

Abstract
OBJECTIVE
Specific autoantibodies characterize type 1 diabetes in childhood but are also found in adult-onset diabetes, even when initially non–insulin requiring, e.g., with latent autoimmune diabetes (LADA). We aimed to characterize adult-onset autoimmune diabetes.
RESEARCH DESIGN AND METHODS
We consecutively studied 6,156 European diabetic patients attending clinics within 5 years of diagnosis (age range, 30–70 years) examined cross-sectionally clinically and for GAD antibodies (GADA) and antibodies to insulinoma-associated antigen-2 (IA-2A) and zinc-transporter 8 (ZnT8A).
RESULTS
Of 6,156 patients, 541 (8.8%) had GADA and only 57 (0.9%) IA-2A or ZnT8A alone. More autoantibody-positive than autoantibody-negative patients were younger, leaner, on insulin (49.5 vs. 13.2%), and female (P < 0.0001 for each), though LADA patients (9.7% of total) did not show categorically distinct clinical features from autoantibody-negative type 2 diabetes. Similarly, more GADA patients with high (>200 World Health Organization IU) (n = 403) compared with low (n = 138) titer were female, lean, and insulin treated (54.6 vs. 39.7%) (P < 0.02 for each). Autoantibody-positive patients usually had GADA (541 of 598; 90.5%) and had LADA more often than type 1 autoimmune diabetes (odds ratio 3.3).
CONCLUSIONS
Adult-onset autoimmune diabetes emerges as a prevalent form of autoimmune diabetes. Our results indicate that adult-onset autoimmune diabetes in Europe encompasses type 1 diabetes and LADA in the same broad clinical and autoantibody-positive spectrum. At diagnosis, patients with adult-onset autoimmune diabetes are usually non–insulin requiring and clinically indistinguishable from patients with type 2 diabetes, though they tend to be younger and leaner. Only with screening for autoantibodies, especially GADA, can they be identified with certainty.
Type 1 diabetes is an autoimmune disease in which insulin deficiency results from immune-mediated destruction of insulin-secreting islet cells (1). Type 1 diabetes was formerly called insulin-dependent diabetes, reflecting the severity of the destructive process and the requirement for insulin therapy in all cases. The majority of patients with type 1 diabetes have autoantibodies in their peripheral blood, and these autoantibodies can predict the future onset of the disease (1). Autoimmune diabetes is characterized by specific autoantibodies such as GAD autoantibodies (GADA), insulinoma-associated antigen-2 autoantibodies (IA-2A) or zinc-transporter 8 autoantibodies (ZnT8A). Type 1 diabetes is the most prevalent form of diabetes in children but also occurs in adults (1). A proportion of patients with adult-onset initially non–insulin-requiring diabetes have diabetes-associated autoantibodies and are thought to have a form of autoimmune diabetes called latent autoimmune diabetes of adult onset (LADA) (2,3). Descriptions of the proportions of LADA patients in clinical case series vary, in part through selection biases such as ascertainment of nonobese cases (4), insulin-naïve cases (5), or treatment-naïve cases (6) or the inclusion of impaired glucose tolerance (7). These studies have established that patients with autoimmune diabetes, as characterized by the presence of GADAs, have a clinical phenotype distinct from initially non–insulin-requiring diabetic patients without GADAs who are mostly designated as type 2 diabetic (1–9). There are no studies of the relative frequency of type 1 diabetes and LADA in adults.
The key uncertainty regarding adult-onset diabetic patients is whether LADA is distinct from type 1 diabetes or more common (10,11). Furthermore, it is as yet unclear which factors are associated with progression toward insulin therapy in adult-onset autoimmune diabetes. Action LADA is a European study that seeks to address these questions by ascertaining adult-onset diabetic patients presenting to nine European hospital-based clinics (some recruiting from a community of primary care settings; see below) within a defined period. We hypothesized that autoimmune diabetes would be prevalent in Europe, that LADA would be more prevalent than type 1 diabetes, and that these two would show phenotypic differences. Furthermore, we predicted that GADA could detect most cases of autoimmune diabetes.
RESEARCH DESIGN AND METHODS
The study design is cross-sectional and includes adult-onset diabetic patients, recruited between 2004 and 2007, from nine European countries: Finland, Odense (Denmark), Vienna (Austria), Belfast (Northern Ireland), Düsseldorf (Germany), London (U.K.), Lyon (France), Rome (Italy), and Barcelona (Spain). Each center is involved in Action LADA, a European Union–funded multicenter European study with the aim of identifying risk factors for adult-onset autoimmune diabetes (www.actionlada.org). All centers recruited patients (aged 30–70 years, with primary diabetes, and diagnosed within the past 5 years). Four recruited from a community or primary care setting (Helsinki, Düsseldorf, Rome, and Odense). The remaining five centers (Vienna, London, Belfast, Rome, Barcelona, and Lyon) recruited patients in a hospital setting.
Patients were designated with diabetes according to standard criteria, and LADA was defined as follows: patients 1) aged 30–70 years, 2) with diabetes-associated autoantibodies, and 3) who did not require insulin treatment for at least 6 months postdiagnosis (12). Type 1 autoimmune diabetic patients were defined as case subjects with diabetes and with diabetes-associated autoantibodies in whom insulin was started at diagnosis or within 1 month of diagnosis. Inclusion criteria for all patients were that patients have diabetes (with at least two recorded fasting blood glucose measurements ≥7 mmol/L) (12), that time from diagnosis was <5 years for all patients, and that patients were aged 30–70 years at the time of recruitment. Exclusion criteria were insufficient dataset, current pregnancy, renal disease with raised creatinine or proteinuria, or acute illness at the time of testing. Data on medication and risk factors were registered by the attending physician based upon the medical files. Serum and plasma samples were collected according to standard procedures and stored at −20°C.
Waist and hip circumferences were measured in a standardized procedure, and blood pressure was recorded locally for each subject. Blood pressure was measured at least twice in the sitting positions. Lipids and lipoproteins (serum total and HDL cholesterol and triglycerides) were determined by standardized assays at each center.
All patients were tested in a central laboratory (London) for serum GADA, IA-2A, and ZnT8A using established radioimmunoprecipitation assays (13,14). Positive results were duplicated, reducing false positives to <0.2%. In the 2003 Diabetes Antibody Standardization Program (DASP 2003) (London), assay characteristics were GADA sensitivity 72%, specificity 95%, and IA-2A sensitivity 68%, specificity 98% (15). In the latest DASP program (DASP 2010), GADA sensitivity was 90% and specificity 93%, IA-2A sensitivity 68% and specificity 95%, and ZnT8A sensitivity 60% and specificity 88% (M.I.H. and R.D.L., unpublished data). The pJH4·1 probe for ZnT8A was provided by Dr. J. Hutton (University of Colorado, Denver, CO) and is a synthetic molecule that combines cytoplasmic ZnT8 COOH-terminal domains with an immunoglobulin Cγ3 hinge sequence in a single-chain construct. It accounts for a ZnT8 dimer containing the protein epitopes 325Trp and 325Arg.
Each assay included serially diluted sera from a prediabetic individual; these in-house standards were diluted to an end point. A separate positive serum sample (equivalent to the World Health Organization [WHO] standard of 250 WHO units) was used as an in-house control to standardize each assay for unit calculation. The cutoff for positivity was selected arbitrarily based on the end point of the standard curve and further confirmed with Quantile-Quantile (Q-Q) probability plots.
Statistical analysis
Data are presented, where appropriate, as means SD, interquartile range, or odds ratios (ORs) (95% CI). The differences between groups were tested with χ2 test or Fisher exact test when appropriate. A logistic regression analysis was performed to evaluate confounding by covariables, with adjustment for sex, age of onset, disease duration, and ethnicity to calculate ORs. All analyses were performed using SPSS statistical software for Windows. A P value <0.05 was considered statistically significant. Q-Q probability plots were used to analyze the distribution of autoantibody measurements for normality. Observed antibody values were plotted along the horizontal axis against expected normal values under normality on the vertical axis using Blom proportion estimation formula. The study protocol is in accordance with the Declaration of Helsinki and was approved by local ethics committees in each study area. Informed written consent was obtained from all subjects before blood sampling. The study was approved by the U.K. National Research Ethics Committee (reference no. P/02/240).
RESULTS
Diabetes autoantibody prevalence and demographics
A total of 6,810 patients were screened for diabetes-associated autoantibodies from the samples received from the Action LADA cohort. Of these, 654 subjects were misclassified, owing to inappropriate age or disease duration, and were excluded. Of 6,156 subjects fulfilling the inclusion criteria, 84.6% were Caucasian, 2.5% Asian, 1.2% African, 4.5% of the Middle East, and 7.2% of other origins. Overall mean (SD) age was 54.4 (9.6) years, mean duration of diabetes was 2.2 (1.6) years, and 58.5% were male. Of these 6,156 patients, 598 (9.7%) were positive for at least one autoantibody (Table 1). Of these, 68.6% were positive for GADA only, 5.0% positive for IA-2A only, and 2.3% positive for ZnT8A only (Fig. 1). At least two autoantibody types were found in 144 (24.1%) patients. The determination of IA-2A and ZnT8A, in addition to GADA, modestly improved the recognition of autoimmune diabetes from 8.8 to 9.7% of the total study group. Within the entire cohort of patients with autoimmune diabetes, 541 of 598 (90.5%) were positive for GADA.
Table 1.
Features of any autoantibody-positive (GADA, IA-2A, or ZnT8A) versus autoantibody-negative patients
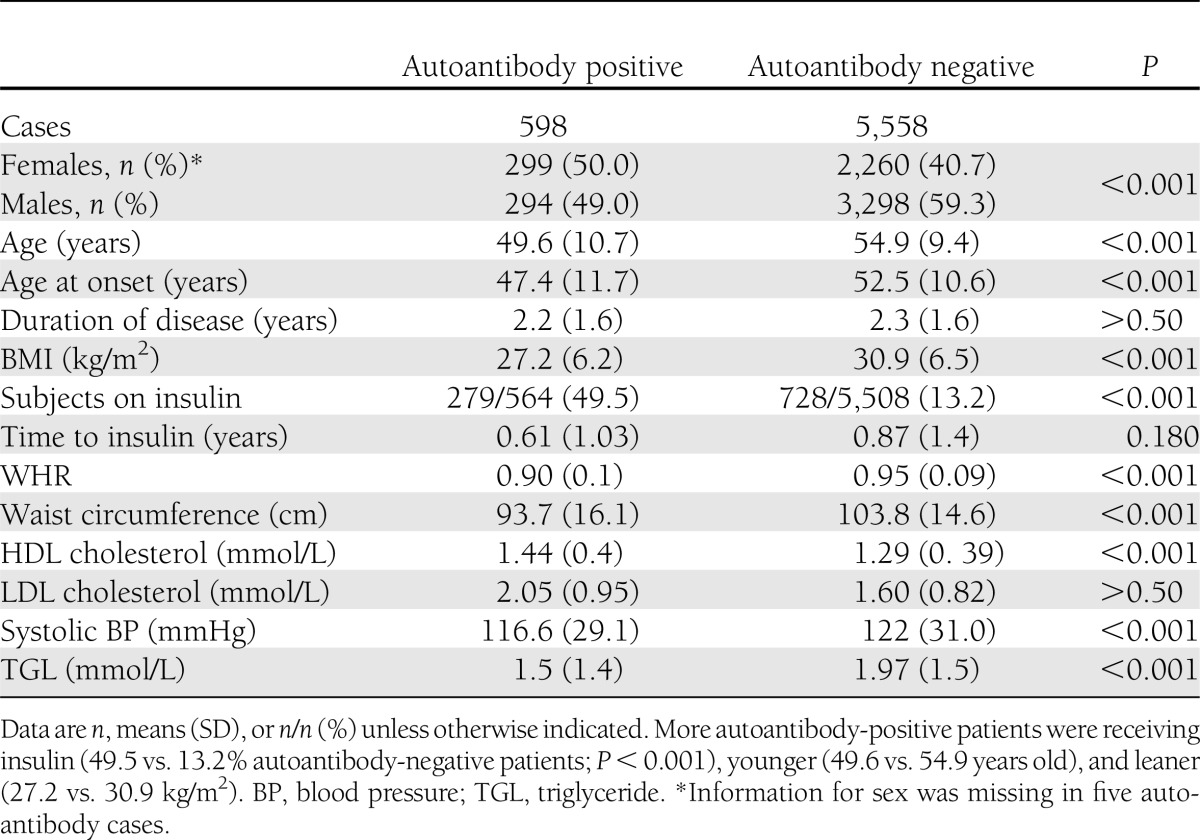
Figure 1.

Venn diagram of numbers of patients with GADA, IA-2A, or ZnT8A; n = 598 of 6,156 (9.8%). Of the autoantibody-positive samples, GADA was identified in 90% of the samples when an autoantibody was detected, with IA-2A and ZnT8A accounting for the remaining 10% of the autoantibodies detected. GADA, n = 541 (8.8%); IA-2A, n = 144 (2.3%); and ZnT8A, n = 110 (1.8%).
The demographics of the autoantibody-positive and -negative patients are shown in Table 1. GADA-positive patients in hospital-based clinics (10.0%) were more prevalent than among the community-based patients (7.8%) (P < 0.0001) (Supplementary Table 1). Autoantibody-positive patients compared with autoantibody-negative patients had a significantly lower mean age of onset (P < 0.001) (Table 1). Analysis of BMI was corrected for age of onset, sex, and duration of disease, and other analyses were corrected for age of onset, sex, duration of disease, and BMI. Of autoantibody-positive compared with autoantibody-negative patients after this correction, mean age, age of onset, BMI, waist-to-hip ratio (WHR), waist circumference, and systolic blood pressure were significantly lower (P < 0.001), while HDL cholesterol was higher (P < 0.001) (Table 1). No differences were seen in LDL cholesterol values (Table 1). More autoantibody-positive patients were receiving insulin at the time of examination (49.5% compared with 13.2% autoantibody-negative patients; P < 0.001); the proportion was similar in hospital-based and community-based clinics (45.5 and 51.4%, respectively) (Supplementary Table 1).
Diabetes phenotype by number of autoantibodies
Patients positive for at least two autoantibodies compared with those positive for a single antibody did not show relevant differences in any demographic or clinical parameters (data not shown). Moreover, patients with an autoantibody other than GADA or with low-titer GADA were leaner and more likely to be insulin treated than autoantibody-negative patients (Supplementary Table 2 and Supplementary Table 3).
Diabetes phenotypes by GADA titer
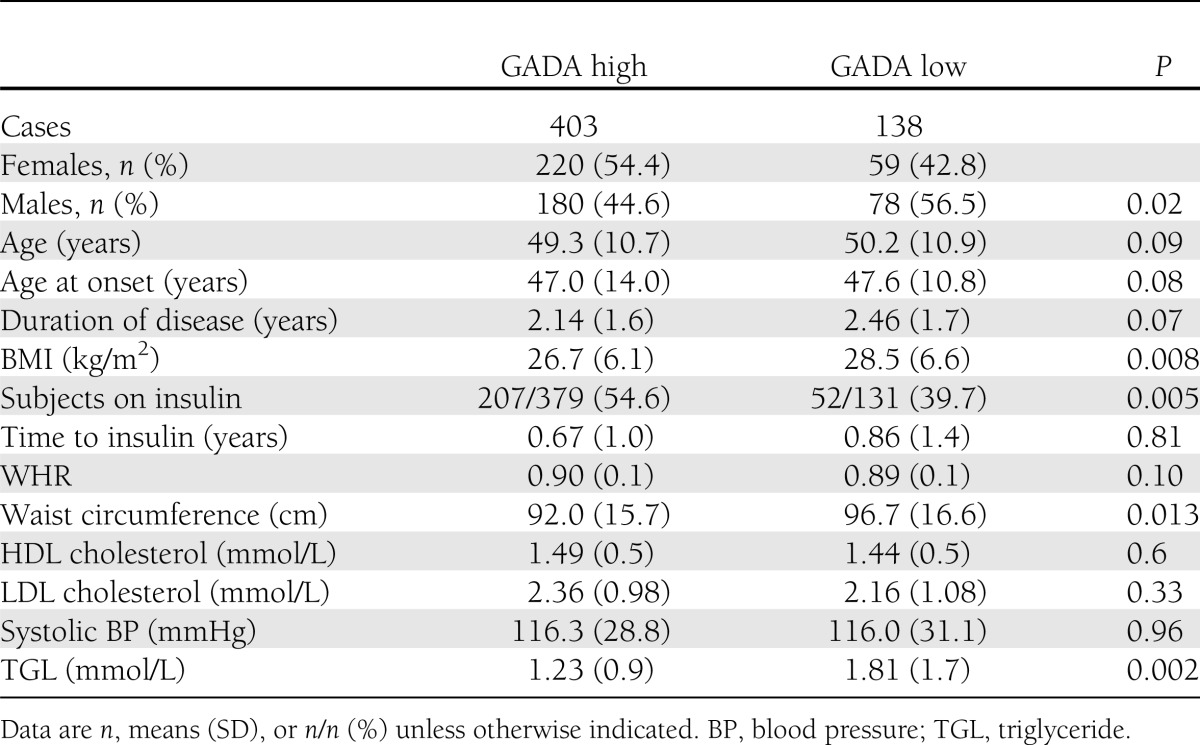
To further define autoantibody positivity, for autoantibody titers on the whole cohort we used the Q-Q plot analysis, and a laboratory cutoff set at 70 WHO units from the standard curves was confirmed, with a further inflection at 200 WHO units indicating high-titer GADA (Supplementary Fig. 1). Patients with high-titer GADA (n = 403), in contrast to low-titer GADA (n = 138), were more likely to be female and younger, have lower BMI (P < 0.01 for all comparisons), and lower serum triglycerides (P < 0.001), and more often be on insulin treatment (54.6 vs. 39.7%; P = 0.005) (Table 2). Compared with GADA-negative patients, high–GADA titer patients had lower waist circumference and WHR as well as higher HDL cholesterol, and more patients were insulin treated (P < 0.001 for all comparisons) (Tables 1 and 2). Compared with GADA-negative patients, the low–GADA titer group also had lower waist circumference, WHR, and BMI (P < 0.01 for all comparisons), as well as higher LDL cholesterol (P = 0.02), and more patients were insulin treated (P < 0.001) (Supplementary Table 3). Among all GADA-positive patients, GADA titer was directly correlated with age at diagnosis (r = 0.129, P = 0.010) and inversely correlated with WHR (r = −0.103, P = 0.047) but not BMI (r = −0.054, P = 0.24).
Table 2.
Features of GADA high- versus GADA low-titer patients
Comparative features of adult-onset type 1 diabetes and LADA
Of 598 patients positive for at least one autoantibody (GADA, IA-2A, or ZnT8A), 279 were on insulin; of these 279 insulin-treated autoantibody-positive patients, information on precise time to insulin therapy was available for 203, of whom 114 (56.2%) were designated as type 1 diabetic (started insulin at diagnosis and all autoantibody positive), 65 (32.0%) were classified as LADA (free of insulin for >6 months from diagnosis and autoantibody positive), and 24 (11.8%) were intermediate (started insulin within 6 months but after 1 month from diagnosis and autoantibody positive).
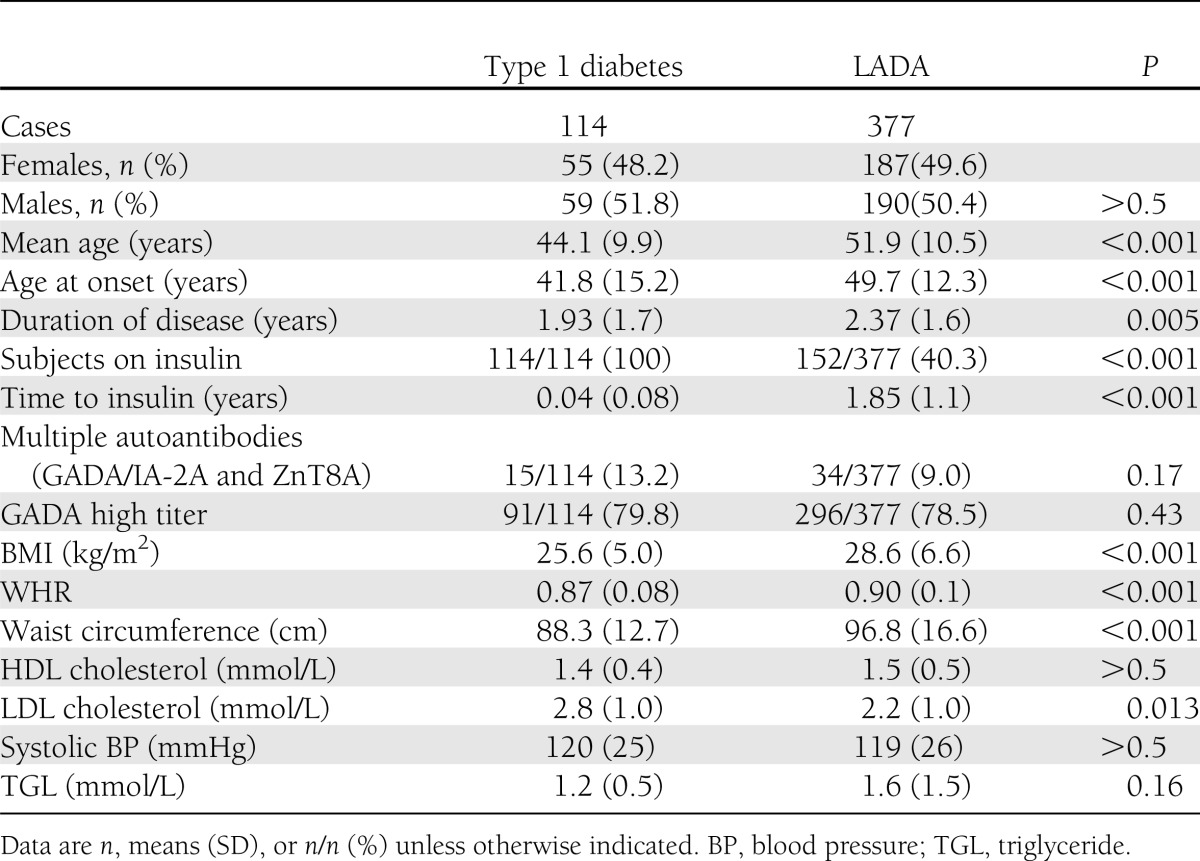
LADA was more prevalent than classic autoimmune type 1 diabetes (OR 3.3). Of autoantibody-positive patients, those classified as type 1 diabetic compared with LADA were younger and had a lower age of onset, BMI, waist circumference, and WHR (P < 0.001 for all comparisons) but higher LDL cholesterol (P = 0.013), whereas the number of patients with high GADA titer did not differ between the groups (80 vs. 79%) (Table 3).
Table 3.
Features of type 1 diabetic versus LADA patients
CONCLUSIONS
These observations show that adult-onset autoimmune diabetes is not rare, as it was reported in 9.7% of this large cohort of adult-onset diabetic patients diagnosed between 30 and 70 years of age attending primary and secondary care European centers. Similar studies have been much smaller with marked selection bias, usually ascertaining only patients with non–insulin-requiring diabetes (2–9). Nevertheless, several of these studies also found that ~10% (range 5–15) of patients with adult-onset diabetes have diabetes-associated autoantibodies, notably GADA (2–9). This present study is the largest to date and benefits from an analysis of all case subjects attending these clinics, irrespective of clinical features, as well as screening for three major diabetes-associated autoantibodies. Insulin autoantibodies, a feature of childhood-onset diabetes, were not included in our screening program, as we were studying adults. The proportion of case subjects classified with type 1 diabetes is probably exaggerated, as clinicians who had access to a local GADA assay result are known to start insulin if the patient is GADA positive (16). GADA were by far the most prevalent diabetes-associated autoantibodies, with only a small additional fraction of patients having other autoantibodies. Thus, the projected shortfall of ascertainment of adult-onset autoimmune diabetes using GADA alone would be small.
We show for the first time that in adult-onset diabetes, LADA is more frequent than adult-onset autoimmune type 1 diabetes, but the two together do not account for all cases of adult-onset autoimmune diabetes, as some patients progress to insulin therapy between diagnosis and 6 months postdiagnosis. Other studies, unlike this present analysis, failed to eliminate the potential error resulting from limited autoantibody specificity, which we did by testing for all autoantibodies twice to limit false positive results. A potential bias in our study is the use of hospital-based clinics in five of nine settings, since patients with autoimmune diabetes are more likely to be ascertained in such clinics given their greater risk of insulin treatment. Such a bias would increase the relative proportion of cases with autoantibodies and, specifically, the proportion with type 1 diabetes compared with LADA—a bias evident for the former but not the latter. That former bias would not influence the characteristics of autoantibody-positive versus autoantibody-negative patients but might further exaggerate the number of apparent cases of type 1 diabetes (16,17). The inclusion of patients up to 4 years postdiagnosis might have led to an underestimation of LADA cases because autoantibodies might become negative with time. Variation in ascertainment through hospital-based or primary care–based clinics around Europe precludes analysis of differential frequencies of autoimmune diabetes within Europe. Despite these potential biases, there was a striking excess of LADA compared with type 1 diabetes, implying that the typical presentation of adult-onset autoimmune diabetes is as non–insulin-requiring diabetes, with neither LADA nor type 1 diabetes, as defined, capturing all adult-onset autoimmune diabetes cases.
Patients with autoimmune diabetes in this large cohort, compared with the remaining autoantibody-negative diabetic patients, tended to more often be female, younger at diagnosis, leaner, and subsequently more likely to be on insulin treatment with metabolic changes including higher HDL cholesterol and lower triglycerides. These differences were noted irrespective of the number of autoantibodies or presence or absence of GADAs. Importantly, patients with autoantibodies other than GADA were also leaner and more likely to be on insulin treatment, consistent with them having a disease process similar to that of the GADA-positive patients. Among patients with autoimmune diabetes, those with type 1 diabetes, compared with the remainder, also tended to be female, younger at diagnosis, leaner, and by definition, on insulin treatment, with lower triglycerides. Moreover, there was a striking male excess in autoantibody-negative type 2 diabetes cases, which was less apparent here in adult-onset autoimmune type 1 diabetes cases (51.8% male) but still in line with the known male excess in that group (18). Apart from detection of diabetes-associated autoantibodies, there were no categorical features that could clinically distinguish adult-onset autoimmune diabetes from type 2 diabetes. We identified at least two modes within the GADA-positive patients—one mode with a cutoff of 70 WHO IU (low GADA titer) and another at 200 WHO IU (high GADA titer)—though it should be noted that it may not be possible to relate our cutoff values to other GADA assay levels. Patients with high-titer compared with low-titer GADAs were more likely to be female, younger at onset, leaner, and on insulin treatment, with lower HDL cholesterol and higher triglycerides; in these features, they resemble patients with type 1 diabetes. However, each form of autoimmune diabetes could be found across the range of GADA titers, though type 1 diabetic patients tended to have high titers and LADA patients tended to have low titers. Moreover, patients with low GADA titer, compared with those who were GADA negative, were also younger at diagnosis and leaner with higher HDL cholesterol, and a higher proportion was treated with insulin. Thus, there is a gradation of clinical and biochemical features in patients, in which GADA titer is a continuous variable, ranging from high through low titer to GADA negativity, without any clear distinction apart from the presence or absence of GADA. Other smaller studies have shown that high-titer GADA-positive patients had a tendency to greater genetic (HLA) disease associations compared with low–GADA titer patients and that these genetic associations for autoimmune diabetes are broadly similar even over a wide age range, as are components of the metabolic syndrome (5,19,20).
As a result, we recommend that type 1 diabetes and LADA be viewed as part of a broad clinical spectrum that more truly represents autoimmune diabetes. The most prevalent form of diabetes is adult-onset type 2 diabetes, which affects ~4–7% of the adult European population. Childhood-onset type 1 diabetes, on the other hand, affects only some 0.25% of European children and adolescents, though a lifetime disease-risk analysis suggested that up to 1% develop classic type 1 diabetes, with a proportion doing so after age 30 years (21). Since we now show that nearly 10% of adult-onset diabetic patients have autoimmune diabetes, it follows that adult-onset autoimmune diabetes is probably more prevalent than childhood-onset type 1 diabetes, while in adult-onset autoimmune diabetes, LADA is more prevalent than classic type 1 diabetes (OR 3.3). Clinically, knowledge that adult-onset diabetic patients have GADA should alert physicians to the increased likelihood of more rapid progression to insulin therapy; i.e., there is value in measuring GADA in all adult-onset diabetes cases because a significant proportion of them with GADA, unidentifiable by clinical phenotype, potentially have a different therapeutic trajectory than in classic type 2 diabetes. In summary, this present study now shows that the majority of adult-onset autoimmune diabetic patients are non–insulin requiring at diagnosis and can be identified through GADA screening. In the tendency to be adult onset, with variable destruction of the target organ, leading to a broad clinical spectrum, autoimmune diabetes can now be seen to resemble other autoimmune diseases.
Supplementary Material
Acknowledgments
This study was partially funded by the 5th Framework Programme of the European Union. D.M. was supported by a grant from Instituto Carlos III, Madrid, Spain (project no. FIS 061104). This study was also funded by DeveloGen. No other potential conflicts of interest relevant to this article were reported.
M.I.H. coordinated the study, analyzed samples, researched data, and contributed to the final manuscript. H.K. and N.S. provided samples and contributed to the final manuscript. H.B. analyzed samples and contributed to the final manuscript. S.A.P. researched data and contributed to the final manuscript. R.B., D.M., A.D.L., K.Y., H.B.-N., J.T., C.S., C.T., D.H., S.H., G.S., and W.A.S. provided samples and contributed to the final manuscript. R.W. and S.B. collated data from centers and contributed to the final manuscript. P.P. provided samples and contributed to the final manuscript. R.D.L. coordinated the study, researched data, and contributed to the final manuscript. R.D.L. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Parts of this study were presented in abstract form at the 72nd Scientific Sessions of the American Diabetes Association, Philadelphia, Pennsylvania, 8–12 June 2012.
APPENDIX
Members of the Action LADA group are as follows: R.D.L., M.I.H., H.B., and S.A.P., Blizard Institute; P.P., University Campus Bio-Medico; R.W. and S.B., Swansea University; H.B.-N. and K.Y., Odense University Hospital; S.H. and D.H., Royal Victoria Hospital; R.B., University “La Sapienza”; W.A.S. and H.K., University of Düsseldorf; N.S., German Diabetes Centre, University of Düsseldorf, and Clinic for Metabolic Diseases at University Hospital Düsseldorf (on leave of absence from the German Diabetes Centre and currently employed by Lilly Deutschland, Bad Homburg); J. Seissler, Ludwig-Maximilians-University; G.S., Rudolfstiftung Hospital; J.T. and C.S., National Institute for Health and Welfare; A.D.L. and E. Brugue, Universitat Autonoma de Barcelona; D.M., Hospital Universitari Arna de Vilanova; and C.T., Hospital Edouard Herriot.
Footnotes
This article contains Supplementary Data online at http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc12-0931/-/DC1.
A slide set summarizing this article is available online.
*A full list of the members of the Action LADA consortium can be found in the appendix.
References
- 1.Bluestone JA, Herold K, Eisenbarth G. Genetics, pathogenesis and clinical interventions in type 1 diabetes. Nature 2010;464:1293–1300 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Leslie RD, Williams R, Pozzilli P. Clinical review: type 1 diabetes and latent autoimmune diabetes in adults: one end of the rainbow. J Clin Endocrinol Metab 2006;91:1654–1659 [DOI] [PubMed] [Google Scholar]
- 3.Tuomi T, Carlsson A, Li H, et al. Clinical and genetic characteristics of type 2 diabetes with and without GAD antibodies. Diabetes 1999;48:150–157 [DOI] [PubMed] [Google Scholar]
- 4.Hosszúfalusi N, Vatay A, Rajczy K, et al. Similar genetic features and different islet cell autoantibody pattern of latent autoimmune diabetes in adults (LADA) compared with adult-onset type 1 diabetes with rapid progression. Diabetes Care 2003;26:452–457 [DOI] [PubMed] [Google Scholar]
- 5.Buzzetti R, Di Pietro S, Giaccari A, et al. Non Insulin Requiring Autoimmune Diabetes Study Group High titer of autoantibodies to GAD identifies a specific phenotype of adult-onset autoimmune diabetes. Diabetes Care 2007;30:932–938 [DOI] [PubMed] [Google Scholar]
- 6.Zinman B, Kahn SE, Haffner SM, O’Neill MC, Heise MA, Freed MI, ADOPT Study Group Phenotypic characteristics of GAD antibody-positive recently diagnosed patients with type 2 diabetes in North America and Europe. Diabetes 2004;53:3193–3200 [DOI] [PubMed] [Google Scholar]
- 7.Turner R, Stratton I, Horton V, et al. UK Prospective Diabetes Study Group UKPDS 25: autoantibodies to islet-cell cytoplasm and glutamic acid decarboxylase for prediction of insulin requirement in type 2 diabetes. Lancet 1997;350:1288–1293 [DOI] [PubMed] [Google Scholar]
- 8.Rosário PW, Reis JS, Amim R, et al. Comparison of clinical and laboratory characteristics between adult-onset type 1 diabetes and latent autoimmune diabetes in adults. Diabetes Care 2005;28:1803–1804 [DOI] [PubMed] [Google Scholar]
- 9.Leslie RD, Kolb H, Schloot NC, et al. Diabetes classification: grey zones, sound and smoke: Action LADA 1. Diabetes Metab Res Rev 2008;24:511–519 [DOI] [PubMed] [Google Scholar]
- 10.Palmer JP, Hampe CS, Chiu H, Goel A, Brooks-Worrell BM. Is latent autoimmune diabetes in adults distinct from type 1 diabetes or just type 1 diabetes at an older age? Diabetes 2005;54(Suppl. 2):S62–S67 [DOI] [PubMed] [Google Scholar]
- 11.Fourlanos S, Dotta F, Greenbaum CJ, et al. Latent autoimmune diabetes in adults (LADA) should be less latent. Diabetologia 2005;48:2206–2212 [DOI] [PubMed] [Google Scholar]
- 12.The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 1997;20:1183–1197 [DOI] [PubMed] [Google Scholar]
- 13.Hawa MI, Fava D, Medici F, et al. Antibodies to IA-2 and GAD65 in type 1 and type 2 diabetes: isotype restriction and polyclonality. Diabetes Care 2000;23:228–233 [DOI] [PubMed] [Google Scholar]
- 14.Wenzlau JM, Juhl K, Yu L, et al. The cation efflux transporter ZnT8 (Slc30A8) is a major autoantigen in human type 1 diabetes. Proc Natl Acad Sci USA 2007;104:17040–17045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bingley PJ, Bonifacio E, Mueller PW. Diabetes Antibody Standardization Program: first assay proficiency evaluation. Diabetes 2003;52:1128–1136 [DOI] [PubMed] [Google Scholar]
- 16.Brophy S, Yderstraede K, Mauricio D, et al. Action LADA Group Time to insulin initiation cannot be used in defining latent autoimmune diabetes in adults. Diabetes Care 2008;31:439–441 [DOI] [PubMed] [Google Scholar]
- 17.Davies H, Brophy S, Fielding A, et al. Latent autoimmune diabetes in adults (LADA) in South Wales: incidence and characterization. Diabet Med 2008;25:1354–1357 [DOI] [PubMed] [Google Scholar]
- 18.Gale EA, Gillespie KM. Diabetes and gender. Diabetologia 2001;44:3–15
- 19.Petrone A, Suraci C, Capizzi M, et al. NIRAD Study Group The protein tyrosine phosphatase nonreceptor 22 (PTPN22) is associated with high GAD antibody titer in latent autoimmune diabetes in adults: Non Insulin Requiring Autoimmune Diabetes (NIRAD) Study 3. Diabetes Care 2008;31:534–538 [DOI] [PubMed] [Google Scholar]
- 20.Hawa MI, Thivolet C, Mauricio D, et al. Action LADA Group Metabolic syndrome and autoimmune diabetes: action LADA 3. Diabetes Care 2009;32:160–164 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lorenzen T, Pociot F, Hougaard P, Nerup J. Long-term risk of IDDM in first-degree relatives of patients with IDDM. Diabetologia 1994;37:321–327 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.