

Abstract
This study assesses the trends and differentials in length of quality life in the U.S. population as measured by happy life expectancy in 1970, 1980, 1990, and 2000. The analysis combines age-specific prevalence rates of subjective well-being from a large nationally representative survey and life table estimates of mortality in decennial Census years. Employing the period prevalence-rate life table method—Sullivan method, the analysis finds evidence for improvement in quality of life in the U.S. Happy life expectancy largely increased in both absolute terms (number of years) and relative terms (proportion of life) over time at all adult ages examined. And increases in total life expectancy were mainly contributed by increases in expectancy in happy years rather than unhappy years. Happy life expectancy is longer than active life expectancy. And there has been greater compression of unhappiness than compression of morbidity. There are substantial differentials in happy life expectancy by sex and race because of differential prevalence rates of happiness. Women and whites had longer years of total and happy life expectancies at most ages and dates, while men and blacks had greater proportions of happy life expectancies across the three decades. Although race differentials generally decreased at older ages and with time, relative disadvantages of blacks persisted.
Keywords: Quality of life, Subjective well-being, Happiness, Happy life expectancy, Active life expectancy, Longevity
1. Introduction
There were substantial mortality declines and sustained increases in life expectancies at birth and old ages in the United States during the last 100 years. The low mortality of older adults combined with the largest birth cohorts entering old age in history, the baby boomers, imply a continuation of the dramatic increase of the size of the aging population in the 21st century (Robine et al., 2003). A question of increasing interest in the demography of aging is whether Americans are living higher quality as well as longer lives. Whereas previous studies assessed healthy life expectancies in terms of negative and domain-specific health outcomes such as disabilities and chronic diseases, few have estimated trends in positive and global measures of subjective well-being that are highly indicative of quality of life. We know little about whether Americans are living longer and happier and how men and women and blacks and whites differ in number of quality years.
This study aims to broaden the scope of healthy life expectancy research to include a key positive element of quality of life—subjective well-being, as measured by happiness. It seeks to develop a useful all-encompassing measure of perceived quality of life at the population level—happy life expectancy (HapLE) that is analogous and complimentary to active life expectancy (ALE). It is the first study to provide initial evidence of trends and sociodemographic differentials in HapLE in the U.S. population. It contributes to our knowledge about changes in quality of life as perceived by citizens in our nation as it faces ever-increasing challenges associated with increasing longevity. The study first constructs measures of HapLE by combining large nationally representative survey data on general happiness (the General Social Survey) and population life table estimates of mortality and employing the period prevalence-rate life table method—Sullivan method. It then examines temporal changes in HapLE in the U.S. from 1970 to 2000 and sex and race differences in changes of HapLE over time. It also discusses the implication of findings on compression of morbidity and unhappiness for overall population quality of life in the U.S.
2. Background
Concerns about life quality in old age have been a vital part of aging research in the social and behavioral sciences (George, 2006). Quality of life in the population can be assessed by the degree to which individuals thrive, as manifested in their health and perceived overall well-being. Since the introduction of the idea of a population health indicator combining mortality and disability by Sanders (1964) and the method of estimation by Sullivan (1971), a growing focus of research in the medical demography of aging has been on using healthy life expectancy measures to monitor changes in the length and proportion of healthy life that occurs with increases in total life expectancy. At present, healthy life expectancy in general has been synonymously referred to as and represented by active life expectancy (ALE), or the average number of years people are expected to live free from physical problems such as disabilities or chronic illness (Crimmins et al., 1989, 1997; Katz et al., 1983; Robine and Ritchie, 1991) and mental disorders such as dementia and depression (Robine et al., 2003) given the current age-specific rates of mortality and morbidity.
The advent of ALE measures largely enhanced our ability to test theories of consequences of the substantial decreases in mortality. Inconsistent with the failure of success hypothesis that predicts expansion of morbidity (Gruenberg, 1977; Kramer, 1980; Olshansky et al., 1991), accumulating evidence emerged for declining morbidity and disability in the old age that lends more support to compression of morbidity hypothesis (Fries, 1980; Nusselder, 1997). Findings on trends in ALE in the U.S. differ depending on the severity of disabilities examined, but both period estimates (Crimmins et al., 1997) and completed cohort estimates (Manton and Land, 2000) show that recent increases in life expectancy after 1980 were concentrated in increases in ALE. And the reduction in length of life with morbidity was unequally distributed among racial and educational groups, with African Americans and those of lower education status experiencing little compression of morbidity (Crimmins and Saito, 2001). Studies of mental health life expectancies were confined to European populations (Ritchie and Polge, 2003). The general trends corroborate with those of ALE.
At present, our understanding of quality of life (QoL) at the population level is largely confined to trends in ALE and can be extended both conceptually and empirically by taking into account global indicators of subjective well-being.
2.1. Quality of life and subjective well-being
Current research conceptualizes QoL as including both objective life conditions such as health status and subjective perceptions (The WHOQOL Group, 1998; Diener and Suh, 1997). This approach suggests clearly that objective status, although strongly related to QoL, is not synonymous with it. In previous research on ALE that focuses on specific domains of health problems such as functional disabilities and chronic illnesses, assessment of subjective well-being is conspicuously absent. It is incumbent for researchers to consider, however, the possibility that disability-free and physically and cognitively intact adults may rate the quality of their lives as poor, whereas disabled individuals have high levels of subjective quality of life. For example, a large number of older adults report high levels of QoL and subjective well-being despite physical disability (Pennex et al., 1998). Meanwhile, considerable proportions of active adults with no disabilities report low levels of QoL (Covinksy et al., 1999). In fact, research shows that objective life conditions explain only about half of the variance in subjective well-being in Americans of all ages (Diener, 1984).
Overall health, exemplified by bio-physiological functioning and mental health indicated by socio-psychological functioning, can be defined in two ways: one by “negative health”, or the absence of disease or impairment, and the other by “positive health”, or signs of good functioning (Veenhoven, 1996). Following the lead of the World Health Organization (1946), some European scholars study health as more than the absence of illness and incorporate positive states of overall well-being such as finding life pleasurable (Perenboom et al., 2003). The movement away from pathology and toward positive measures of health has also been witnessed in survey-based studies in social psychology (e.g., Diener, 1984; George, 1999) and economics (e.g., Easterlin, 2001) that found positive aspects of health, such as subjective appraisals of sense of well-being, especially happiness, also matter a great deal for overall quality of life. Positive health, although widely accepted at the conceptual level, has received almost no attention at the empirical level in social research on U.S. population.
2.2. Happy life expectancy
Happiness has been a most important indicator of QoL because, together with physical and mental health, it shows how people live and thrive. And it provides information especially pertinent to welfare policies in the broadest sense (Veenhoven, 1997). Happiness has been formally defined as a state of stable, global judgment of life quality and the degree to which a person evaluates the overall quality of his present life positively (Easterlin, 2001; Veenhoven, 1997). This conceptualization denotes an overall evaluation of life instead of a specific domain of life (e.g., work, marriage, physical condition). It also indicates a stable state of mind and positive appreciation of life. The terms life satisfaction and subjective well-being are variants of happiness and tend to be used interchangeably. Life satisfaction denotes essentially the same meaning as happiness and subjective well-being is a broader term used to encompass concepts like happiness and satisfaction (George, 1981). Empirical evidence shows that measures of these concepts are highly inter-correlated and share individual, social, and national-level determinants (George, 2006; Veenhoven, 1996).
Quality of life in a population can be assessed through a measure of happy life expectancy (HapLE thereafter) when combined with assessment of length of life. Analogous to the commonly used measures of healthy life expectancies, HapLE is a summary life table measure that disaggregates the total life expectancy (TLE) into happiness status specific life expectancies. Using the Sullivan method (Sullivan, 1971; Robine and Ritchie, 1991), HapLE at any specific age can be formally defined as the average number of years of happy life a member of the life table cohort would live given the current age-specific rates of mortality and happiness.
The study of HapLE can compliment studies of ALE and yield results that can shed light on the debate of different consequences of recent mortality change. Estimates of ALE in the U.S. suggest that, although expectations of life free of disability generally increased for men and women from 1970 to 1990, a substantial number of years were spent in morbid state. For instance, ALE at age 65 in 1990 was estimated to be 9.8 for women (total LE = 18.9) and 7.4 for men (total LE = 15.1), leaving about one half of remaining life disabled (Crimmins et al., 1997). A theoretically and empirically important question is: Do trends in HapLE parallel those in ALE? Because physical health is among the strongest predictors of happiness (Mroczek and Spiro, 2005), the trends and patterns of HapLE may closely mirror those of ALE. But empirical evidence of large mismatches between physical health status and perceived well-being implies that life expectancies in positive states of well-being may differ from those in ALE. Specifically, the observation that older adults are able to sustain high levels of happiness despite the onset of frailty and chronic disabilities (Baltes and Carstensen, 2003; Steverink et al., 2001) implies a longer HapLE than ALE. A related question is whether there has been a compression of unhappiness similar to the compression of morbidity or, on the contrary, an expansion of unhappy life—indicating declines in quality of life. Measures and estimations of HapLE, therefore, become essential to gauge the magnitude of the difference in HapLE and ALE and testing competing hypotheses.
To date, explicit empirical assessment of HapLE appears in only three studies (Kunst et al., 1994; Perenboom et al., 2004; Veenhoven, 1996). These studies focus on European countries with occasional incorporation of U.S. population, but there has been no sustained empirical investigation of HapLE in the U.S. population using sound data and analytic methods. The problematic operationalization of HapLE in two of the studies casts doubts on the accuracy and interpretation of their results.1 The other study by Perenboom and colleagues (2004) significantly improved the method of estimation using the Sullivan’s method. But because it used the Negative Affect Scale (NAS) to measure well-being, the study does not estimate length of happy life. This is especially important because of consistent evidence that the factors that predict negative affect are not the same factors that predict positive affect (e.g., George, 1981, 1992). The trend analysis by Perenboom et al. (2004) showed increases in well-being-life expectancy in the Netherlands between 1989 and 1998 for men and women at ages 16 and 65. Moreover, the increase at older ages exceeded the increase in TLE, indicating a compression of distress. These findings are from one European country over only 10 years. The question of whether the same trends and patterns of HapLE hold for the U.S. in the same and other time periods remains.
The overall temporal pattern of population HapLE as a whole may mask notable differences in patterns among demographic subgroups. Previous research on determinants of happiness suggests men and women and blacks and whites differ in levels of happiness. Studies based on age-heterogeneous samples generally show small sex differences and those based on samples of older adults show that older women report significantly lower levels of happiness than older men and this gender gap widens with age (Inglehard, 2002; Pinqart and Soerensen, 2001). Trend analysis shows changing sex differences over time, with women being happier than men in the 1970s and less happy than men in the 1990s (Easterlin, 2001). The racial gap in happiness is much larger than that for sex, with blacks less happy than their white counterparts throughout the life course (Easterlin, 2001). And this difference does not disappear when socioeconomic status is taken into account (Davis, 1984). Sex and race differences in prevalence rates of happiness as well as mortality rates, therefore, suggest different group-specific estimates of HapLE and time trends of HapLE. The identification of these major social and demographic differentials can contribute to efforts to make compression of unhappiness/expansion of happy life more characteristic of the total population.
In sum, limitations in previous studies call for broader conceptualizations, measures, and analyses of life quality in the U.S. adult population. The remainder of this paper seeks to fill this gap by constructing life table estimates of HapLE as quantitative summaries of population quality of life for the last 30 years in the U.S. It assesses temporal trends in sex- and race-specific HapLE and changes in both absolute and relative lengths of happy life.
3. Data and methods
3.1. Data
To calculate HapLE, two types of data will need to be combined: (1) responses to the happiness question from large scale national representative survey data for estimates of prevalence rates of happiness; and (2) population mortality rates and life tables from Census and vital statistics for estimates of total life expectancy.
Repeated cross-sectional surveys from the General Social Survey (GSS) (Davis and Smith, 2005) provide the best nationally-representative source of data on happiness in the U.S. The GSS also spans the longest time period in the U.S. and is part of the World Database on Happiness (Veenhoven, 1992). Each survey uses multistage stratified probability sampling and includes a nationally representative sample of non-institutionalized adults age 18 and older in the U.S. Subjective well-being is assessed in the GSS as a single-item report of happiness. 2 The data on happiness are available for most years from 1972 to 2004. In all years, the GSS question on overall happiness is: “Taken all together, how would you say things are these days—would you say that you are very happy, pretty happy, or not too happy?” The responses are coded as 1 (=very happy), 2 (=pretty happy), and 3 (=not too happy). The sample sizes range from about 1500 to 3000 across survey years.
Despite the simplicity of the happiness measure, there is considerable evidence of its psychometric adequacy in both U.S. and international research. The measure has adequate validity. Most people know quite well whether or not they enjoy life. Eight out of 10 Americans think of it every week (Veenhoven, 1996). Responses are generally not distorted by systematic bias associated with normative notions and desires, ego-defense, and social desirability (Diener, 1984; Veenhoven, 1996). Clinical studies that compared responses to single direct questions with ratings based on in-depth interviews and projective tests did not find much difference between the two (Heady and Wearing, 1992; Veenhoven, 1984). It is also important to note that self-reports of subjective well-being measure dimensions of social life feelings that discriminate well from psychiatric diagnoses such as depression and anxiety, as well as self-esteem (Hughes and Thomas, 1998). Findings from previous research also show that the measure has considerable reliability. The test–retest reliability has been reported to be between 0.6 and 0.7 (Veenhoven, 1996). There is strong evidence that similar referents (i.e., the areas of the life upon which judgments of happiness rest) are used both within nations and across them (Veenhoven, 1992). That is, the sources of happiness are quite stable because in most people’s lives, the dominant concerns are making a living, family life, and health (Easterlin, 2001). The co-occurrence of worries does not prove response distortion because individuals may see life as satisfying overall despite some difficult times (Veenhoven, 1996). In addition, random bias in responses tends to balance out and does not affect the accuracy of happiness averages in large samples (Saris et al., 1996).
The analysis estimates age-specific prevalence rates of happiness using sample proportions in each of the three states of happiness: very happy, pretty happy, and not too happy or unhappy. The first two states are qualitatively homogeneous categories and thus can also be combined into the state of being happy. Estimates of life table functions by sex and race are from the decennial life tables of the U.S. population provided by the National Vital Statistics Report from CDC/NCHS3 because population mortality data and estimates of life expectancies are of best quality in decennial Census years. Accordingly, the analysis focuses on rates of happiness in years 1970, 1980, 1990, and 2000. Pooling the survey data from the three survey years including and surrounding each decennial Census year increases the stability of estimates (e.g., Crimmins and Saito, 2001). The sample sizes range from 3411 to 5617 for these years.
3.2. Analytic method
The prevalence-rate based Sullivan life table method is employed to compute estimates of HapLE (Sullivan, 1971). The essence of the method is to partition the total person-years lived obtained from the period life table into the happy and unhappy life expectancy based on the age-specific prevalence rate or proportion happy estimated from the cross-sectional survey. Age-specific prevalence rate of being happy, very happy, and pretty happy can be denoted as nhx, nh1x, and nh2x, where x and x + n are ages at the beginning and end of the age interval (n = 5 in this study) and nhx = nh1x + nh2x. To calculate the expectation of happy life, for example, one first calculates the person-years of the life lived in the happy state for a given age interval x to x + n:
| (1) |
where nLx is the person-year life table function. Based on Eq. (1), happy life expectancy (HapLE) at age x can be calculated just as the standard total life expectancy:
| (2) |
where the is the total person-years lived in happiness from age x up to the end of the life table; lx value represents the number of persons alive at the beginning of the age interval x out of the original 100,000 births, the radix of the life table. Similarly, very happy and pretty happy life expectancies can be calculated using corresponding age-specific prevalence rates, nh1x and nh2x. Unhappy life expectancy (UHapLE) can be derived by modifying Eq. (1) using the unhappy prevalence ratio, nhux = (1 − nhx), or simply calculated as: .
As in previous applications, the Sullivan method employed in the present study is based on the assumption of stationarity of age-specific happiness prevalence. That is, the age-specific happiness prevalence is constant over time. Together with the period life table assumption of stationary population and mortality (Preston et al., 2001), this assumption is needed to infer the age-specific happiness prevalence of a hypothetical cohort from different cohorts in cross-sectional data. And the purpose is to use a period life table to calculate the life expectancy of a hypothetical cohort that experiences the current happiness and mortality rates. Substantive findings, therefore, will have to be interpreted as expectations of life of synthetic life table cohorts rather than those of true cohorts across the life course. It has been shown recently that Sullivan’s method has a sound statistical foundation and under the stationarity assumption, it yields unbiased and consistent estimator of state-specific life expectancy (Imai and Soneji, forthcoming).
The Sullivan method applies well to data from large surveys that produce highly reliable estimates for age-specific prevalence rates and is useful for monitoring relatively smooth long term trends in health expectancies (Laditka and Hayward, 2003; Mathers and Robine, 1997). These conditions are met in analyses of total population HapLE. For population subgroups stratified by age, sex, and race in a given year, the sample sizes are relatively small and become even smaller when all four variables are used to classify the population subgroups (i.e., smaller than 50). The age-group-specific prevalence rates observed from the GSS data exhibit erratic changes across ages and groups (especially for the oldest ages which have few respondents) due to sampling errors and other stochastic fluctuations. Therefore, following well-established demographic practice (e.g., Land et al., 1994), the analysis aggregated the single years of age into 5-year age groups and used regression models to obtain smoothed expected rates that are more stable and reliable. Specifically, observed age-specific rates of happiness were modeled using multivariate regressions with covariates of age, year, sex, and race. Model fit of various model specifications (using polynomial and interaction terms of covariates) was compared using the Bayesian Information Criterion statistics (BICs). Reported results are based on the best fitting model (see Appendix A for more details). The predicted age-specific prevalence rates of happiness from the final model are presented in Table 1 by sex and race for 1970, 1980, 1990, and 2000.4
Table 1.
Percent of population in two states of happiness by age, sex, and race: U.S. 1970–2000
| Age | Men
|
Women
|
||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1970 (N = 1611)
|
1980 (N = 1517)
|
1990 (N = 1471)
|
2000 (N = 2456)
|
1970 (N = 1800)
|
1980 (N = 2035)
|
1990 (N = 2000)
|
2000 (N = 3161)
|
|||||||||
| 5hx | 5hux | 5hx | 5hux | 5hx | 5hux | 5hx | 5hux | 5hx | 5hux | 5hx | 5hux | 5hx | 5hux | 5hx | 5hux | |
| 30–34 | 85.8 | 14.2 | 87.6 | 12.4 | 89.2 | 10.8 | 90.6 | 9.4 | 88.3 | 11.7 | 88.6 | 11.4 | 89.0 | 11.0 | 89.3 | 10.7 |
| 35–39 | 86.3 | 13.7 | 88.0 | 12.0 | 89.5 | 10.5 | 90.9 | 9.1 | 88.4 | 11.6 | 88.7 | 11.3 | 89.0 | 11.0 | 89.3 | 10.7 |
| 40–44 | 86.4 | 13.6 | 88.1 | 11.9 | 89.6 | 10.4 | 91.0 | 9.0 | 88.2 | 11.8 | 88.5 | 11.5 | 88.8 | 11.2 | 89.1 | 10.9 |
| 45–49 | 86.3 | 13.7 | 88.0 | 12.0 | 89.6 | 10.4 | 90.9 | 9.1 | 87.8 | 12.2 | 88.1 | 11.9 | 88.5 | 11.5 | 88.8 | 11.2 |
| 50–54 | 86.1 | 13.9 | 87.8 | 12.2 | 89.4 | 10.6 | 90.7 | 9.3 | 87.3 | 12.7 | 87.6 | 12.4 | 87.9 | 12.1 | 88.3 | 11.7 |
| 55–59 | 85.8 | 14.2 | 87.6 | 12.4 | 89.2 | 10.8 | 90.5 | 9.5 | 86.6 | 13.4 | 87.0 | 13.0 | 87.4 | 12.6 | 87.7 | 12.3 |
| 60–64 | 85.6 | 14.4 | 87.4 | 12.6 | 89.0 | 11.0 | 90.4 | 9.6 | 86.0 | 14.0 | 86.4 | 13.6 | 86.8 | 13.2 | 87.1 | 12.9 |
| 65–69 | 85.4 | 14.6 | 87.2 | 12.8 | 88.8 | 11.2 | 90.3 | 9.7 | 85.5 | 14.5 | 85.9 | 14.1 | 86.3 | 13.7 | 86.6 | 13.4 |
| 70–74 | 85.5 | 14.5 | 87.3 | 12.7 | 88.9 | 11.1 | 90.3 | 9.7 | 85.2 | 14.8 | 85.6 | 14.4 | 85.9 | 14.1 | 86.3 | 13.7 |
| 75–79 | 85.8 | 14.2 | 87.6 | 12.4 | 89.1 | 10.9 | 90.5 | 9.5 | 85.1 | 14.9 | 85.5 | 14.5 | 85.9 | 14.1 | 86.3 | 13.7 |
| 80–84 | 86.5 | 13.5 | 88.1 | 11.9 | 89.6 | 10.4 | 91.0 | 9.0 | 85.4 | 14.6 | 85.8 | 14.2 | 86.2 | 13.8 | 86.6 | 13.4 |
| 85+ | 87.5 | 12.5 | 89.1 | 10.9 | 90.5 | 9.5 | 91.7 | 8.3 | 86.2 | 13.8 | 86.5 | 13.5 | 86.9 | 13.1 | 87.2 | 12.8 |
| White
|
Black
|
|||||||||||||||
| 1970 (N = 2940)
|
1980 (N = 2966)
|
1990 (N = 2953)
|
2000 (N = 4549)
|
1970 (N = 460)
|
1980 (N = 552)
|
1990 (N = 402)
|
2000 (N = 795)
|
|||||||||
| 5hx | 5hux | 5hx | 5hux | 5hx | 5hux | 5hx | 5hux | 5hx | 5hux | 5hx | 5hux | 5hx | 5hux | 5hx | 5hux | |
|
|
||||||||||||||||
| 30–34 | 89.5 | 10.5 | 90.4 | 9.6 | 91.3 | 8.7 | 92.1 | 7.9 | 75.6 | 24.4 | 77.5 | 22.5 | 79.2 | 20.8 | 80.9 | 19.1 |
| 35–39 | 89.4 | 10.6 | 90.4 | 9.6 | 91.3 | 8.7 | 92.1 | 7.9 | 76.8 | 23.2 | 78.6 | 21.4 | 80.3 | 19.7 | 81.9 | 18.1 |
| 40–44 | 89.2 | 10.8 | 90.1 | 9.9 | 91.0 | 9.0 | 91.8 | 8.2 | 77.4 | 22.6 | 79.2 | 20.8 | 80.8 | 19.2 | 82.4 | 17.6 |
| 45–49 | 88.6 | 11.4 | 89.7 | 10.3 | 90.6 | 9.4 | 91.4 | 8.6 | 77.7 | 22.3 | 79.4 | 20.6 | 81.1 | 18.9 | 82.6 | 17.4 |
| 50–54 | 88.0 | 12.0 | 89.1 | 10.9 | 90.0 | 10.0 | 90.9 | 9.1 | 77.7 | 22.3 | 79.5 | 20.5 | 81.1 | 18.9 | 82.7 | 17.3 |
| 55–59 | 87.2 | 12.8 | 88.4 | 11.6 | 89.4 | 10.6 | 90.3 | 9.7 | 77.7 | 22.3 | 79.4 | 20.6 | 81.1 | 18.9 | 82.6 | 17.4 |
| 60–64 | 86.5 | 13.5 | 87.7 | 12.3 | 88.8 | 11.2 | 89.8 | 10.2 | 77.7 | 22.3 | 79.5 | 20.5 | 81.1 | 18.9 | 82.7 | 17.3 |
| 65–69 | 85.8 | 14.2 | 87.1 | 12.9 | 88.2 | 11.8 | 89.2 | 10.8 | 77.9 | 22.1 | 79.6 | 20.4 | 81.3 | 18.7 | 82.8 | 17.2 |
| 70–74 | 85.4 | 14.6 | 86.7 | 13.3 | 87.8 | 12.2 | 88.9 | 11.1 | 78.4 | 21.6 | 80.1 | 19.9 | 81.7 | 18.3 | 83.3 | 16.7 |
| 75–79 | 85.3 | 14.7 | 86.6 | 13.4 | 87.7 | 12.3 | 88.8 | 11.2 | 79.4 | 20.6 | 81.0 | 19.0 | 82.6 | 17.4 | 84.0 | 16.0 |
| 80–84 | 85.6 | 14.4 | 86.8 | 13.2 | 88.0 | 12.0 | 89.0 | 11.0 | 80.8 | 19.2 | 82.4 | 17.6 | 83.9 | 16.1 | 85.2 | 14.8 |
| 85+ | 86.4 | 13.6 | 87.6 | 12.4 | 88.7 | 11.3 | 89.7 | 10.3 | 82.8 | 17.2 | 84.3 | 15.7 | 85.6 | 14.4 | 86.8 | 13.2 |
Note. 5hx = 5h1x + 5h2x, where 5hx, 5h1x, and 5h2x are age-specific rates of being happy, very happy, and pretty happy; 5hux is age-specific unhappy rate.
Sources: See text and Appendix A.
Decennial life tables are publicly available in the form of single-year unabridged life tables by sex and race and were converted into 5-year abridged life tables to be consistent with the prevalence rates estimated from the GSS.5 While survey-based prevalence rates and life table parameters are estimated for all adult ages, the remainder of the analysis will focus on estimates for three age groups: 30, 65, and 85, to capture differences in important stages of adult life course and facilitate comparisons with ALE at these ages.
4. Results and findings
To examine trends and differences in happy life expectancy, we first need to understand trends and differences in rates of happiness as their inputs.
4.1. Happiness trends and differentials
Table 1 shows considerable age and temporal variations in estimated happiness prevalence rates for all subgroups over the last three decades. The patterns also differ among these subgroups. The proportion happy tended to increase with age among men and blacks whereas it tended to decrease with age among women and whites. There were increases in all groups in proportions very happy or pretty happy from 1970 to 2000, with men and blacks gaining more improvement than women and whites. Age-specific very happy and pretty happy rates show similar results and were not presented in the interest of space. Consistent with prior studies on correlates of happiness in the U.S. (e.g., Easterlin, 2001; Davis, 1984), the age, year, sex, and race differences in proportion happy are all statistically significant. In addition, there are also significant interaction effects between sex and age, sex and year, and race and age (see Appendix A).
Changes in group differentials with age and over time are further demonstrated in Figs. 1 and 2. Fig. 1 indicates the ratio of age-specific happiness rates for men to women over the 30-year period. Although men were at relatively disadvantages in happiness compared to women in early and middle adulthood in 1970 and 1980 (as indicated by the ratios below 1 for ages 30–65 in 1970 and ages 30–45 in 1980), they surpassed women at every age in 1990 and 2000 in proportion happy (i.e., the ratios are above 1). And the upward age trends in the ratios for all periods suggest increasing advantages of men relative to women with age. Fig. 2 compares the ratios of age-specific happiness rates for blacks to whites. It is evident that the racial gap in subjective well-being is larger than the sex gap and was persistent from 1970 to 2000. The black to white ratios were constantly above 1 for all ages and periods, with the highest ratio being close to 1.2. In contrast to the upward age trend in the sex differences, the black and white gap was the largest in early adulthood and steeply declined into old age. While period declines in sex differentials were largely constant for all ages, period declines in the racial gap decreased steadily with age and became very small at ages 75 and over. This suggests that blacks’ disadvantage in subjective well-being relative to whites declined with age and time, but their improvement in recent decades was much less pronounced in older ages.
Fig. 1.

Ratio of age-specific happy rates (5hx) for men to women: 1970–2000.
Fig. 2.

Ratio of age-specific happy rates (5hx) for White to Black: 1970–2000.
4.2. Happy life expectancy by sex
Table 2 presents estimates of total life expectancy (TLE), happy life expectancy (HapLE) and unhappy life expectancy (UHapLE) in years and proportions by sex for ages 30, 65, and 85 and years 1970, 1980, 1990, and 2000. Men and women differ in both lengths and proportions of happy and unhappy life. At all ages and dates, women’s expected years of total, happy, and unhappy life exceeded those of men. But the opposite is true when life expectancies are examined proportionally. With the exception of age 30 in 1970, proportions of life in happiness were greater for men than women. For both men and women, estimates of pretty happy life expectancies (PHapLE) are greater than those of very happy life expectancies (VHapLE) in both years and proportions. Estimates of VHapLE and PHapLE show similar age and sex patterns with those of HapLE. And longer years of VHapLE for women than men are restricted to younger ages.
Table 2.
Life expectancy in happiness by age and sex: U.S. 1970–2000
| Expectation of life | Men
|
Women
|
||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1970 | 1980 | 1990 | 2000 | 1970–2000 | 1970 | 1980 | 1990 | 2000 | 1970–2000 | |
| At age 30 years | ||||||||||
| Total (TLE) | 40.5 | 42.8 | 44.0 | 45.9 | 5.4 | 46.9 | 49.3 | 50.1 | 50.5 | 3.6 |
| Happy (HapLE) | 34.8 | 37.5 | 39.3 | 41.6 | 6.8 | 40.8 | 43.0 | 43.9 | 44.4 | 3.6 |
| Very happy (VHapLE) | 13.9 | 14.7 | 15.2 | 15.8 | 1.9 | 17.3 | 17.3 | 16.7 | 16.0 | −1.3 |
| Pretty happy (PHapLE) | 20.9 | 22.8 | 24.2 | 25.8 | 4.9 | 23.5 | 25.7 | 27.2 | 28.4 | 4.9 |
| Unhappy (UHapLE) | 5.7 | 5.2 | 4.7 | 4.3 | −1.4 | 6.1 | 6.3 | 6.2 | 6.1 | 0.0 |
| % of life expectancy | ||||||||||
| Total | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | ||
| Happy | 86.0 | 87.8 | 89.3 | 90.7 | 4.7 | 86.9 | 87.2 | 87.6 | 87.9 | 1.0 |
| Very happy | 34.4 | 34.5 | 34.4 | 34.4 | 0.0 | 36.9 | 35.1 | 33.3 | 31.6 | −5.3 |
| Pretty happy | 51.6 | 53.3 | 54.9 | 56.3 | 4.7 | 50.1 | 52.2 | 54.3 | 56.3 | 6.2 |
| Unhappy | 14.0 | 12.2 | 10.7 | 9.3 | −4.7 | 13.1 | 12.8 | 12.4 | 12.1 | −1.0 |
| At age 65 years | ||||||||||
| Total (TLE) | 13.0 | 14.2 | 15.1 | 16.2 | 3.2 | 16.8 | 18.4 | 19.0 | 19.1 | 2.3 |
| Happy (HapLE) | 11.2 | 12.4 | 13.5 | 14.7 | 3.5 | 14.3 | 15.8 | 16.3 | 16.5 | 2.2 |
| Very happy (VHapLE) | 5.1 | 5.6 | 5.9 | 6.3 | 1.2 | 6.1 | 6.4 | 6.2 | 5.9 | −0.2 |
| Pretty happy (PHapLE) | 6.0 | 6.9 | 7.6 | 8.4 | 2.3 | 8.2 | 9.4 | 10.1 | 10.6 | 2.4 |
| Unhappy (UHapLE) | 1.8 | 1.8 | 1.6 | 1.5 | −0.3 | 2.4 | 2.6 | 2.6 | 2.6 | 0.1 |
| % of life expectancy | ||||||||||
| Total | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | ||
| Happy | 85.8 | 87.6 | 89.2 | 90.6 | 4.8 | 85.4 | 85.8 | 86.2 | 86.6 | 1.2 |
| Very happy | 39.4 | 39.3 | 39.1 | 39.0 | −0.4 | 36.4 | 34.5 | 32.8 | 31.1 | −5.3 |
| Pretty happy | 46.4 | 48.3 | 50.1 | 51.6 | 5.2 | 49.0 | 51.3 | 53.4 | 55.5 | 6.5 |
| Unhappy | 14.2 | 12.4 | 10.8 | 9.4 | −4.8 | 14.6 | 14.2 | 13.8 | 13.4 | −1.2 |
| At age 85 years | ||||||||||
| Total (TLE) | 4.7 | 5.1 | 5.3 | 5.6 | 0.9 | 5.6 | 6.4 | 6.7 | 6.7 | 1.0 |
| Happy (HapLE) | 4.1 | 4.6 | 4.8 | 5.2 | 1.0 | 4.9 | 5.5 | 5.8 | 5.8 | 1.0 |
| Very happy (VHapLE) | 1.9 | 2.1 | 2.1 | 2.3 | 0.3 | 1.9 | 2.1 | 2.1 | 2.0 | 0.0 |
| Pretty happy (PHapLE) | 2.2 | 2.5 | 2.7 | 2.9 | 0.7 | 2.9 | 3.4 | 3.7 | 3.8 | 0.9 |
| Unhappy (UHapLE) | 0.6 | 0.6 | 0.5 | 0.5 | −0.1 | 0.8 | 0.9 | 0.9 | 0.8 | 0.1 |
| % of life expectancy | ||||||||||
| Total | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | ||
| Happy | 87.5 | 89.1 | 90.5 | 91.7 | 4.2 | 86.2 | 86.5 | 86.9 | 87.2 | 1.1 |
| Very happy | 40.8 | 40.6 | 40.4 | 40.2 | −0.6 | 34.6 | 32.8 | 31.2 | 29.5 | −5.1 |
| Pretty happy | 46.7 | 48.5 | 50.1 | 51.5 | 4.8 | 51.6 | 53.7 | 55.7 | 57.7 | 6.1 |
| Unhappy | 12.5 | 10.9 | 9.5 | 8.3 | −4.2 | 13.8 | 13.5 | 13.1 | 12.8 | −1.1 |
Time trends show pronounced increases in TLE for both men and women during the 30 years due to improvement in survival conditions and reductions in adult mortality. Expected years of happy life also increased continuously over the three decades for both men and women. At age 30, men were expected to live 34.8 years of happy life in 1970 and 41.6 years of happy life in 2000. The corresponding increase for women was from 40.8 to 44.4 years. And these increases were mainly contributed by increases in PHapLE. Meanwhile, there were decreases in expected years of unhappy life for men and no apparent change for women. There were also changes in proportions of happy and unhappy life. As indicated by their larger declines in percentages of unhappy life, men experienced a greater compression of unhappiness than women at age 30.
At ages 65 and 80 similar generalizations can be made about time trends. In contrast to the trends of ALE between 1970 and 1990 suggesting about 40–50% of total life at older ages spent in disability (Crimmins et al., 1997), the majority of adult life at all ages is spent in the happy state. Table 2 indicates that for men at all three ages, increases in expected years of happy life from 1970 to 2000 exceeded those in total life. For women, increases in TLE were concentrated in happy years. For both sexes, increases in years of HapLE were predominantly driven by increases in years of PHapLE rather than VHapLE. In fact, women showed declines in years of VHapLE at ages 30 and 65 and declines in proportions of VHapLE at all ages. Consistent decreases in both years and proportions of unhappy life for men of all ages across the three decades suggest compression of unhappiness with increasing longevity. Similar albeit smaller decreases in proportions of unhappy life for women also suggest a slight compression of unhappiness at all ages.6
4.3. Happy life expectancy by race
Table 3 shows estimated life expectancies by happiness state in years and proportions by race between 1970 and 2000. At age 30, despite their shorter TLE, blacks had much longer expected unhappy life than whites in both absolute and relative terms. In 1970, blacks at age 30 were expected to live 8.7 years or 22.4% of their total life in unhappiness, as opposed to their white counterparts whose UHapLE was only 5.4 years or 12.3% of the total life. At ages 65 and 85, the black and white differences in total, happy, and unhappy life expectancies decreased and even reversed in absolute but not in relative terms. Consistent with the trends shown above in race differentials in prevalence rates of happiness, whites’ advantages relative to blacks in expected years of happy life largely decreased from age 30 to age 65. And blacks and whites had roughly the same numbers of expected years of unhappy life at age 65. The TLE for blacks was higher than for whites at age 85 in all years. This reflects the well-known African-American/Caucasian “mortality crossover” among the oldest old (Nam, 1995) possibly due to selective survival and/or poor quality of mortality data at older ages, especially for blacks (Land et al., 1994; Preston et al., 1996). At this age, blacks had slightly more expected years of happy and unhappy life than whites except for 2000. At all ages and dates, however, blacks lived larger proportions of their life unhappy than whites.
Table 3.
Life expectancy in happiness by age and race: U.S. 1970–2000
| Expectation of life | White
|
Black
|
||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1970 | 1980 | 1990 | 2000 | 1970–2000 | 1970 | 1980 | 1990 | 2000 | 1970–2000 | |
| At age 30 years | ||||||||||
| Total (TLE) | 44.2 | 46.5 | 47.7 | 48.7 | 4.4 | 38.7 | 41.6 | 42.2 | 44.1 | 5.4 |
| Happy (HapLE) | 38.8 | 41.3 | 42.8 | 44.1 | 5.3 | 30.0 | 33.1 | 34.2 | 36.4 | 6.4 |
| Very happy (VHapLE) | 16.8 | 17.1 | 16.9 | 16.6 | −0.1 | 8.4 | 9.6 | 10.3 | 11.4 | 3.0 |
| Pretty happy (PHapLE) | 22.0 | 24.2 | 25.9 | 27.4 | 5.4 | 21.6 | 23.5 | 23.9 | 25.0 | 3.4 |
| Unhappy (UHapLE) | 5.4 | 5.3 | 4.9 | 4.6 | −0.9 | 8.7 | 8.6 | 8.0 | 7.6 | −1.0 |
| % of life expectancy | ||||||||||
| Total | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | ||
| Happy | 87.7 | 88.7 | 89.7 | 90.6 | 2.9 | 77.6 | 79.5 | 81.1 | 82.7 | 5.1 |
| Very happy | 38.0 | 36.7 | 35.5 | 34.2 | −3.8 | 21.7 | 23.1 | 24.4 | 25.8 | 4.1 |
| Pretty happy | 49.7 | 52.0 | 54.2 | 56.2 | 6.5 | 55.9 | 56.4 | 56.7 | 56.9 | 1.0 |
| Unhappy | 12.3 | 11.3 | 10.3 | 9.4 | −2.9 | 22.4 | 20.5 | 18.9 | 17.3 | −5.1 |
| At age 65 years | ||||||||||
| Total (TLE) | 15.0 | 16.6 | 17.4 | 17.9 | 2.8 | 14.2 | 15.4 | 15.6 | 16.1 | 2.0 |
| Happy (HapLE) | 12.9 | 14.4 | 15.3 | 15.9 | 3.0 | 11.2 | 12.4 | 12.8 | 13.6 | 2.3 |
| Very happy (VHapLE) | 5.9 | 6.2 | 6.3 | 6.3 | 0.4 | 3.5 | 4.0 | 4.3 | 4.7 | 1.2 |
| Pretty happy (PHapLE) | 7.0 | 8.1 | 9.0 | 9.7 | 2.6 | 7.7 | 8.4 | 8.6 | 8.9 | 1.2 |
| Unhappy (UHapLE) | 2.2 | 2.2 | 2.1 | 1.9 | −0.2 | 2.9 | 2.9 | 2.7 | 2.6 | −0.4 |
| % of life expectancy | ||||||||||
| Total | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | ||
| Happy | 85.6 | 86.9 | 88.1 | 89.1 | 3.5 | 79.3 | 81.0 | 82.6 | 84.0 | 4.8 |
| Very happy | 39.0 | 37.7 | 36.4 | 35.1 | −3.9 | 24.6 | 26.0 | 27.4 | 28.8 | 4.2 |
| Pretty happy | 46.6 | 49.2 | 51.7 | 54.0 | 7.4 | 54.7 | 55.0 | 55.2 | 55.2 | 0.5 |
| Unhappy | 14.4 | 13.1 | 11.9 | 10.9 | −3.5 | 20.7 | 19.0 | 17.4 | 16.0 | −4.8 |
| At age 85 years | ||||||||||
| Total (TLE) | 5.2 | 5.9 | 6.2 | 6.2 | 1.1 | 6.5 | 6.5 | 6.5 | 6.3 | −0.2 |
| Happy (HapLE) | 4.5 | 5.2 | 5.5 | 5.6 | 1.1 | 5.4 | 5.5 | 5.6 | 5.4 | 0.0 |
| Very happy (VHapLE) | 2.0 | 2.2 | 2.2 | 2.2 | 0.2 | 1.7 | 1.8 | 1.9 | 1.9 | 0.2 |
| Pretty happy (PHapLE) | 2.5 | 3.0 | 3.3 | 3.4 | 1.0 | 3.7 | 3.7 | 3.7 | 3.6 | −0.2 |
| Unhappy (UHapLE) | 0.7 | 0.7 | 0.7 | 0.6 | −0.1 | 1.1 | 1.0 | 0.9 | 0.8 | −0.3 |
| % of life expectancy | ||||||||||
| Total | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | ||
| Happy | 86.4 | 87.6 | 88.7 | 89.7 | 3.3 | 82.8 | 84.3 | 85.6 | 86.8 | 4.0 |
| Very happy | 38.8 | 37.5 | 36.2 | 34.9 | −3.9 | 25.7 | 27.1 | 28.5 | 30.0 | 4.3 |
| Pretty happy | 47.6 | 50.1 | 52.5 | 54.7 | 7.1 | 57.1 | 57.2 | 57.1 | 56.8 | −0.3 |
| Unhappy | 13.6 | 12.4 | 11.3 | 10.3 | −3.3 | 17.2 | 15.7 | 14.4 | 13.2 | −4.0 |
Time trends show that there were evident continuous increases in years of HapLE and decreases in UHapLE for both groups, but the racial gap remained substantial. In 2000, the UHapLE at age 30 for blacks decreased to 7.6 years and 17.3% of the total life. The corresponding figures for whites are 4.6 years and 9.4%. Increases in TLE at all ages during the last 30 years were mainly contributed by increases in HapLE for both whites and blacks. A notable racial difference in change in HapLE is that improvement in blacks was contributed much more by increases in VHapLE than whites. There were declines in both years and proportions of unhappy life for both groups, indicating compression of unhappiness.
4.4. Happy life expectancy by sex and race
The examination of lengths and proportions of happy life for sex–race-specific subgroups further indicates differential trends and patterns of compression of unhappiness, as shown in Table 4. At age 30 in 2000 white women had the longest TLE of 50.9 years and the longest HapLE of 45.6 years. While both black women and white men had about 46 years of expected life, UHapLE was 4 years longer for black women. Black men faired much worse than their white counterparts with regard to lengths of total and happy life expectancies. While they were expected to live fewer years in total than their female counterparts, they had shorter UHapLE.
Table 4.
Expectation of life in happiness in years by age, sex, and race: U.S. 1970–2000
| Expectation of life | White Men
|
White Women
|
||||||
|---|---|---|---|---|---|---|---|---|
| 1970 | 1980 | 1990 | 2000 | 1970 | 1980 | 1990 | 2000 | |
| At age 30 | ||||||||
| Total (TLE) | 41.0 | 43.3 | 44.6 | 46.3 | 47.5 | 49.7 | 50.6 | 50.9 |
| Happy (HapLE) | 35.8 | 38.5 | 40.4 | 42.5 | 41.8 | 44.0 | 45.0 | 45.6 |
| Very happy (VHapLE) | 14.8 | 15.5 | 15.9 | 16.3 | 18.6 | 18.5 | 17.9 | 17.0 |
| Pretty happy (PHapLE) | 21.0 | 23.0 | 24.5 | 26.2 | 23.2 | 25.5 | 27.2 | 28.6 |
| Unhappy (UHapLE) | 5.2 | 4.8 | 4.3 | 3.8 | 5.7 | 5.7 | 5.5 | 5.3 |
| At age 65 | ||||||||
| Total (TLE) | 13.0 | 14.2 | 15.2 | 16.3 | 16.9 | 18.5 | 19.1 | 19.2 |
| Happy (HapLE) | 11.2 | 12.6 | 13.7 | 14.9 | 14.4 | 16.0 | 16.6 | 16.8 |
| Very happy (VHapLE) | 5.3 | 5.7 | 6.1 | 6.4 | 6.4 | 6.7 | 6.5 | 6.2 |
| Pretty happy (PHapLE) | 5.9 | 6.8 | 7.6 | 8.4 | 8.0 | 9.3 | 10.1 | 10.6 |
| Unhappy (UHapLE) | 1.8 | 1.7 | 1.6 | 1.4 | 2.4 | 2.5 | 2.5 | 2.4 |
| At age 85 | ||||||||
| Total (TLE) | 4.6 | 5.1 | 5.3 | 5.5 | 12.6 | 13.3 | 13.3 | 14.5 |
| Happy (HapLE) | 4.1 | 4.6 | 4.8 | 5.1 | 5.8 | 5.9 | 5.9 | 5.5 |
| Very happy (VHapLE) | 1.9 | 2.1 | 2.2 | 2.2 | 3.6 | 4.2 | 4.5 | 5.3 |
| Pretty happy (PHapLE) | 2.1 | 2.4 | 2.6 | 2.9 | 6.4 | 6.8 | 6.8 | 7.3 |
| Unhappy (UHapLE) | 0.6 | 0.5 | 0.5 | 0.4 | 2.5 | 2.3 | 2.0 | 1.9 |
| Black Men
|
Black Women
|
|||||||
| 1970 | 1980 | 1990 | 2000 | 1970 | 1980 | 1990 | 2000 | |
|
|
||||||||
| At age 30 | ||||||||
| Total (TLE) | 35.4 | 37.8 | 38.1 | 41.0 | 42.0 | 45.4 | 46.0 | 46.7 |
| Happy (HapLE) | 27.0 | 30.0 | 31.2 | 34.6 | 33.0 | 36.2 | 37.1 | 38.1 |
| Very happy (VHapLE) | 8.0 | 9.4 | 10.3 | 12.2 | 8.7 | 9.9 | 10.5 | 11.1 |
| Pretty happy (PHapLE) | 19.1 | 20.6 | 20.9 | 22.4 | 24.3 | 26.3 | 26.6 | 27.0 |
| Unhappy (UHapLE) | 8.3 | 7.8 | 6.9 | 6.4 | 8.9 | 9.2 | 8.9 | 8.6 |
| At age 65 | ||||||||
| Total (TLE) | 12.6 | 13.3 | 13.3 | 14.5 | 15.7 | 17.1 | 17.3 | 17.4 |
| Happy (HapLE) | 10.1 | 11.0 | 11.3 | 12.6 | 12.5 | 13.8 | 14.1 | 14.3 |
| Very happy (VHapLE) | 3.6 | 4.2 | 4.5 | 5.3 | 3.5 | 3.9 | 4.2 | 4.3 |
| Pretty happy (PHapLE) | 6.4 | 6.8 | 6.8 | 7.3 | 9.0 | 9.8 | 10.0 | 10.0 |
| Unhappy (UHapLE) | 2.5 | 2.3 | 2.0 | 1.9 | 3.2 | 3.3 | 3.2 | 3.1 |
| At age 85 | ||||||||
| Total (TLE) | 5.9 | 5.6 | 5.6 | 5.7 | 7.0 | 7.1 | 7.0 | 6.5 |
| Happy (HapLE) | 5.0 | 4.9 | 4.9 | 5.2 | 5.8 | 5.9 | 5.9 | 5.5 |
| Very happy (VHapLE) | 1.9 | 1.9 | 2.1 | 2.3 | 1.5 | 1.6 | 1.7 | 1.6 |
| Pretty happy (PHapLE) | 3.2 | 3.0 | 2.9 | 2.9 | 4.3 | 4.3 | 4.2 | 3.9 |
| Unhappy (UHapLE) | 0.9 | 0.7 | 0.6 | 0.6 | 1.2 | 1.1 | 1.1 | 1.0 |
Over the course of the last 30 years, all groups at age 30 experienced substantial increases in expected years of happy life and some decreases in expected years of unhappy life. Fig. 3 suggests that black men had the largest increase in HapLE (7.6 years), followed by white men (6.7 years) and black women (5 years). Black men also led in the amount of increase in VHapLE. White women, on the other hand, show a decrease in VHapLE. UHapLE decreased for all and decreased the most among black and white men. The net changes in years of TLE for all are positive and are largely associated with improvement in perceived quality of life rather than prolonged unhappy life.
Fig. 3.
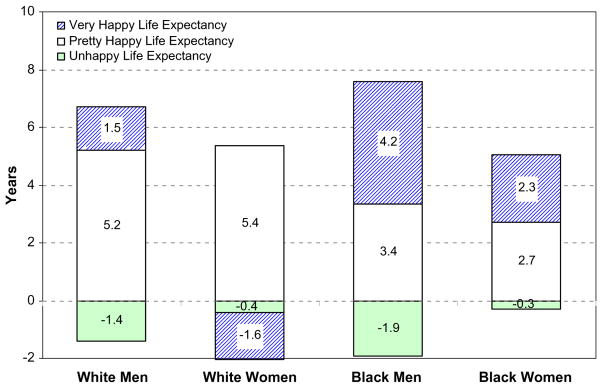
Change in life expectancy in years from 1970 to 2000 at age 30 by sex and race.
At age 65, white women continued to lead in lengths of total and happy life expectancies, and patterns for the other groups are similar to those at age 30. At age 85, sex and race differences in lengths of total, happy, and unhappy life expectancies largely decreased, with black women having the longest TLE and HapLE before 2000. Similar to the trends at age 30, increases in TLE were driven by increases in years of HapLE at ages 65 and 85. But changes in lengths of HapLE over time show different trends of group differentials at older ages. The large increments in expectation of years of happy life for blacks seemed to be restricted to early adulthood. At age 65, black men showed less increment compared to white men and even less at age 85. Black women experienced the least increment in expected years of happy life at age 65 and even a decrease at age 85.
Estimated proportions of expected happy and unhappy life at age 30 across the period of 1970–2000 are shown in Fig. 4. Estimates of proportion of life in happiness were greatest for white men and least for black women. And estimated proportions of very happy life increased over time for all but white women. All groups exhibited some degree of decreases in proportions of unhappy life over time. White men and black men, however, experienced greater degrees of compression of unhappiness than their female counterparts. Consistent with previous findings from Fig. 3, the improvement is especially notable for black men. And sex and race differences in relative lengths of happy and unhappy life hold at older ages.
Fig. 4.

Percent in expected life in happiness by sex and race at age 30: U.S. 1970–2000.
5. Discussion and conclusions
This study assessed the length of quality life in the U.S. population in terms of positive global indicators of well-being. The analysis combined age-specific prevalence rates of subjective well-being from a large nationally representative survey and life table estimates of mortality rates and life expectancies in four decennial Census years. The results of the analysis using the Sullivan method suggest interesting trends and differentials in happy life expectancies between 1970 and 2000. The study concludes that there has been an improvement in quality of life in the U.S. Happy life expectancy largely increased in both absolute terms (number of years) and relative terms (the proportion of life) at all adult ages examined. The differentials in happy life expectancy are also evident in men and women and whites and blacks. Race differentials were larger than sex differentials. Although these differentials generally decreased at older ages and with time, relative disadvantages of black men and women persisted.
The analysis finds evidence for the U.S. adult population that the majority of life is expected to be concentrated in years in very happy or pretty happy states from 1970 to 2000 for all ages. This corroborates findings from previous studies of European countries (Kunst et al., 1994; Perenboom et al., 2004; Veenhoven, 1996) and stands in contrast to a principal finding of studies of active life expectancy during the same time period (1970–1990)—that only about half of life at these ages are expected to be disability-free (Crimmins et al., 1997; Crimmins and Saito, 2001). Therefore, conclusions about general trends in well-being-life expectancy differ depending on conceptualization and measurement of quality of life used. The longer years and larger proportions of happy life than disability-free life suggests that a thorough understanding of the full range of manifestations of quality of life requires a comprehensive assessment of both domain-specific negative health outcomes and all-encompassing positive outcomes. The finding that happy life expectancy is longer than disability-free life expectancy has important social and demographic implications. It suggests that individuals with chronic illness and disability can sustain a descent sense of well-being through various means such as assistant living, technologically advanced devices and equipments, and instrumental support from social network.
Time trends of changes in happy life expectancy do not run parallel to those in disability-free life expectancy. The increases in total life expectancy were contributed by an increase in life expectancy with disability from 1970 to 1980 but an increase in disability-free life expectancy from 1980 to 1990 (Crimmins et al., 1997). Other studies of European populations show stagnating or even decreasing trends in disability- free life expectancy (Perenboom et al., 2004). This study provides evidence consistent with trends in the Netherlands that increases in happy life expectancy in the U.S. were continuous from 1970 to 2000 and exceeded the increases in total life expectancy for most ages and subgroups. Furthermore, there were increases in life expectancy in two different levels of happiness: very happy and pretty happy. And most increases in expectations of happy life are due to increases in expectations of pretty happy life. In contrast to little increase in the proportion of life without disability in the U.S., the steady increase in the proportion of happy life during this period indicates a greater extent of compression of unhappiness than compression of morbidity. Therefore, evidence of compression of unhappiness further challenges the failure of success hypothesis and supports an optimistic view of prospects of mortality declines. Lengthening life at older ages does not necessarily result in prolonged life with declined quality. Over the period of last 30 years, some aspects of life quality, such as perceived overall well-being, have increased to the effect that their influence may compensate for, or balance, a lack of increase in life without disabilities or activity limitations.
Changes in trends and patterns of happy life expectancy are primarily due to changes in prevalence rates of happiness. The increases in prevalence rates of happiness over time contributed to the increases in happy life expectancy. The validity and reliability of the measure of happiness rates undoubtedly affect this result and need to be corroborated by future studies using other data. But the present finding is in keeping with previous reports that suggest increasing happiness in European and American populations that can be related to changes in macroeconomic variables such as higher gross domestic product and lower unemployment rates from 1970s to 1990s (di Tella et al., 2003; Hagerty and Veenhoven, 2003).
Sex and race differentials in age-specific prevalence rates of happiness also shaped these differentials in happy life expectancy. Similar to the sex-specific patterns of active life expectancy, men gained more increases in happy life expectancy in both years and proportions than women and experienced more compression of poor quality life. The much smaller improvement in happy life expectancy for women relative to men results from the apparent lack of decline in the proportion of unhappy women. Those aged 30 in 1980–2000 are cohorts born in 1950–1970 who experienced the unanticipated increases in rates of female labor force participation and marital dissolution (Spain and Bianchi, 1996). So their lower levels of happiness and small increment in happy life expectancy could reflect increasing social stress associated with balancing work and family and/or economic deprivation of female-headed households. And the disappearance of female advantage during old age may be because women suffer more from the adverse effects of widowhood, whereas men benefit more from the positive effect of retirement (Easterlin, 2003). The substantial black and white gap in happy life expectancy confirms earlier findings on the continuing racial disparity in quality of life in the U.S. from 1970s to 1990s (Easterlin, 2001; Hughes and Thomas, 1998). It is noteworthy that racial inequality in happy life expectancy decreased somewhat in recent years. In addition, there were greater increases in very happy life expectancy for blacks compared to whites. These could be associated with Affirmative Action that narrowed the racial gap in education and income and consequently in quality of life. The convergence in black and white happy life expectancies at old ages could result from the differential survival of healthier and happier blacks.
Although the present study focuses on positive indicators of general subjective well-being, it provides an analytic framework and findings that can be extended and compared to studies of other indicators of well-being. It has been suggested that happiness or perception of life quality as a whole can be correlated with and act as a precursor of mental disorders such as depressive symptomatology (George, 2006). A prior study along this line that was conducted in the Dutch population estimated depression-free life expectancy to constitute only about 20% of total life expectancy at age 55 (Deeg et al., 1994). A recent finding in the U.S. from a short-term longitudinal survey suggests that more recent cohorts exhibit increasing levels of depressive symptoms (Yang, 2007). This trend can potentially translate to similarly low depression-free life expectancy. The lack of survey data on depression that span a long enough historical time presents a challenge for direct comparisons of happy vs. depression-free life expectancy. Nonetheless, it is important for future research to conduct such an analysis to better understand the relation between burden of mental illness and sense of well-being when better data become available.
In all, this study provides evidence that contributes to extant research on aging and quality of life in the U.S. in several respects. First, the study compliments studies of ALE and suggests that Americans are living longer and higher quality lives not only as indicated by physical fitness but also as indicated by subjective well-being. Second, the study finds substantial social disparities in the extent of compression of unhappy life and suggests the necessity for future research to further examine other aspects of social inequality such as socioeconomic and marital status differences that may result in inequality in population quality of life. Third, because happiness measures are useful for determining the extent to which societies meet the needs of their members and the degree to which citizens thrive, the U.S. HapLE estimates can aid cross-country comparisons of national quality of life and provide clues to betterment of people’s life through social policy.
Acknowledgments
This research is supported by National Institute on Aging Grant No. 1R03AG030000-01 and pilot project Grant No. R24 HD051152 from the Population Research Center, and Grant No. 5 P30 AG012857-12 from the Center on Aging at NORC, The University of Chicago. I thank Maria Medvedva for research assistance.
Appendix A. Model estimation of prevalence rates of happiness
Observed age-specific rates of happiness were modeled using logit regression models for group data (STATA command: blogit). Specifically, the model takes the following form:
where θij is the probability of being unhappy or happy for 5-year age group i in year j, for i = 1, …, 15 and j = 1, …, 4; A, Y, S, and R stand for age, year, sex (female = 1), and race (black = 1), respectively. Age and year effects were treated as dummy variables/indicators in alternative model specifications. The present model proved to be more parsimonious and yielded better model fit. Interaction effects were also tested among remaining variables and omitted in the interest of space.
BIC tests were conducted to search for preferred models. The coefficient estimates from the chosen model of unhappy rates are shown below as an example. All main and interaction effects included are statistically significant. This model was fitted to the data and yielded the predicted age-specific rates by sex and race shown in Table A.1. Predicted age-specific rates of being very happy and pretty happy were obtained using the same procedure.
Table A.1.
Model estimates of being unhappy
| Variable | Coefficient | SE | p-value |
|---|---|---|---|
| Age | .045 | .016 | 0.004 |
| Age2 | .002 | .002 | 0.376 |
| Age3 | −.001 | .000 | 0.004 |
| Year | −.164 | .029 | 0.000 |
| Sex (female = 1) | −.212 | .108 | 0.049 |
| Race (black = 1) | .739 | .059 | 0.000 |
| Age * Sex | .039 | .013 | 0.002 |
| Year * Sex | .106 | .038 | 0.006 |
| Age * Race | −.070 | .015 | 0.000 |
| Constant | −1.767 | .083 | 0.000 |
| −2log-likelihood | 14,287.3 | ||
| BIC | 14,336.6 |
Footnotes
The calculation of HapLE is seriously flawed in these two studies (Kunst et al., 1994; Veenhoven, 1996). Misusing the Sullivan method, they obtained values of HapLE by simply multiplying the TLE at birth by the average happiness score. There are at least three problems with this procedure. First, the average happiness score is not equivalent to the prevalence rate. Second, the HapLE calculated is based on TLE at birth and happiness scores that were assessed in adults, making age-specific interpretation difficult. The authors justified this procedure by assuming no age differences in levels of happiness—but this assumption is disproved by numerous empirical studies that clearly document substantial age differences (e.g., Blanchflower and Oswald, 2004; Easterlin, 2001; George, 2006). Third, this estimation procedure rests on TLE instead of the key life table parameter, person-years, which violates the principle of calculating life expectancies and may yield implicit biases that are hard to quantify.
There were also multiple items tapping life satisfaction in the GSS. The assessment of life satisfaction, therefore, requires construction of an index or scale that sums these items with responses ranging from 1 (=a very great deal) to 7 (=none) for each item. Because life satisfaction is measured using domain-specific items that do not evaluate life-as-a-whole, it is not accepted as a valid indicator in the World Database of Happiness. And these items are only available for some but not all years from 1973 to 1994. Because of the difficulty in the operationalizations and the limited availability of the measure, the present study focuses on happiness. Previous research suggests that results based on these various measures of subjective well-being should largely resemble each other.
The decennial life tables for 1969–1971, 1979–1981, and 1989–1991 are from http://www.cdc.gov/nchs/data/lifetables/life69_1_1.pdf, / life79_1_1.pdf, and /life89_1_1.pdf, respectively. And the 2000 life tables are from http://www.cdc.gov/nchs/data/nvsr/nvsr51/nvsr51_03.pdf.
Data for 1980, 1990, and 2000 are pooled with those from the 3 years including and surrounding these years; data for 1970 are pooled with those from 1972 to 1974. Studies of happiness trends have shown that the levels of general happiness in 1970 were similar to those in the early 1970s (Rodgers, 1982). The data for sex–race-specific groups exhibit the same patterns and are not presented in the interest of space.
Population life tables for the U.S. are calculated for the resident population, which includes both the institutionalized and noninstitutionalized populations. However, the sampling frame of the General Social Survey does not include the institutionalized population in the U.S. Without data on subjective well-being from institutionalized population, this study assumes that institutionalized individuals have the same prevalence rates of happiness as the noninstitutionalized population. It is possible that older adults residing in nursing homes due to various health or social reasons are on average less happy than community dwelling individuals. To ascertain the degree to which this leads to an overestimate of the happy life expectancy, the study used the available institutionalized life expectancy for U.S. population (Crimmins et al., 1997) to adjust the present estimates of happy life expectancy by simulating the worst scenario where all the years expected to be lived in institutions are unhappy.
In the extreme hypothetical scenario where all the years expected to be lived in institutions are unhappy, there were only slight reductions in happy life expectancy. For instance, happy life expectancy decreased 0.41 year for men and 0.88 year for women at age 65 in 1970. The decreases were 0.51 year for men and 1.2 years for women at the same age in 1990. Similar amount of reductions occurred to estimates of happy life expectancy at age 85. So any scenarios less extreme would lead to even smaller reductions in happy life expectancy. These results are also consistent with the simulation results of changes in life expectancy in well-being in the Netherlands when taking institutionalized population into account (Perenboom et al., 2004). Because there has been a trend toward deinstitutionalization of the U.S. population, that is, the institutionalized population continued to decline at most ages during the past few decades, this trend was found to have very little effect on the length of disabled life (Crimmins et al., 1997). Similarly, this study concludes that the happiness rates of the institutionalized population barely affect the overall trend of the happy life expectancy.
References
- Baltes MM, Carstensen LL. The process of successful aging: selection, optimization, and compensation. In: Staudinger UM, Lindenberger U, editors. Understanding Human Development: Dialogues with Life-span Psychology. Kluwer Academic Publishers; Dordrecht, Netherlands: 2003. pp. 81–104. [Google Scholar]
- Blanchflower DG, Oswald AJ. Well-being over time in Britain and the USA. Journal of Public Economics. 2004;88:1359–1386. [Google Scholar]
- Covinksy KE, Wu AW, Landefeld CS, Connors AF, Phillips RS, Jr, Tsevat J, Dawson NV, Lynn J, Fortinsky RH. Health status versus quality of life in older patients: does the distinction matter? American Journal of Medicine. 1999;106:435–440. doi: 10.1016/s0002-9343(99)00052-2. [DOI] [PubMed] [Google Scholar]
- Crimmins EM, Saito Y. Trends in healthy life expectancy in the United States 1970–1990. Social Science and Medicine. 2001;52:1629–1641. doi: 10.1016/s0277-9536(00)00273-2. [DOI] [PubMed] [Google Scholar]
- Crimmins EM, Saito Y, Ingegneri D. Changes in life expectancy and disability-free life expectancy in the United States. Population and Development Review. 1989;15:235–267. [Google Scholar]
- Crimmins EM, Saito Y, Ingegneri D. Trends in disability-free life expectancy in the United States, 1970–90. Population and Development Review. 1997;23:555–572. [Google Scholar]
- Davis JA. New money, an old man/lady and ‘two’s company’: subjective welfare in the NORC General Social Surveys, 1972–1982. Social Indicators Research. 1984;15:319–350. [Google Scholar]
- Davis JA, Smith TW. General Social Surveys, 1972–2004. National Opinion Research Center; Chicago: 2005. [Google Scholar]
- Deeg DJH, Westendorp DE, Serriere M. Autonomy and well-being in the aging population. I. Report from the longitudinal aging study Amsterdam 1992–1993. VU University Press; Amsterdam: 1994. [Google Scholar]
- Diener E. Subjective well-being. Psychological Bulletin. 1984;95:542–575. [PubMed] [Google Scholar]
- Diener E, Suh ME. Subjective well-being and age: an international analysis. In: Schaie KW, Lawton MP, editors. Annual Review of Gerontology and Geriatrics. Vol. 17. Academic Press; New York: 1997. pp. 218–235. [Google Scholar]
- di Tella R, MacCulloch RJ, Oswald AJ. The macroeconomics of happiness. The Review of Economics and Statistics. 2003;85:809– 827. [Google Scholar]
- Easterlin RA. Life cycle welfare: trends and differences. Journal of Happiness Studies. 2001;2:1–12. [Google Scholar]
- Easterlin RA. Happiness of women and men in later life: nature, determinants, and prospects. In: Joseph Sirgy M, Rahtz Don R, Coskun Samli A, editors. Advances in Quality-of-Life Theory and Research. Kluwer Academic Publishers; Dordrecht, The Netherlands: 2003. pp. 13–26. [Google Scholar]
- Fries JF. Aging, natural death, and the compression of morbidity. The New England Journal of Medicine. 1980;303:105–130. doi: 10.1056/NEJM198007173030304. [DOI] [PubMed] [Google Scholar]
- George LK. Subjective well-being: conceptual and methodological issues. Annual Review of Gerontology and Geriatrics. 1981;2:345– 382. [Google Scholar]
- George LK. Economic status and subjective well-being. In: Cutler NE, Gregg DW, Lawton MP, editors. Aging, Money, and Life Satisfaction. Springer; New York: 1992. pp. 69–100. [Google Scholar]
- George LK. Life course perspectives on mental health. In: Aneshensel CS, Phelan JC, editors. Handbook of the Sociology of Mental Health. Kluwer Academic/Plenum Publishers; New York: 1999. pp. 565–584. [Google Scholar]
- George LK. Perceived quality of life. In: Binstock RH, George LK, editors. Handbook of Aging and the Social Sciences. 6. Elsevier; San Diego, CA: 2006. pp. 320–336. [Google Scholar]
- Gruenberg EM. The failure of success. Milbank Memorial Fund Quarterly/Health and Society. 1977;55:3–24. [PubMed] [Google Scholar]
- Hagerty MR, Veenhoven R. Wealth and happiness revisited—growing national income does go with greater happiness. Social Indicators Research. 2003;64:1–27. [Google Scholar]
- Heady BW, Wearing AJ. A theory of subjective well-being. Longman Cheshire; Melbourne, Australia: 1992. Understanding happiness. [Google Scholar]
- Hughes M, Thomas ME. The continuing significance of race revisited: a study of race, class, and quality of life in America, 1972 to 1996. American Sociological Review. 1998;63:785–795. [PubMed] [Google Scholar]
- Imai K, Soneji S. On the estimation of disability-free life expectancy: Sullivan’s method and its extension. Journal of American Statistical Association. doi: 10.1198/016214507000000040. forthcoming. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Inglehard R. Gender, aging, and subjective well-being. International Journal of Comparative Sociology. 2002;43:391–408. [Google Scholar]
- Katz S, Branch LG, Branson MH, Papsidero JA, Beck JC, Creer DS. Active life expectancy. New England Journal of Medicine. 1983;309:1218–1224. doi: 10.1056/NEJM198311173092005. [DOI] [PubMed] [Google Scholar]
- Kramer M. The rising pandemic of mental disorders and associated chronic diseases and disabilities. Acta Psychiatrica Scandinavica. 1980;62:282–297. [Google Scholar]
- Kunst AE, Okma-VanKeulen PT, Veenhoven R. Happy life expectancy in 5 European countries. Paper presented at the XIII World Congress of Sociology; Bielefield, Germany. July 1994.1994. [Google Scholar]
- Laditka SB, Hayward MD. The evolution of demographic methods to calculate health expectancies. In: Robine J, et al., editors. Determining Health Expectancies. John Wiley and Sons Ltd; Atrium, England: 2003. pp. 221–234. [Google Scholar]
- Land KC, Guralnik JM, Blazer DG. Estimating increment–decrement life tables with multiple covariates from panel data: the case of active life expectancy. Demography. 1994;31:297–319. [PubMed] [Google Scholar]
- Manton KG, Land KC. Active life expectancy estimates for the U.S. elderly population: a multidimensional continuous-mixture model of functional change applied to completed cohorts, 1982–1996. Demography. 2000;37:253–265. [PubMed] [Google Scholar]
- Mathers CD, Robine JM. How good is Sullivan’s method for monitoring changes in population health expectancies. Journal of Epidemiology and Community Health. 1997;51:80–86. doi: 10.1136/jech.51.1.80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mroczek DK, Spiro A. Change in life satisfaction during adulthood: findings from the Veterans Affairs Normative Aging Study. Journal of Personality and Social Psychology. 2005;88:189–202. doi: 10.1037/0022-3514.88.1.189. [DOI] [PubMed] [Google Scholar]
- Nam CB. Another look at mortality crossovers. Social Biology. 1995;42:133–142. doi: 10.1080/19485565.1995.9988893. [DOI] [PubMed] [Google Scholar]
- Nusselder W. Compression or Expansion of Morbidity: A Life-Table Approach. Erasmus University of Rotterdam; Rotterdam, The Netherlands: 1997. [Google Scholar]
- Olshansky SJ, Rudberg MA, Carnes BA, Cassel CK, Brody JA. Trading off longer life for worsening health. Journal of Aging and Health. 1991;3:194–216. [Google Scholar]
- Pennex B, Guralnik JM, Simonsick EM, Kasper JD, Ferrucci L, Fried LP. Emotional vitality among disabled older women: the women’s health and aging study. Journal of the American Geriatrics Society. 1998;46:807–815. doi: 10.1111/j.1532-5415.1998.tb02712.x. [DOI] [PubMed] [Google Scholar]
- Perenboom RJ, van Oyen H, Mutafova M. Health expectancies in European countries. In: Robine J, et al., editors. Determining Health Expectancies. John Wiley and Sons Ltd; Atrium, England: 2003. pp. 359–376. [Google Scholar]
- Perenboom RJM, van Herten LM, Boshuizen HC, van Den Bos GAM. Trends in life expectancy in well-being. Social Indicators Research. 2004;65:227–244. [Google Scholar]
- Pinqart M, Soerensen S. Gender differences in self-concept and psychological well-being in old age: a meta-analysis. Journal of Gerontology: Psychological Sciences. 2001;56B:195–213. doi: 10.1093/geronb/56.4.p195. [DOI] [PubMed] [Google Scholar]
- Preston SH, Heuveline P, Guillot M. Demography: Measuring and Modeling Population Processes. Blackwell; Malden, MA: 2001. [Google Scholar]
- Preston SH, Elo IT, Rosenwaike I, Hill M. African-American mortality at older ages: results of a matching study. Demography. 1996;33:193–209. [PubMed] [Google Scholar]
- Ritchie K, Polge C. Mental health expectancy. In: Robine J, et al., editors. Determining Health Expectancies. John Wiley and Sons Ltd; Atrium, England: 2003. pp. 175–185. [Google Scholar]
- Robine JM, Ritchie K. Healthy life expectancy: evaluation of global indicator of change in population health. British Medical Journal. 1991;302:457–460. doi: 10.1136/bmj.302.6774.457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robine J-M, Jagger C, Mathers CD, Crimmins EM, Suzman RM, editors. Determining Health Expectancies. John Wiley and Sons Ltd; Atrium, England: 2003. [Google Scholar]
- Rodgers W. Trends in reported happiness within demographically defined subgroups, 1957–78. Social Forces. 1982;60:826–842. [Google Scholar]
- Sanders BS. Measuring community health levels. American Journal of Public Health. 1964;54:1063–1070. doi: 10.2105/ajph.54.7.1063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saris WE, Veenhoven R, Scherpenzeel A, Bunting B, editors. A comparative study of satisfaction with life in Europe. Eötvös University Press; Budapest, Hungary: 1996. [Google Scholar]
- Spain D, Bianchi SM. Balancing act: motherhood, marriage, and employment among American women. Russell Sage Foundation; New York: 1996. [Google Scholar]
- Steverink N, Westerhof GJ, Bode C, Dittmann-Kohli F. The personal experience of aging, individual resources, and subjective well-being. Journal of Gerontology: Psychological Sciences. 2001;56B:364–373. doi: 10.1093/geronb/56.6.p364. [DOI] [PubMed] [Google Scholar]
- Sullivan DF. A single index of mortality and morbidity. HSMHA Health Reports. 1971;86:347–354. [PMC free article] [PubMed] [Google Scholar]
- Veenhoven R. Conditions of happiness. Kluwer Academic; Boston: [1984] 1991. Reprint. [Google Scholar]
- Veenhoven R. Happiness in nations. World Database of Happiness, Distributional Findings in Nations, Erasmus University Rotterdam. 1992 Retrieved December 4, 2006, from: http://www.worlddatabaseofhappiness.eur.nl.
- Veenhoven R. Happy life expectancy: a comparative measure of quality of life in nations. Social Indicators Research. 1996;39:1–58. [Google Scholar]
- Veenhoven R. Advances in understanding happiness. Revue Québécoise de Psychologie. 1997;18:29–74. [Google Scholar]
- World Health Organization. World Health Organization Charter. Geneva: 1946. [Google Scholar]
- The WHOQOL Group. Development of the World Health Organization WHOQOL—BREF quality of life assessment. Psychological Medicine. 1998;28:551–558. doi: 10.1017/s0033291798006667. [DOI] [PubMed] [Google Scholar]
- Yang Y. Is old age depressing? Growth trajectories and cohort variations in late life depression. Journal of Health and Social Behavior. 2007;48:16–32. doi: 10.1177/002214650704800102. [DOI] [PubMed] [Google Scholar]