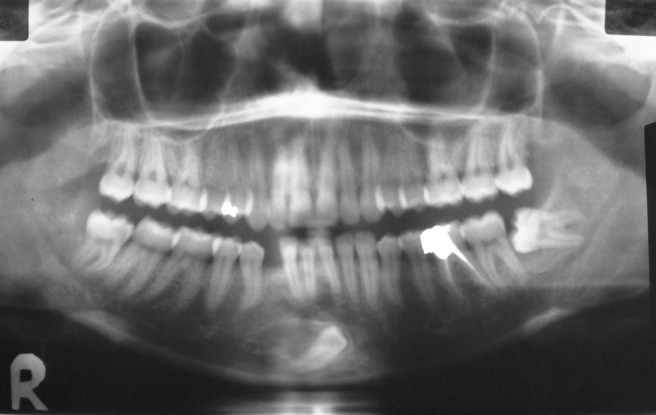
Mandibular adenomatoid odontogenic tumour. The lesion crosses the midline (extending from the right lower first premolar to the left lower lateral teeth). The right mandibular canine is unerupted. The borders are well-defined and sclerotic
Figure 2.
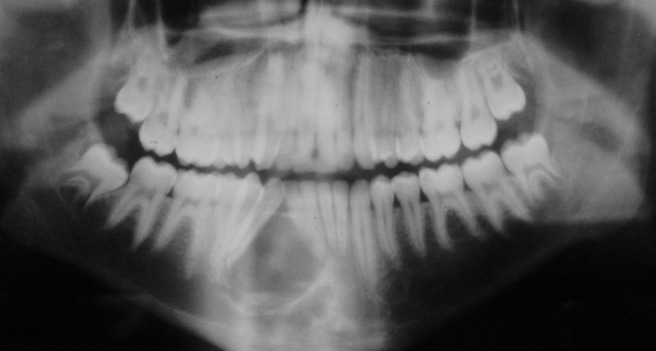
Mandibular adenomatoid odontogenic tumour. The lesion is extending from the right lower first premolar to the left lower central teeth, displacing four teeth. The borders are well-defined and sclerotic
The various parameters of AOTs were analysed for the entire cohort and for specific groups of patients up to 16 years of age (which we found to be the median age of the patients at the time of diagnosis) and those older than 16 years. A separate analysis was performed on a group of patients aged 30 years and above at the time of diagnosis, because an earlier study had shown that it was related to changes in jaw predilection.136
Statistical analysis
A descriptive analysis was used to evaluate the frequency of nominal variables. The χ2 and Fisher's exact tests were used to calculate possible associations between age, gender, presenting symptoms and the various radiographic characterizations. Pearson correlations were used to evaluate the correlation between the age of the patient and the diameter of the lesion. A t-test was used to evaluate the association between the diameter of the lesion and various radiographic characterizations (SPSS® v. 10.0; SPSS, Chicago, IL). The level of significance was set at p < 0.05.
The study was approved by the ethical committee of Tel Aviv University.
Results
A total of 272 cases of AOTs were reviewed, of which 5 were new and had not been reported until now. The age of the patients was known for 267 cases: it ranged from 3 years to 82 years, with a mean of 18.4 years and a median of 16 years (Table 2). The highest incidence of AOTs (67%) was in patients aged 10–20 years (Table 3), and most of those cases involved patients in the age range 12–16 years. The gender was known for 239 cases: 141 (59%) were females and 98 (41%) were males, with a female-to-male ratio of 1.4:1. Distribution of the lesions in the maxilla and mandible was known for 241 cases: 152 (63%) were in the maxilla and 89 (37%) were in the mandible, with a maxilla-to-mandible ratio of 1.7:1. Mandibular lesions constituted 45% of all lesions among patients older than 16 years of age, compared with 31% among patients younger than 16 years of age (p = 0.032). Specific locations within the jaws that enabled applying the criteria of “anterior” and “posterior” were known for 211 cases (Table 4): the lesions were located anteriorly in 58% of the cases. Symptomatology was known for 157 cases: 136 (87%) patients were asymptomatic and 21 (13%) complained of pain.
Table 2. Age and gender distribution of the patients with adenomatoid odontogenic tumours.
| Results | Males | Females | Total |
| Total | 98 (41) | 141 (59) | 239 |
| Mean (years) | 20 | 17.6 | 18.4 |
| Median (years) | 16 | 16 | 16 |
| Age range (years) | 8–75 | 3–82 | 3–82 |
Data are number (percentage) unless otherwise indicated.
Table 3. Distribution of adenomatoid odontogenic tumours by decade of life.
| Decade (range, years) | Reported cases (n) | % |
| First (0–9) | 15 | 5.6 |
| Second (10–19) | 180 | 67.4 |
| Third (20–29) | 52 | 19.5 |
| Fourth (30–39) | 10 | 3.7 |
| Fifth (40–49) | 3 | 1.1 |
| Sixth (50–59) | 2 | 0.7 |
| Seventh (60–69) | 3 | 1.1 |
| Eighth (70–79) | 1 | 0.37 |
| Ninth (80–89) | 1 | 0.37 |
| Total (%) | 267 | 100 |
Table 4. Location and radiological features of adenomatoid odontogenic tumoursa.
| Feature | Maxilla, n (%) | Mandible, n (%) | Total (%) |
| Location | |||
| Anterior | 77 (58) | 46 (58) | 123 (58) |
| Posterior | 55 (42) | 33 (42) | 88 (42) |
| Variant | |||
| Pericoronal | 89 (74) | 48 (60) | 137 (68.5) |
| Extracoronal | 24 (20) | 30 (37.5) | 54 (27) |
| Extraosseous | 7 (6) | 2 (2.5) | 9 (4.5) |
| Locularity | |||
| Unilocular | 59 (92) | 53 (89) | 112 (91) |
| Multilocular | 5 (8) | 6 (11) | 11 (9) |
| Displacement | |||
| Present | 48 (86) | 35 (73) | 83 (80) |
| Absent | 8 (14) | 13 (27) | 21 (20) |
| Resorption | |||
| Present | 12 (25.5) | 6 (13) | 18 (19) |
| Absent | 35 (74.5) | 40 (87) | 75 (81) |
| Expansion | |||
| Present | 43 (69) | 37 (66) | 80 (68) |
| Absent | 19 (31) | 19 (34) | 38 (32) |
| Radiolucent | 97 (99) | 66 (97) | 163 (98) |
| Radio-opaque | 1 (1) | 2 (3) | 3 (2) |
| Opacitiesb | |||
| Present | 33 (73) | 38 (81) | 71 (77) |
| Absent | 12 (27) | 9 (19) | 21 (23) |
| Perforation | |||
| Present | 7 (8) | 6 (9) | 13 (9) |
| Absent | 77 (92) | 58 (91) | 135 (91) |
| Midline | |||
| Not crossed | 87 (96) | 52 (78) | 139 (88) |
| Crossed | 4 (4) | 15 (22) | 19 (12) |
| Borders | |||
| Well defined | 58 (87) | 48 (84) | 105 (85) |
| Ill defined | 9 (13) | 9 (16) | 18 (15) |
aThe percentage given represents the proportion of cases in which accurate interpretation could be made.
bReferring to predominantly radiolucent lesions.
The radiological features of AOTs are summarized in Table 4. The most common variant was the follicular (pericoronal). Follicular lesions accounted for 137 (69%) of the cases, and 85 of them (76%) were in the group of patients younger than 16 years of age. The extrafollicular (extracoronal) variant was reported in 54 (27%) of all cases, with 35 (42%) of them in the group of patients older than 16 years of age. The peripheral (extraosseous) variant was present in 9 (5%) of the cases, of which 8 were in the group of patients younger than 16 years of age. The follicular variant was significantly more prominent in the maxilla, whereas the extrafollicular variant was significantly more prominent in the mandible (p = 0.018).
Canines were the most common unerupted teeth associated with AOTs (74% of all unerupted teeth), and maxillary canines were the most common among them. Lesions were unilocular in 112 (91%) cases and multilocular in 11 (9%). They were classified as predominantly radiolucent in 163 (98%) of the cases, and radio-opaque in only 3 (2%). In 92 predominantly radiolucent lesions, a definite determination could be made as to the presence or absence of calcifications in the lesion; opacities (dominant and non-dominant) were present in 71 (77%) of those lesions. The opacities were described as flecks or snowflakes, patchy areas of calcification, spicules of calcification, scattered radio-opacities, irregular radio-opacities, amorphous radio-opacities, fine radio-opacities and faint radio-opacities. The size of the lesions ranged from 0.4 cm to 12 cm, with a mean of 2.9 cm. 28% of the lesions were considered small (under 2 cm), 32% were medium-sized (2–3 cm) and 40% were large lesions (above 3 cm).
Expansion of the cortex was present in 80 (68%) cases and it was significantly more prominent among patients who were older than 16 years of age (p = 0.045). Borders were well defined in 105 (85%) cases and ill defined in 19 (15%). Tooth displacement was noted in 83 (80%) cases, and root resorption was described in 18 (19%). There was perforation of the cortex in 13 (9%) cases. The lesion crossed the midline in 19 (12%) cases and involved the mandible in 15 (79%) of them (p < 0.001).
Small opacities were significantly associated with expansion of the cortex (p = 0.043). There was no significant association between lesion size and opacities, but there was a significant correlation between lesion size and the age of the patient at the time of diagnosis (p = 0.016). Lesion size was also associated with increased root resorption (p < 0.001), ill-defined borders (p < 0.001), expansion (p < 0.001), perforation of the cortex (p < 0.001) and whether or not the lesion crossed the midline (p < 0.001).
There were particularly interesting findings in patients aged 30 years and above at the time of diagnosis. These patients have shown significant predilection towards lesions in the mandible (p = 0.011, vs the entire cohort), root resorption (p = 0.013) and crossing the midline (p = 0.019).
Discussion
It had been generally accepted that the relative frequency of AOT corresponds to 2.2–7.1% of all odontogenic tumours. However, a comprehensive worldwide literature survey by Philipsen et al1 disclosed a much wider range, i.e. from 0.6% to 38.5 %. The histological findings of AOTs are remarkably similar in the literature. An AOT has been described as a tumour of odontogenic epithelium with duct-like structures and with varying degrees of inductive changes in the connective tissue. The tumour may be solid or partly cystic and may contain globular masses of calcified material.2
Some clinical findings of the present study are in general agreement with other studies published in the English-language literature. We and others have found that an AOT is usually a symptom-free lesion33,136,137 and that patients with follicular AOTs are significantly younger than those with the extrafollicular variant. This is probably due to the fact that follicular AOT is associated with the lack of tooth eruption, which leads the patient to seek dental consultation and results in early diagnosis.137,138
The mean age of the patients at the time of diagnosis was 18.4 years in the current study. Although there is a general agreement regarding the peak incidence of the tumour in the second decade of life,136-142 the mean age varied between 16 years33 and 21 years143 in the different reviews.
In the current study, the predilection for females was shown as a female-to-male ratio of 1.4:1. This finding was in agreement with the findings among African138 and non-Asian populations.137 However, the female-to-male ratio among Asian populations was reported as high as 2.3:1, and up to 3:1 among Japanese populations.137
The predilection for the maxilla and anterior region of the jaws was shown in the current study with a maxilla-to-mandible ratio of 1.7:1. Other studies reported maxilla-to-mandible ratios of 1.4:1,140 1.8:1,33,138 1.9:1137 and 2:1.136
The present study is, to our best knowledge, the first one to demonstrate the continuing influence of age on the radiological characterizations of AOTs through the analysis of multiple radiological features below and above the ages of 16 years as well as above the age of 30 years. The size of the lesion is correlated with increasing age and is significantly associated with features such as increased root resorption, ill-defined borders, expansion, perforation of the cortex and lesions crossing the midline. These changes may reflect a longer duration of the lesion due to a late diagnosis.
Our results showed that patients older than 16 years of age are more likely to present with a lesion in the mandible, the extrafollicular variant and expansion of the cortex. Patients older than 30 years are more likely to present with a lesion that displays root resorption and lesions crossing the midline.
An AOT requires a radiological differential diagnosis from a variety of odontogenic lesions. Differentiating it from a dentigerous cyst is difficult when the AOT is completely radiolucent and has a follicular relationship with an unerupted tooth.144 The follicular type of AOT, however, sometimes extends apically along the root beyond the cementoenamel junction, while dentigerous cysts are attached to the tooth at the cervical region: this feature can help to distinguish between the two types of lesions. In addition, an AOT often contains fine radio-opacities, which may also be helpful. In this regard, it is of interest to note that panoramic radiography is often unable to demonstrate radio-opacities when the calcification is minimal, whereupon intraoral radiographs may be essential for correct radiographic interpretation of an AOT in the presence of minimal quantities of calcified deposits.139 A keratocystic odontogenic tumour (KCOT) and a unicystic ameloblastoma (UA) can also mimic a follicular AOT when they are in a pericoronal location. Both of those lesions are diagnosed in the second and third decades of life (similar to an AOT), but they are more common in the posterior area of the mandible,144 as opposed to an AOT, which is more common in the anterior region of the jaws. Another lesion that needs to be distinguished from a follicular AOT is a calcifying cystic odontogenic tumour (CCOT). This lesion is similar to an AOT because it is also found in the anterior region of the jaws; it may also be associated with an unerupted tooth, may also contain radio-opacities, and is also diagnosed in the second decade of life. Because of so many close similarities, it is often impossible to differentiate between CCOTs and AOTs.145
The extrafollicular variant of AOT also needs to be differentially diagnosed from several odontogenic and non-odontogenic lesions. Among the radiolucent odontogenic lesions it has to be differentiated not only from KCOTs and UAs that are not associated with unerupted teeth but also from lateral periodontal cysts (LPCs). An LPC is located between the roots of erupted teeth in the anterior region of the mandible, but is diagnosed in patients older than those with AOTs.146 When the extrafollicular variant of an AOT contains foci of radio-opacities, it resembles not only a CCOT that is not associated with unerupted teeth but also ameloblastic fibro-odontomas (AFOs) and calcifying epithelial odontogenic tumours (CEOTs). However, these last two lesions are located mainly in the posterior area of the mandible, and, while AFO is diagnosed mainly in young children (mean age of 10 years), CEOT is diagnosed in patients older than those with AOTs.146
In conclusion, a unilocular radiolucency with opacities and tooth displacement in the anterior region of the jaws are the radiological features most characteristic of the majority of AOTs. The present analysis reveals that other features of the lesion are more variable and that they are influenced mainly by the age of the patient and by the size of the lesion. Patients older than 16 years of age are more likely to present with a lesion in the mandible, a lesion of the extrafollicular variant and expansion of the cortex. Patients older than 30 years of age are more likely to present with a lesion that displays root resorption and one that crosses the midline. These findings could be explained by the correlation between the age of the patient at the time of diagnosis and the size of the lesion. It cannot, however, be ruled out that these changes reflect a longer duration of the lesion.
Acknowledgments
The authors thank Esther Eshkol for editorial assistance.
Footnotes
The study was supported by the Ed and Herb Stein chair of Oral Pathology, Tel Aviv University, Israel.
References
- 1.Philipsen HP, Reichart PA, Siar CH, Ng KH, Lau SH, Zhang X, et al. An updated clinical and epidemiological profile of the adenomatoid odontogenic tumour: a collaborative retrospective study. J Oral Pathol Med 2007;36:383–393 [DOI] [PubMed] [Google Scholar]
- 2.Yilmaz N, Acikgoz A, Celebi N, Zengin AZ, Gunhan O. Extrafollicular adenomatoid odontogenic tumor of the mandible: report of a case. Eur J Dent 2009;3:71–74 [PMC free article] [PubMed] [Google Scholar]
- 3.Philipsen HP, Birn H. The adenomatoid odontogenic tumour. Ameloblastic adenomatoid tumour or adeno-ameloblastoma. Acta Pathol Microbiol Scand 1969;75:375–398 [PubMed] [Google Scholar]
- 4.Reichart PA, Philipsen HP. Odontogenic tumors and allied lesions. London, UK; Quintessence Publ; 2004 [Google Scholar]
- 5.Friedrich RE, Scheuer HA, Zustin J. Adenomatoid odontogenic tumor (AOT) of maxillary sinus: case report with respect to immunohistochemical findings. In Vivo 2009;23:111–116 [PubMed] [Google Scholar]
- 6.Sandhu SV, Narang RS, Jawanda M, Rai S. Adenomatoid odontogenic tumor associated with dentigerous cyst of the maxillary antrum: a rare entity. J Oral Maxillofac Pathol 2010;14:24–28 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Friedrich RE, Zustin J, Scheuer HA. Adenomatoid odontogenic tumour of the mandible. Anticancer Res 2010;30:1787–1792 [PubMed] [Google Scholar]
- 8.Ide F. Inter-radicular adenomatoid odontogenic tumor of the anterior mandible. J Oral Maxillofac Surg 2010;68:490–491 [DOI] [PubMed] [Google Scholar]
- 9.Martínez A, Mosqueda-Taylor A, Marchesani FJ, Brethauer U, Spencer ML. Adenomatoid odontogenic tumor concomitant with cystic complex odontoma: case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:e25–29 [DOI] [PubMed] [Google Scholar]
- 10.Carlos-Bregni R, Vargas PA, Santos Silva AR, Chaves-Netto HD, de Moraes M, Lopes MA. Adenomatoid odontogenic hamartoma: concerns about correct nomenclature and 2 additional case reports. J Oral Maxillofac Surg 2009;67:1779–1780 [DOI] [PubMed] [Google Scholar]
- 11.Ali YH, Hussain AE. Adenomatoid odontogenic tumour of the middle turbinate: case report and literature review. J Otolaryngol Head Neck Surg 2009;38:E9–13 [PubMed] [Google Scholar]
- 12.Garg D, Palaskar S, Shetty VP, Bhushan A. Adenomatoid odontogenic tumor—hamartoma or true neoplasm: a case report. J Oral Sci 2009;51:155–159 [DOI] [PubMed] [Google Scholar]
- 13.Yilmaz N, Acikgoz A, Celebi N, Zengin AZ, Gunhan O. Extrafollicular adenomatoid odontogenic tumor of the mandible: report of a case. Eur J Dent 2009;3:71–74 [PMC free article] [PubMed] [Google Scholar]
- 14.Ide F, Mishima K, Saito I, Kusama K. Diagnostically challenging epithelial odontogenic tumors: a selective review of 7 jawbone lesions. Head Neck Pathol 2009;3:18–26 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.McGuff HS, Alderson GL, Jones AC, Edgin WA. Oral and maxillofacial pathology case of the month. Adenomatoid odontogenic tumor. Tex Dent J 2008;125:1192–1195 [PubMed] [Google Scholar]
- 16.Bartake AR, Punnya VA, Sudeendra P, Rekha K. Two adenomatoid odontogenic tumours of the maxilla: a case report. Br J Oral Maxillofac Surg 2009;47:638–640 [DOI] [PubMed] [Google Scholar]
- 17.Durrani F, Singh R. Intraosseous follicular adenomatoid odontogenic tumour-a case report. Int J Dent 2009;2009:597483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Cudney N, Persico J, Cordell KG, D'Silva NJ. Adenomatoid odontogenic tumor developing in association with an odontoma: report of a case. Quintessence Int 2008;39:693–697 [PubMed] [Google Scholar]
- 19.Santos JN, Lima FO, Romério P, Souza VF. Adenomatoid odontogenic tumor: an unusual case exhibiting cribriform aspect. Quintessence Int 2008;39:777–781 [PubMed] [Google Scholar]
- 20.Ide F, Mishima K, Saito I, Kusama K. Rare peripheral odontogenic tumors: report of 5 cases and comprehensive review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;106:e22–28 [DOI] [PubMed] [Google Scholar]
- 21.Vasconcelos BC, Frota R, Cardoso AB, Porto GG, Carneiro SC. Adenomatoid odontogenic tumor. Braz J Otorhinolaryngol 2008;74:315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Jivan V, Altini M, Meer S, Mahomed F. Adenomatoid odontogenic tumor (AOT) originating in a unicystic ameloblastoma: a case report. Head Neck Pathol 2007;1:146–149 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Chuan-Xiang Z, Yan G. Adenomatoid odontogenic tumor: a report of a rare case with recurrence. J Oral Pathol Med 2007;36:440–443 [DOI] [PubMed] [Google Scholar]
- 24.Nonaka CF, de Souza LB, Quinderé LB. Adenomatoid odontogenic tumour associated with dentigerous cyst--unusual case report. Braz J Otorhinolaryngol 2007;73:129–131 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kaminagakura E, Costa MS, Lopes MC, de Almeida OP. Extrafollicular adenomatoid odontogenic tumor: a case report. Gen Dent 2007;55:141–142 [PubMed] [Google Scholar]
- 26.Vera Sempere FJ, Artes Martínez MJ, Vera Sirera B, Bonet Marco J. Follicular adenomatoid odontogenic tumor: immunohistochemical study. Med Oral Patol Oral Cir Bucal 2006;11:E305–308 [PubMed] [Google Scholar]
- 27.Jham BC, Passos JB, Vieira doCarmo MA, Gomes CO, Mesquita RA. Adenomatoid odontogenic tumor originated in the periodontal ligament. Oral Oncol Extra 2006;42:268–271 [Google Scholar]
- 28.Nigam S, Gupta SK, Chaturvedi KU. Adenomatoid odontogenic tumor—a rare cause of jaw swelling. Braz Dent J 2005;16:251–253 [DOI] [PubMed] [Google Scholar]
- 29.Handschel JG, Depprich RA, Zimmermann AC, Braunstein S, Kübler NR. Adenomatoid odontogenic tumor of the mandible: review of the literature and report of a rare case. Head Face Med 2005;1:3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Motamedi MH, Shafeie HA, Azizi T. Salvage of an impacted canine associated with an adenomatoid odontogenic tumour: a case report. Br Dent J 2005;199:89–90 [DOI] [PubMed] [Google Scholar]
- 31.Effiom OA, Odukoya O. Adenomatoid odontogenic tumour: a clinico-pathological analysis and melanin pigmentation study of 31 Nigerian cases. Niger Postgrad Med J 2005;12:131–135 [PubMed] [Google Scholar]
- 32.Bravo M, White D, Miles L, Cotton R. Adenomatoid odontogenic tumor mimicking a dentigerous cyst. Int J Pediatr Otorhinolaryngol 2005;69:1685–1688 [DOI] [PubMed] [Google Scholar]
- 33.Leon JE, Mata GM, Fregnani ER, Carlos-Bregni R, de Almeida OP, Mosqueda-Taylor A, et al. Clinicopathological and immunohistochemical study of 39 cases of adenomatoid odontogenic tumour: a multicentric study. Oral Oncol 2005;41:835–842 [DOI] [PubMed] [Google Scholar]
- 34.Sato D, Matsuzaka K, Yama M, Kakizawa T, Inoue T. Adenomatoid odontogenic tumor arising from the mandibular molar region: a case report and review of the literature. Bull Tokyo Dent Coll 2004;45:223–227 [DOI] [PubMed] [Google Scholar]
- 35.Batra P, Prasad S, Parkash H. Adenomatoid odontogenic tumour: review and case report. J Can Dent Assoc 2005;71:250–253 [PubMed] [Google Scholar]
- 36.Asaumi J, Yanagi Y, Konouchi H, Hisatomi M, Matsuzaki H, Shigehara H, et al. Assessment of MRI and dynamic contrast-enhanced MRI in the differential diagnosis of adenomatoid odontogenic tumor. Eur J Radiol 2004;51:252–256 [DOI] [PubMed] [Google Scholar]
- 37.Walker LM, Wood AJ, McDonald A, Carpenter W. Unerupted mandibular second primary molar with an unusual histopathological finding: a case report. J Dent Child (Chic) 2004;71:77–79 [PubMed] [Google Scholar]
- 38.Olgaç V, Köseoğlu BG, Kasapoğlu C. Adenomatoid odontogenic tumor: a report of an unusual maxillary lesion. Quintessence Int 2003;34:686–688 [PubMed] [Google Scholar]
- 39.Larsson A, Swartz K, Heikinheimo K. A case of multiple AOT-like jawbone lesions in a young patient-a new odontogenic entity? J Oral Pathol Med 2003;32:55–62 [DOI] [PubMed] [Google Scholar]
- 40.Konouchi H, Asaumi J, Yanagi Y, Hisatomi M, Kishi K. Adenomatoid odontogenic tumor: correlation of MRI with histopathological findings. Eur J Radiol 2002;44:19–23 [DOI] [PubMed] [Google Scholar]
- 41.Philipsen HP, Srisuwan T, Reichart PA. Adenomatoid odontogenic tumor mimicking a periapical (radicular) cyst: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;94:246–248 [DOI] [PubMed] [Google Scholar]
- 42.Takahashi K, Yoshino T, Hashimoto S. Unusually large cystic adenomatoid odontogenic tumour of the maxilla: case report. Int J Oral Maxillofac Surg 2001;30:173–175 [DOI] [PubMed] [Google Scholar]
- 43.Bulut E, Tasar F, Akkocaoglu M, Ruacan S. An adenomatoid odontogenic tumor with unusual clinical features. J Oral Sci 2001;43:283–286 [DOI] [PubMed] [Google Scholar]
- 44.Blumenthal NM, Mostofi R. Repair of an intrabony defect from an adenomatoid odontogenic tumor. J Periodontol 2000;71:1637–1640 [DOI] [PubMed] [Google Scholar]
- 45.Lee JK, Lee KB, Hwang BN. Adenomatoid odontogenic tumor: a case report. J Oral Maxillofac Surg 2000;58:1161–1164 [DOI] [PubMed] [Google Scholar]
- 46.Damm DD, Fantasia JE. Failure of eruption. Adenomatoid odontogenic tumor. Gen Dent 2000;48:650–722 [PubMed] [Google Scholar]
- 47.Garcia-Pola Vallejo M, Gonzalez Garcia M, Lopez-Arranz JS, Herrero Zapatero A. Adenomatoid odontogenic tumor arising in a dental cyst: report of unusual case. J Clin Pediatr Dent 1998;23:55–58 [PubMed] [Google Scholar]
- 48.Dayi E, Gürbüz G, Bilge OM, Ciftcioğlu MA. Adenomatoid odontogenic tumour (adenoameloblastoma). Case report and review of the literature. Aust Dent J 1997;42:315–318 [DOI] [PubMed] [Google Scholar]
- 49.Curran AE, Miller EJ, Murrah VA. Adenomatoid odontogenic tumor presenting as periapical disease. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997;84:557–560 [DOI] [PubMed] [Google Scholar]
- 50.Holroyd I, Rule DC. Adenomatoid odontogenic tumour in a 12-year-old boy. Int J Paediatr Dent 1997;7:101–106 [DOI] [PubMed] [Google Scholar]
- 51.Kearns GJ, Smith R. Adenomatoid odontogenic tumour: an unusual cause of gingival swelling in a 3-year-old patient. Br Dent J 1996;181:380–382 [DOI] [PubMed] [Google Scholar]
- 52.Takeda Y, Shimono M. Adenomatoid odontogenic tumor with extensive formation of tubular dentin. Bull Tokyo Dent Coll 1996;37:189–193 [PubMed] [Google Scholar]
- 53.Siar CH, Ong ST, Ng KH. Adenomatoid odontogenic tumour: a case study with radiographic differential diagnostic considerations. Singapore Dent J 1996;21:19–22 [PubMed] [Google Scholar]
- 54.Miyake M, Nagahata S, Nishihara J, Ohbayashi Y. Combined adenomatoid odontogenic tumor and calcifying epithelial odontogenic tumor: report of case and ultrastructural study. J Oral Maxillofac Surg 1996;54:788–93 [DOI] [PubMed] [Google Scholar]
- 55.Zeitoun IM, Dhanrajani PJ, Mosadomi HA. Adenomatoid odontogenic tumor arising in a calcifying odontogenic cyst. J Oral Maxillofac Surg 1996;54:634–637 [DOI] [PubMed] [Google Scholar]
- 56.Vitkus R, Meltzer JA. Repair of a defect following the removal of a maxillary adenomatoid odontogenic tumor using guided tissue regeneration. A case report. J Periodontol 1996;67:46–50 [DOI] [PubMed] [Google Scholar]
- 57.Arotiba JT, Ogunbiyi JO, Ajagbe HA. Adenomatoid odontogenic tumours in Ibadan, Nigeria. East Afr Med J 1995;72:783–786 [PubMed] [Google Scholar]
- 58.Geist SM, Mallon HL. Adenomatoid odontogenic tumor: report of an unusually large lesion in the mandible. J Oral Maxillofac Surg 1995;53:714–717 [DOI] [PubMed] [Google Scholar]
- 59.Carr RF, Foster LD, Gilliam CH, Evans G. Odontogenic adenomatoid tumors associated with orthodontic treatment. Am J Orthod Dentofacial Orthop 1995;107:648–650 [DOI] [PubMed] [Google Scholar]
- 60.Takeda Y. Induction of osteodentin and abortive enamel in adenomatoid odontogenic tumor. Ann Dent 1995;54:61–63 [PubMed] [Google Scholar]
- 61.Unal T, Cetingul E, Gunbay T. Peripheral adenomatoid odontogenic tumor: birth of a term. J Clin Pediatr Dent 1995;19:139–142 [PubMed] [Google Scholar]
- 62.Haring JI. Case #7. Adenomatoid odontogenic tumor. RDH 1994;14:12. [PubMed] [Google Scholar]
- 63.Philipsen HP, Samman N, Ormiston IW, Wu PC, Reichart PA. Variants of the adenomatoid odontogenic tumor with a note on tumor origin. J Oral Pathol Med 1992;21:348–52 [DOI] [PubMed] [Google Scholar]
- 64.Nomura M, Tanimoto K, Takata T, Shimosato T. Mandibular adenomatoid odontogenic tumor with unusual clinicopathologic features. J Oral Maxillofac Surg 1992;50:282–285 [DOI] [PubMed] [Google Scholar]
- 65.Tajima Y, Sakamoto E, Yamamoto Y. Odontogenic cyst giving rise to an adenomatoid odontogenic tumor: report of a case with peculiar features. J Oral Maxillofac Surg 1992;50:190–193 [DOI] [PubMed] [Google Scholar]
- 66.Layton SA. Adenomatoid odontogenic tumour. Report of an unusual lesion in the posterior maxilla. Dentomaxillofac Radiol 1992;21:50–52 [DOI] [PubMed] [Google Scholar]
- 67.Raubenheimer EJ, Seeliger JE, van Heerden WF, Dreyer AF. Adenomatoid odontogenic tumour: a report of two large lesions. Dentomaxillofac Radiol 1991;20:43–45 [DOI] [PubMed] [Google Scholar]
- 68.Warter A, George-Diolombi G, Chazal M, Ango A. Melanin in a dentigerous cyst and associated adenomatoid odontogenic tumor. Cancer 1990;66:786–788 [DOI] [PubMed] [Google Scholar]
- 69.Aldred MJ, Gray AR. A pigmented adenomatoid odontogenic tumor. Oral Surg Oral Med Oral Pathol 1990;70:86–89 [DOI] [PubMed] [Google Scholar]
- 70.Mendis BR, MacDonald DG. Adenomatoid odontogenic tumour. A survey of 21 cases from Sri Lanka. Int J Oral Maxillofac Surg 1990;19:141–143 [DOI] [PubMed] [Google Scholar]
- 71.Toida M, Hyodo I, Okuda T, Tatematsu N. Adenomatoid odontogenic tumor: report of two cases and survey of 126 cases in Japan. J Oral Maxillofac Surg 1990;48:404–408 [DOI] [PubMed] [Google Scholar]
- 72.Watkins KE, Rushton VE. Adenomatoid odontogenic tumour: report of a case demonstrating the importance of adequate radiology. Proc Br Soc Dent Maxillofac Radiol 1990;4:5–10 [PubMed] [Google Scholar]
- 73.Takeda Y. Pigmented adenomatoid odontogenic tumour. Report of an undescribed case and review of the literature of pigmented intraosseous odontogenic lesions. Virchows Arch A Pathol Anat Histopathol 1989;415:571–575 [DOI] [PubMed] [Google Scholar]
- 74.Valderrama LS. Dentigerous cyst with intracystic adenomatoid odontogenic tumor and complex odontoma. J Philipp Dent Assoc 1988;41:35–41 [PubMed] [Google Scholar]
- 75.Mehta DS, Mehta MJ. Adenomatoid odontogenic tumour: report of a case. Singapore Dent J 1987;12:71–73 [PubMed] [Google Scholar]
- 76.Chong HuatSiar , Kok Han N. Combined calcifying epithelial odontogenic tumor and adenomatoid odontogenic tumor. Int J Oral Maxillofac Surg 1987;16:214–216 [DOI] [PubMed] [Google Scholar]
- 77.Thomas SL. Adenomatoid odontogenic tumor. Report of a case in the mandible. J Kans Dent Assoc 1987;71:10–11 [PubMed] [Google Scholar]
- 78.Kuntz AA, Reichart PA. Adenomatoid odontogenic tumor mimicking a globulo-maxillary cyst. Int J Oral Maxillofac Surg 1986;15:632–636 [DOI] [PubMed] [Google Scholar]
- 79.Webb DJ, Colman MF, Moore L, Correll RW. Expansile radiolucent mass in the maxilla. J Am Dent Assoc 1985;111:474–476 [DOI] [PubMed] [Google Scholar]
- 80.Ajagbe HA, Daramola JO, Junaid TA, Ajagbe AO. Adenomatoid odontogenic tumor in a black African population: report of thirteen cases. J Oral Maxillofac Surg 1985;43:683–687 [DOI] [PubMed] [Google Scholar]
- 81.Parkash H, Sidhu SS, Chopra P. Adenomatoid odontogenic tumour of the jaws. J Dent 1984;12:297–301 [DOI] [PubMed] [Google Scholar]
- 82.Sofat JR, Sabharwal BD. Adenomatoid odontogenic tumour—a case report. J Indian Dent Assoc 1984;56:423–424, 428 [PubMed] [Google Scholar]
- 83.Poulson TC, Greer RO., Jr Adenomatoid odontogenic tumor: clinicopathologic and ultrastructural concepts. J Oral Maxillofac Surg 1983;41:818–824 [DOI] [PubMed] [Google Scholar]
- 84.Saito I, Ide F, Umemura S. An unusual adenomatoid odontogenic tumor presenting as a residual cyst. J Oral Maxillofac Surg 1983;41:534–535 [DOI] [PubMed] [Google Scholar]
- 85.Damm DD, White DK, Drummond JF, Poindexter JB, Henry BB. Combined epithelial odontogenic tumor: adenomatoid odontogenic tumor and calcifying epithelial odontogenic tumor. Oral Surg Oral Med Oral Pathol 1983;55:487–496 [DOI] [PubMed] [Google Scholar]
- 86.Glickman R, Super S, SunderRaj M, Jain R, Chaudhry A. An adenomatoid odontogenic tumor simulating globulo-maxillary cyst. J Oral Med 1983;38:26–30 [PubMed] [Google Scholar]
- 87.Arole FO, Arain AH, Taiwo EO. Adenomatoid odontogenic tumour (adeno-ameloblastoma). Odontostomatol Trop 1982;5:171–175 [PubMed] [Google Scholar]
- 88.Gupta MK, Gupta DS. Adenomatoid odontogenic tumor (a case report). J Indian Dent Assoc 1982;54:331–333 [PubMed] [Google Scholar]
- 89.Stroncek GG, Acevedo A, Higa LH. An atypical odontogenic adenomatoid tumor and review of the literature. J Oral Med 1981;36:102–105 [PubMed] [Google Scholar]
- 90.Yamamoto H, Kozawa Y, Hirai G, Hagiwara T, Nakamura T. Adenomatoid odontogenic tumor: light and electron microscopic study. Int J Oral Surg 1981;10:272–278 [DOI] [PubMed] [Google Scholar]
- 91.Schlosnagle DC, Someren A. The ultrastructure of the adenomatoid odontogenic tumor. Oral Surg Oral Med Oral Pathol 1981;52:154–161 [DOI] [PubMed] [Google Scholar]
- 92.Gupta NP, Gupta SC, Munshi AK. Adenomatoid odontogenic tumour. Indian J Cancer 1980;17:272–275 [PubMed] [Google Scholar]
- 93.Bedrick AE, Solomon MP. The adenomatoid odontogenic tumor: an unusual clinical presentation. Oral Surg Oral Med Oral Pathol 1979;48:143–145 [DOI] [PubMed] [Google Scholar]
- 94.Omara LM. Adenomatoid odontogenic tumor. Egypt Dent J 1979;25:279–289 [PubMed] [Google Scholar]
- 95.Smith RR, Olson JL, Hutchins GM, Crawley WA, Levin LS. Adenomatoid odontogenic tumor: ultrastructural demonstration of two cell types and amyloid. Cancer 1979;43:505–511 [DOI] [PubMed] [Google Scholar]
- 96.Mars M. Adenomatoid odontogenic tumour (adenoameloblastoma). A case report. Br Dent J 1978;144:45–46 [DOI] [PubMed] [Google Scholar]
- 97.De AndradeSobrinho J, de Carvalho MB, Rapoport A, Saba LM. Odontogenic adenomatoid tumor of the mandible (adenoameloblastoma). Int Surg 1978;63:39–42 [PubMed] [Google Scholar]
- 98.Khanna S, Khanna NN, Shrivastava AB, Gupta IM. Adenomatoid odontogenic tumor. Ear Nose Throat J 1977;56:468–472 [PubMed] [Google Scholar]
- 99.Khan MY, Kwee H, Schneider LC, Saber I. Adenomatoid odontogenic tumor resembling a globulomaxillary cyst: light and electron microscopic studies. J Oral Surg 1977;35:739–742 [PubMed] [Google Scholar]
- 100.Solarin EO, Mosadomi A. Adenomatoid odontogenic tumour (adenoameloblastoma). Br J Oral Surg 1977;15:26–31 [DOI] [PubMed] [Google Scholar]
- 101.Swinson TW. An extraosseous adenomatoid odontogenic tumour: a case report. Br J Oral Surg 1977;15:32–36 [DOI] [PubMed] [Google Scholar]
- 102.Tsaknis PJ, Carpenter WM, Shade NL. Odontogenic adenomatoid tumor: report of case and review of the literature. J Oral Surg 1977;35:146–149 [PubMed] [Google Scholar]
- 103.Parichatikanond P, Dharamadhach A, Damrongvadha P, Benjarasmeroj S. Adenomatoid odontogenic tumour. J Med Assoc Thai 1976;59:80–86 [PubMed] [Google Scholar]
- 104.Milobsky L, Milobsky SA, Miller GM. Adenomatoid odontogenic tumor (adenoameloblastoma). Report of a case. Oral Surg Oral Med Oral Pathol 1975;40:681–685 [DOI] [PubMed] [Google Scholar]
- 105.Kestner AT, Vatral JJ, White DK. Odontogenic adenomatoid tumor. J N J Dent Assoc 1975;47:27–29 [PubMed] [Google Scholar]
- 106.Hacihanefioðlu U. The adenomatoid odontogenic tumor. Oral Surg Oral Med Oral Pathol 1974;38:65–73 [DOI] [PubMed] [Google Scholar]
- 107.Meyer I, Giunta JL. Adenomatoid odontogenic tumor (adenoameloblastoma): report of case. J Oral Surg 1974;32:448–451 [PubMed] [Google Scholar]
- 108.Yazdi I, Nowparast B. Extraosseous adenomatoid odontogenic tumor with special reference to the probability of the basal-cell layer of oral epithelium as a potential source of origin. Report of a case. Oral Surg Oral Med Oral Pathol 1974;37:249–256 [DOI] [PubMed] [Google Scholar]
- 109.Seymour RL, Funke FW, Irby WB. Adenoameloblastoma. Report of a case and review of the literature. Oral Surg Oral Med Oral Pathol 1974;38:860–865 [DOI] [PubMed] [Google Scholar]
- 110.Khin U, Sanders B, Kasper E, Adilman H. Adenomatoid odontogenic tumor. J Oral Surg 1973;31:607–612 [PubMed] [Google Scholar]
- 111.Fahim MS. Ameloblastic adenomatoid tumor (adenomeloblastoma). Egypt Dent J 1973;19:291–300 [PubMed] [Google Scholar]
- 112.Chambers KS. The adenoameloblastoma. Br J Oral Surg 1973;10:310–320 [DOI] [PubMed] [Google Scholar]
- 113.Goracy E, Stratigos GT. Adenoameloblastoma: report of case. J Am Dent Assoc 1973;86:672–674 [DOI] [PubMed] [Google Scholar]
- 114.Berk RS, Baden E, Ladov M, Williams AC. Adenoameloblastoma (odontogenic adenomatoid tumor): report of case. J Oral Surg 1972;30:201–208 [PubMed] [Google Scholar]
- 115.Abrams AM, Melrose RJ. Odontogenic adenomatoid tumor. Clinical pathologic Conference No. 19. J South Calif Dent Assoc 1972;40:108–111 [PubMed] [Google Scholar]
- 116.Martis CS, Karakasis DT. Adenoameloblastoma. Case report. Plast Reconstr Surg 1972;50:409–411 [PubMed] [Google Scholar]
- 117.Seimley DC, Jacoby JK, Kolodny SC. Adenoameloblastoma: report of case. J Oral Surg 1971;29:133–135 [PubMed] [Google Scholar]
- 118.McGinnis JP, Jr, Turner JE, Holt S. Adenoameloblastoma- report of a case. J Tenn State Dent Assoc 1970;50:235–238 [PubMed] [Google Scholar]
- 119.Giansanti JS, Someren A, Waldron CA. Odontogenic adenomatoid tumor (adenoameloblastoma). Survey of 3 cases. Oral Surg Oral Med Oral Pathol 1970;30:69–88 [DOI] [PubMed] [Google Scholar]
- 120.Burzynski NJ, Rosenberg C, Crider R, Martin TH. The ameloblastic adenomatoid tumor. Oral Surg Oral Med Oral Pathol 1970;29:880–882 [DOI] [PubMed] [Google Scholar]
- 121.Martinelli C, Melhado RM, Dos Santos-Pinto R. Adenoameloblastoma. Histologic and histochemical study in one case. Oral Surg Oral Med Oral Pathol 1969;28:534–541 [DOI] [PubMed] [Google Scholar]
- 122.Abrams AM, Melrose RJ, Howell FV. Adenoameloblastoma. A clinical pathologic study of ten new cases. Cancer 1968;22:175–185 [DOI] [PubMed] [Google Scholar]
- 123.Spouge JD. The adenoameloblastoma. Oral Surg Oral Med Oral Pathol 1967;23:470–482 [DOI] [PubMed] [Google Scholar]
- 124.Rosenberg CJ, Cruz J. The so-called Adenoameloblastoma. Report of two cases. Oral Surg Oral Med Oral Pathol 1963;16:1459–1464 [DOI] [PubMed] [Google Scholar]
- 125.Link JF. Adenoameloblastoma of the maxilla: report of case. J Oral Surg Anesth Hosp Dent Serv 1963;21:432–434 [PubMed] [Google Scholar]
- 126.Ishikawa G, Mori K. A histopathological study on the adenomatoid ameloblastoma. Report of four cases. Acta Odontol Scand 1962;20:419–432 [DOI] [PubMed] [Google Scholar]
- 127.Oehlers FA. The so-called adenoameloblastoma. Oral Surg Oral Med Oral Pathol 1961;14:712–725 [DOI] [PubMed] [Google Scholar]
- 128.Tiecke RW, Shira RB. Adenoameloblastoma: report of case. J Oral Surg Anesth Hosp Dent Serv 1961;19:252–254 [PubMed] [Google Scholar]
- 129.Topazian RG, Simon GT. Adenoameloblastoma. Report of three cases. Oral Surg Oral Med Oral Pathol 1960;13:1038–1045 [DOI] [PubMed] [Google Scholar]
- 130.Gorlin RJ, Chaudhry AP. Adenoameloblastoma. Oral Surg Oral Med Oral Pathol 1958;11:762–768 [DOI] [PubMed] [Google Scholar]
- 131.Bernier JL, Tiecke RW. Adenoameloblastoma; report of nine cases. Oral Surg Oral Med Oral Pathol 1956;9:1304–1317 [DOI] [PubMed] [Google Scholar]
- 132.Thoma KH. Adenoameloblastoma. Oral Surg Oral Med Oral Pathol 1955;8:441–444 [DOI] [PubMed] [Google Scholar]
- 133.Bernier JL, Tiecke RW. Adenoameloblastoma. J Oral Surg (Chic) 1950;8:259–261 [PubMed] [Google Scholar]
- 134.White SC. Computer-aided differential diagnosis of oral radiographic lesions. Dentomaxillofac Radiol 1989;18:53–59 [DOI] [PubMed] [Google Scholar]
- 135.Zlotogorski A, Buchner A, Kaffe I, Schwartz-Arad D. Radiological features of central haemangioma of the jaws. Dentomaxillofac Radiol 2005;34:292–296 [DOI] [PubMed] [Google Scholar]
- 136.Philipsen HP, Reichart PA, Zhang Kh, Nikai H, Yu QX. Adenomatoid odontogenic tumor: biologic profile based on 499 cases. J Oral Pathol Med 1991;20:149–158 [DOI] [PubMed] [Google Scholar]
- 137.Swasdison S, Dhanuthai K, Jainkittivong A, Philipsen HP. Adenomatoid odontogenic tumors: an analysis of 67 cases in a Thai population. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105:210–215 [DOI] [PubMed] [Google Scholar]
- 138.Arotiba GT, Arotiba JT, Olaitan AA, Ajayi OF. The adenomatoid odontogenic tumor: an analysis of 57 cases in a Black African population. J Oral Maxillofac Surg 1997;55:146–148 [DOI] [PubMed] [Google Scholar]
- 139.Dare A, Yamaguchi A, Yoshiki S, Okano T. Limitation of panoramic radiography in diagnosing adenomatoid odontogenic tumors. Oral Surg Oral Med Oral Pathol 1994;77:662–668 [DOI] [PubMed] [Google Scholar]
- 140.Toida M, Hyodo I, Okuda T, Tatematsu N. Adenomatoid odontogenic tumor: report of two cases and survey of 126 cases in Japan. J Oral Maxillofac Surg 1990;48:404–408 [DOI] [PubMed] [Google Scholar]
- 141.Mendis BR, MacDonald DG. Adenomatoid odontogenic tumour. A survey of 21 cases from Sri Lanka. Int J Oral Maxillofac Surg 1990;19:141–143 [DOI] [PubMed] [Google Scholar]
- 142.Effiom OA, Odukoya O. Adenomatoid odontogenic tumour: a clinico- pathological analysis and melanin pigmentation study of 31 Nigerian cases. Niger Postgrad Med J 2005;12:131–135 [PubMed] [Google Scholar]
- 143.Ochsenius G, Ortega A, Godoy L, Penaflel C, Escobar E. Odontogenic tumors in Chile: a study of 362 cases. J Oral Pathol Med 2002;31:415–420 [DOI] [PubMed] [Google Scholar]
- 144.Buchner A, Merrell PW, Carpenter WM. Relative frequency of central odontogenic tumors: a study of 1,088 cases from Northern California and comparison to studies from other parts of the world. J Oral Maxillofac Surg 2006;64:1343–1352 [DOI] [PubMed] [Google Scholar]
- 145.Buchner A. The central (intraosseous) calcifying odontogenic cyst: an analysis of 215 cases. J Oral Maxillofac Surg 1991;49:330–339 [DOI] [PubMed] [Google Scholar]
- 146.Neville BW, Dam DD, Allen CM, Bouquot JE. Oral and maxillofacial pathology. 3rd edn. St Louis, MO: Saunders Elsevier; 2009 [Google Scholar]