

Abstract
Objective
Sudden major cerebral artery occlusion often resists recanalization with currently available techniques or can results in massive symptomatic intracranial hemorrhage (sICH) after thrombolytic therapy. The purpose of this study was to examine mechanical recanalization with a retrievable self-expanding stent and balloon in acute intracranial artery occlusions.
Methods
Twenty-eight consecutive patients with acute intracranial artery occlusions were treated with a Solitaire retrievable stent. Balloon angioplasty was added if successful recanalization was not achieved after stent retrieval. The angiographic outcome was assessed by Thrombolysis in Cerebral Infarction (TICI) and the clinical outcomes were assessed by the National Institutes of Health Stroke Scale (NIHSS) and the modified Rankin Scale (mRS).
Results
At baseline, mean age was 69.4 years and mean initial NIHSS score was 12.5. A recanalization to TICI 2 or 3 was achieved in 24 patients (85%) after stent retrieval. Successful recanalization was achieved after additional balloon angioplasty in 4 patients. At 90-day follow-up, 24 patients (85%) had a NIHSS improvement of ≥4 and 17 patients (60%) had a good outcome (mRS ≤2). Although there was sICH, there was one death associated with the procedure.
Conclusion
Mechanical thromboembolectomy with a retrievable stent followed by additional balloon angioplasty is a safe and effective first-line therapy for acute intracranial artery occlusions especially in case of unsuccessful recanalization after stent thrombectomy.
Keywords: Acute cerebral artery occlusion, Mechanical recanalization, Retrievable stent, Balloon angioplasty
INTRODUCTION
Thromboembolic occlusion of major cerebral arteries is usually a very serious condition and successful recanalization improves outcomes. Unfortunately, such lesions are often refractory to intravenous (IV) and/or intra-arterial (IA) thrombolysis1,15,25,28). Endovascular intervention offers good result in the treatment of acute ischemic stroke in patients presenting beyond the 4.5-hour time window, as well as in patients presenting in less than 4.5-hours who are ineligible for tissue plasminogen activator (tPA) or have failed to respond to IV tPA.
Endovascular recanalization with an IA chemical thrombolytic agent was commonly performed in the past. However, these agents are known to frequently cause symptomatic intracranial hemorrhage (sICH)3,7,25). Several reports about mechanical thrombolysis in acute ischemic stroke have been published over the past decade including a new technique with the Solitaire® AB/FR device (EV3, Irvine, CA, USA) with favorable outcomes5,19,20). Even with the new technique, some cases of large artery occlusion were not resolved with retrievable stent therapy alone.
We collected data from 28 consecutive patients with acute ischemic stroke who were treated with the Solitaire AB/FR stent device. Some of these patients also received balloon angioplasty when recanalization failed with Solitaire stent. We report the results of recanalization and overall outcomes.
MATERIALS AND METHODS
Data were analyzed from interventional database at our Stroke Center between March 2011 and December 2011. All patients treated with Solitaire retrievable stent for acute cerebral artery occlusion were included in this study. Some patients underwent additional balloon angioplasty when recanalization failed with stent alone. As a protocol for acute stroke patient in our stroke center, all patients who present with symptoms suspicious of acute ischemic stroke are initially examined with a CT scan. In addition to plain CT, CT angiography and perfusion CT are done at the same session. If intracranial hemorrhage was excluded by CT, diffusion magnetic resonance (MR) and 4-vessel angiography were performed. Inclusion criteria for mechanical recanalization in this study were as follows : 1) clinical diagnosis of acute stroke by a stroke neurologist; 2) baseline National Institutes of Health Stroke Scale (NIHSS) score ≥4, except for isolated aphasia or hemianopsia; 3) exclusion of hemorrhage as determined by cranial CT; 4) large vessel occlusion [intracranial internal carotid artery (ICA), A1 of anterior cerebral artery, M1-M2 of middle cerebral artery (MCA), vertebrobasilar artery] with correlating neurological deficits; 5) large perfusion-diffusion mismatch between perfusion CT and diffusion MR; and 6) initiation of treatment within 8 hours after symptom onset for hemispheric stroke and 12 hours for vertebrobasilar stroke.
All patients who were included in these criteria went through recanalization with Solitaire stent during study period. Balloon was used as secondary method when recanalization failed.
Procedure
Patients were sedated with 50-100 ug of fentanyl. Diagnostic cerebral angiography was performed to assess the site of vessel occlusion and collateral circulation. Collateral flow was graded based on the system proposed by the American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology13) : grade 0, no collateral visible to the ischemic site; grade 1, slow collateral to the periphery of some of the defect and to only a portion of the ischemic territory; grade 2, rapid collaterals to the periphery of the ischemic site with persistence of some of the defect and to only a portion of the ischemic territory; grade 3, collateral with slow but complete angiographic blood flow to the ischemic bed occurring by the late venous phase; grade 4, complete and rapid collateral blood flow to the vascular bed of the entire ischemic territory by retrograde perfusion.
For the endovascular procedure, a 6- to 7-French (Fr) guiding catheter was placed in the cervical ICA or VA, depending on vessel diameter. The guiding catheter was continuously flushed with heparinized saline (10 IU/mL). Using standard cerebral catheterization techniques, the microcatheter was guided into the occluded vessel and passed through the occluded area. The length and shape of the occlusion segment was assessed with selective angiography using a microcatheter (Excelsior® SL-10, Stryker, Natick, MA, USA) to distal portion of occlusion segment. Another larger microcatheter (Rebar®-18, EV3, Irvine, CA, USA) replaced along the long type microwire (Transcend®-300, Stryker, Natick, MA, USA). The Solitaire stent was advanced through the microcatheter and fully deployed in the occluded segment. Stents were slightly oversized to allow proper adjustment to the vessel wall (4 to 6 mm diameter, 15 to 20 mm length). Additional angiography was performed immediately after stent deployment and before stent retrieval. Five minutes after deployment, the unsheathed Solitaire stent was removed with the microcatheter. One assistant compressed the common carotid artery to block the anterograde flow of the ICA and another assistant aspirated the guiding catheter gently with a 50 cc syringe to prevent thrombus migration during stent retrieval. Angiography was performed after complete retraction of the Solitaire stent. When occlusion persisted, the procedure was repeated once again with the re-captured stent. The results of recanalization were assessed by angiography immediately after the procedure according to the Thrombolysis in Cerebral Infarction (TICI) criteria13). Demographic, clinical and laboratory data including neurological and physical examinations, NIHSS, routine blood analysis and 12-lead ECG were recorded for each patient.
When successful recanalization (TICI of 2 or 3) was still not achieved with second stent retrieval, balloon angioplasty was performed at the occluded segment. The distal artery was selected with a microcatheter, and the microwire was exchanged with a longer microwire (Transcend®-300, Stryker). The microcatheter was exchanged with the angioplasty balloon and advanced into the occluded segment. The Gateway balloon® (Stryker, Natick, MA, USA), an over-the-wire type, was used. The balloon diameter was 2/3 to 3/4 normal vessel diameter and the length was 5-10 mm longer than the occluded segment. After positioning the balloon at the occluded segment, the balloon was inflated slowly up to nominal pressure and maintained for 120 seconds. Thromboembolectomy with Solitaire stent was then repeated once again when recanalization was not sufficient.
Although permanent stent deploy was avoided as much as possible, it was used if sufficient recanalization could only be obtained with the stent deployment. In such cases, aspirin (300 mg) and clopidogrel (300 mg) were administered using a Levin tube before stent placement.
Patient care and follow-up
Immediately after recanalization, systolic blood pressure was controlled between 100-120 mm Hg using continuous IV nicardipine to prevent hyperperfusion injury. All patients underwent CT immediately after the procedure to verify the absence of hemorrhagic transformation. After exclusion of hemorrhage, long-term aspirin (100 mg/d) was prescribed. Additional CT or MR imaging was performed whenever a patient shows deterioration clinically. CT angiography and perfusion CT were performed within 72 hours and again 90 days after intervention. The occurrence of sICH was defined as clinical deterioration (4-point increase or more in the NIHSS or 1-point deterioration in the level of consciousness) combined with a space-occupying brain hematoma on the CT or MR image3,9,14).
Clinical outcomes were evaluated with 90-day modified Rankin Scale (mRS), NIHSS, and 90-day mortality. An mRS of 0 to 2 was defined as a good outcome, 3 as moderate and 4-6 as poor.
RESULTS
A total of 28 patients were treated with endovascular recanalization during the study period. Eighteen were male and ten were female. Mean age was 69.4 years and mean initial NIHSS score was 12.5. The mean time interval from stroke onset to hospital visit was 376 minutes. After initial CT, two patients who were within 3 hours of symptom onset were treated with IV tPA (0.9 mg/kg) without clinical improvement over one hour. Baseline characteristics and demographic data are listed in Table 1.
Table 1.
Baseline characteristics of patients
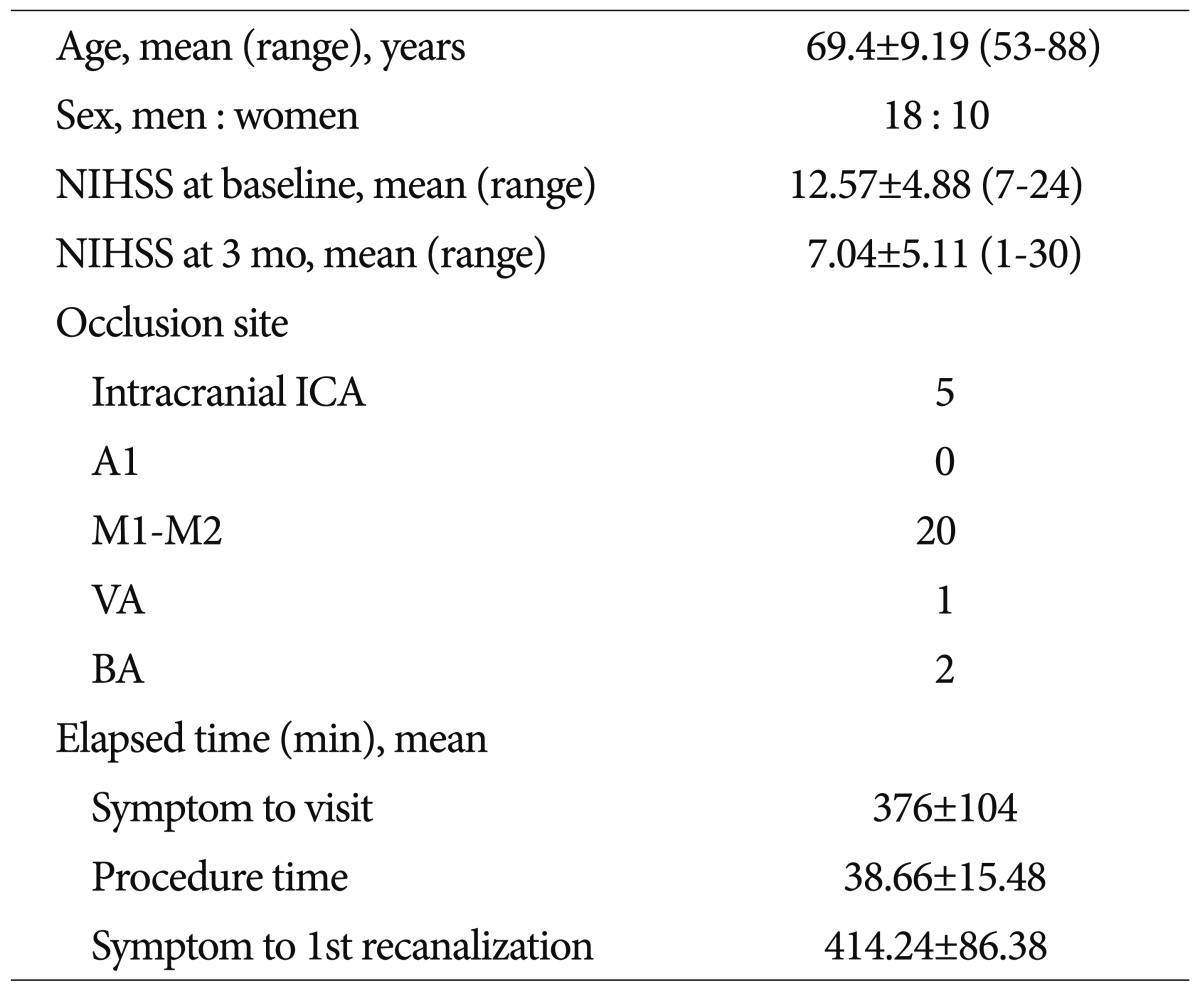
NIHSS : National Institutes of Health Stroke Scale, ICA : internal carotid artery
Angiographic outcome
By the end of thromboembolectomy with a retrievable stent, 24 patients demonstrated grade 2 or 3 recanalization according to the TICI grading system. Nine patients acquired successful recanalization after second time stent retrieval. Mean time from femoral puncture to first successful recanalization was 38.6 min. New occlusion of a distal artery from migration of the lost clot was observed in two patients with no neurologic deterioration. Balloon angioplasty was performed in four patients who showed insufficient recanalization (TICI of 0-1) after a second attempt of thromboembolectomy with Solitaire. It took an additional 7-10 minutes from balloon catheter preparation to 1st angiography after balloon angioplasty. The location of occlusion was M1 in three cases and distal ICA (ophthalmic segment) in one case. Successful recanalization was achieved after balloon angioplasty in two patients and after additional stent retrieval in one patient with M1 occlusion. Recanalization was failed even after stent retrieval and balloon angioplasty in one patient with distal ICA occlusion, and recanalization was achieved after permanent stent deployment. Combination thromboembolectomy with stent retrieval and balloon angioplasty is illustrated in Fig. 1. Finally, we successfully recanalized all patients with single Solitaire or combined balloon angioplasty.
Fig. 1.

A case illustration for combination of thromboembolectomy with stent retrieval and balloon angioplasty of a 59-year-old male presenting with motor weakness of the left arm and leg. Right internal carotid artery (ICA) angiography before recanalization (A) reveals an acute thromboembolic occlusion of the right distal ICA. Right ICA angiography after recanalization shows severe stenosis of the distal ICA-M1 segment after stent deployment (B) and M1 segment occlusion even after repeating stent retrieval (C). After angioplasty with Gateway balloon (2.0×15 mm) (D), angiography shows successful recanalization (TICI grade 3) (E). TICI : Thrombolysis in Cerebral Infarction.
No patient showed re-occlusion or severe stenosis (>70% of normal vessel) at 90-day follow up.
Clinical outcomes
The NIHSS score before recanalization and at 90-day follow-up is presented in Fig. 2. Most patients with successful recanalization showed immediate improvement of clinical symptoms. Twenty-four of 28 patients showed an NIHSS decrease of more than three points in three days and nine showed a decrease of more than five points. Definite neurologic improvement was not seen in the other three patients, even after successful recanalization.
Fig. 2.

Comparison of National Institutes of Health Stroke Scale (NIHSS) scores before and after recanalization.
Brain CT scans within 72 hours of treatment demonstrated no sICH. One patient died from progression of the MCA territory infarction and severe brain edema, despite successful recanalization. At three-month follow-up, 17 patients had a good outcome (mRS of 0 to 2), 6 moderate (mRS of 3), and 5 poor (mRS of 4 to 6).
DISCUSSION
Early recanalization of acute thromboembolic occlusions of intracranial arteries can remarkably improve the life quality of patient9,21,29). The tPA trials of NINDS suggested that treatment within 3 to 4.5 hours from symptom onset was beneficial despite an increased risk of symptomatic hemorrhage22,25,26). Unfortunately, presentation beyond the narrow therapeutic time window is the leading cause of treatment disqualification4,10). Over the past decade, thrombolytic agents like urokinase, tirofiban and abciximab were commonly used in IA thrombolysis and some resulted in a good prognosis. Even so, IA thrombolysis always has a risk of sICH, especially when a large amount of thrombolytic agent is used3,7,25).
Compared to IA fibrinolytic strategies, mechanical thromboembolectomy offers the advantage of a potential reduction in the rate of hemorrhagic transformation. The MERCI trials demonstrated that endovascular mechanical thromboembolectomy is technically efficacious in achieving recanalization in patients within 8 hours of stroke onset10,11,23,24). The Penumbra system has shown promising clinical outcome, with successful recanalization in 82 to 100% of cases2,12,17). Nevertheless, these instruments have some flaws, such as occasional difficulty passing a carotid siphon due to its relatively large profile, especially in elderly patients with tortuous vessels. The repetitive push and pull action of the separator wire also increases the possibility of vessel injury or perforation resulting in reocclusion or hemorrhage. In real practice, the efficacy of recanalization was also not as high as the former studies8,23,24).
The Solitaire AB/FR stent has recently been considered as a part of the standard care for acute intracranial artery occlusion. There is no difference in device design between the AB and FR variants. This device advances in the microcatheter and can approach almost every vessel that is selected with the microcatheter. The Solitaire device is an intracranial stent that is fully retrievable after full deployment and there is no need for aggressive antiplatelet therapy. Several recent studies suggested a good revascularization rate with the Solitaire stent6,16,18,27).
Despite promising results, thromboembolectomy with Solitaire is not a panacea. Recanalization can fail in cases when severe stenosis is accompanied by occlusion, when an occlusive clot is attached firmly to the endothelium, or when the clot is too hard to be opened by a self-expandable stent strut, or when severe vasospasm happens after thromboembolectomy. In such situations, the occlusive clot cannot be removed efficiently and balloon angioplasty can be an effective secondary method. A balloon can dilate the stenosis or spasm, loosen the endothelial-clot attachment, and shatter hard clot, enabling efficacious clot removal and recanalization.
In our consecutive case-review series with the Solitaire stent alone, we were able to achieve a successful revascularization rate of 85.7%. The other patients, who failed recanalization after stent retrieval, also achieved successful recanalization after balloon angioplasty or permanent stent deployment. Complete revascularization was achieved in 60% (TICI of 3). Though our study is limited by small sample size, our results suggest that most patients with failed Solitaire thromboembolectomy can achieve successful recanalization with subsequent balloon angioplasty. We utilized an over-the-wire type Gateway balloon®, which is more easily advanced to the distal vessel than the same sized monorail type. Although we avoided permanent stent deploy if possible, successful recanalization was failed in one patient even after stent retrieval and balloon angioplasty, and sufficient blood flow was achieved after permanent stent deploy.
With this single or combined procedure, we achieved a recanalization rate of 100% (TICI of 2 or 3). The mean time from femoral puncture to recanalization was only 38 mins (range 20-62). After recanalization, 85% of the patients experienced a ≥4-point improvement on the NIHSS score at discharge and 60% of patients achieved a good clinical outcome at three months. Remarkably, occurrence of sICH in our patients was significantly retrievlower than previous studies. The lack of sICH after recanalization in our patient series may be explained by several factors, including proper sedation during the procedure, non-excessive angioplasty, strict blood pressure control, and above all, avoidance of IA thrombolytic agents. The mortality during study period in this consecutive series was 3.5%, as one patient had died at three-month follow-up.
There are, however, some drawbacks to the use of intracranial stents and balloons for acute recanalization in ischemic stroke. One concern is the migration of a thromboembolic fragment. Clot migration was observed in only two cases in our consecutive case analysis perhaps because most of the clot was removed with aspiration of the guiding catheter during stent retrieval. There was no aggravation of the neurological deficit or enlargement of infarction size in these two cases.
Another concern with our procedure is the possibility of causing endothelial injury or dissection during stent retrieval or angioplasty, which can lead to secondary stenosis or blood leakage. Fortunately, there was no dissection or secondary stenosis during our study. The risk of vessel injury increases with amount of atherosclerotic stenosis. Finally, the risk of hyperperfusion also increases if there is preexisting, severe and chronic stenosis. It is important not to attempt full recovery of vessel diameter as even small increases in radius greatly increase the volume of flow according to Poiseuille's law. In our opinion, 50-70% restoration of the normal diameter is sufficient for saving the penumbra and preventing hyperperfusion. If a perfusion defect is discovered on follow-up study, it is not too late to carry out additional angioplasty or stent deployment.
CONCLUSION
The Solitaire device is technically safe and effective in clearing cerebral thrombi and restoring flow to the neurovasculature. Also, balloon angioplasty is an effective secondary procedure when sufficient restoration of blood flow is not achieved with stenting alone. Although our case number is small and a larger scale study is required, the combination of a retrievable stent and balloon is a promising first-line therapy for acute occlusion of intracranial artery due to its high success rate and low complication rate.
References
- 1.Arnold M, Nedeltchev K, Mattle HP, Loher TJ, Stepper F, Schroth G, et al. Intra-arterial thrombolysis in 24 consecutive patients with internal carotid artery T occlusions. J Neurol Neurosurg Psychiatry. 2003;74:739–742. doi: 10.1136/jnnp.74.6.739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bose A, Henkes H, Alfke K, Reith W, Mayer TE, Berlis A, et al. The Penumbra System : a mechanical device for the treatment of acute stroke due to thromboembolism. AJNR Am J Neuroradiol. 2008;29:1409–1413. doi: 10.3174/ajnr.A1110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Brekenfeld C, Remonda L, Nedeltchev K, Arnold M, Mattle HP, Fischer U, et al. Symptomatic intracranial haemorrhage after intra-arterial thrombolysis in acute ischaemic stroke : assessment of 294 patients treated with urokinase. J Neurol Neurosurg Psychiatry. 2007;78:280–285. doi: 10.1136/jnnp.2005.078840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Broderick JP, Lu M, Kothari R, Levine SR, Lyden PD, Haley EC, et al. Finding the most powerful measures of the effectiveness of tissue plasminogen activator in the NINDS tPA stroke trial. Stroke. 2000;31:2335–2341. doi: 10.1161/01.str.31.10.2335. [DOI] [PubMed] [Google Scholar]
- 5.Castaño C, Dorado L, Guerrero C, Millán M, Gomis M, Perez de la Ossa N, et al. Mechanical thrombectomy with the Solitaire AB device in large artery occlusions of the anterior circulation : a pilot study. Stroke. 2010;41:1836–1840. doi: 10.1161/STROKEAHA.110.584904. [DOI] [PubMed] [Google Scholar]
- 6.Cohen JE, Gomori JM, Leker RR, Moscovici S, Ramirez-Denoriega F, Itshayek E. Recanalization with stent-based mechanical thrombectomy in anterior circulation major ischemic stroke. J Clin Neurosci. 2012;19:39–43. doi: 10.1016/j.jocn.2011.06.015. [DOI] [PubMed] [Google Scholar]
- 7.Eckert B, Koch C, Thomalla G, Kucinski T, Grzyska U, Roether J, et al. Aggressive therapy with intravenous abciximab and intra-arterial rtPA and additional PTA/stenting improves clinical outcome in acute vertebrobasilar occlusion : combined local fibrinolysis and intravenous abciximab in acute vertebrobasilar stroke treatment (FAST) : results of a multicenter study. Stroke. 2005;36:1160–1165. doi: 10.1161/01.STR.0000165918.80812.1e. [DOI] [PubMed] [Google Scholar]
- 8.Flint AC, Duckwiler GR, Budzik RF, Liebeskind DS, Smith WS MERCI and Multi MERCI Writing Committee. Mechanical thrombectomy of intracranial internal carotid occlusion : pooled results of the MERCI and Multi MERCI Part I trials. Stroke. 2007;38:1274–1280. doi: 10.1161/01.STR.0000260187.33864.a7. [DOI] [PubMed] [Google Scholar]
- 9.Furlan A, Higashida R, Wechsler L, Gent M, Rowley H, Kase C, et al. Intra-arterial prourokinase for acute ischemic stroke. The PROACT II study : a randomized controlled trial. Prolyse in Acute Cerebral Thromboembolism. JAMA. 1999;282:2003–2011. doi: 10.1001/jama.282.21.2003. [DOI] [PubMed] [Google Scholar]
- 10.Furlan AJ. CVA : reducing the risk of a confused vascular analysis. The Feinberg lecture. Stroke. 2000;31:1451–1456. doi: 10.1161/01.str.31.6.1451. [DOI] [PubMed] [Google Scholar]
- 11.Gobin YP, Starkman S, Duckwiler GR, Grobelny T, Kidwell CS, Jahan R, et al. MERCI 1 : a phase 1 study of Mechanical Embolus Removal in Cerebral Ischemia. Stroke. 2004;35:2848–2854. doi: 10.1161/01.STR.0000147718.12954.60. [DOI] [PubMed] [Google Scholar]
- 12.Grunwald IQ, Walter S, Papanagiotou P, Krick C, Hartmann K, Dautermann A, et al. Revascularization in acute ischaemic stroke using the penumbra system : the first single center experience. Eur J Neurol. 2009;16:1210–1216. doi: 10.1111/j.1468-1331.2009.02750.x. [DOI] [PubMed] [Google Scholar]
- 13.Higashida RT, Furlan AJ, Roberts H, Tomsick T, Connors B, Barr J, et al. Trial design and reporting standards for intra-arterial cerebral thrombolysis for acute ischemic stroke. Stroke. 2003;34:e109–e137. doi: 10.1161/01.STR.0000082721.62796.09. [DOI] [PubMed] [Google Scholar]
- 14.Kase CS, Furlan AJ, Wechsler LR, Higashida RT, Rowley HA, Hart RG, et al. Cerebral hemorrhage after intra-arterial thrombolysis for ischemic stroke : the PROACT II trial. Neurology. 2001;57:1603–1610. doi: 10.1212/wnl.57.9.1603. [DOI] [PubMed] [Google Scholar]
- 15.Kim YS, Garami Z, Mikulik R, Molina CA, Alexandrov AV CLOTBUST Collaborators. Early recanalization rates and clinical outcomes in patients with tandem internal carotid artery/middle cerebral artery occlusion and isolated middle cerebral artery occlusion. Stroke. 2005;36:869–871. doi: 10.1161/01.STR.0000160007.57787.4c. [DOI] [PubMed] [Google Scholar]
- 16.Koh JS, Lee SJ, Ryu CW, Kim HS. Safety and efficacy of mechanical thrombectomy with solitaire stent retrieval for acute ischemic stroke : a systematic review. Neurointervention. 2012;7:1–9. doi: 10.5469/neuroint.2012.7.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kulcsár Z, Bonvin C, Pereira VM, Altrichter S, Yilmaz H, Lövblad KO, et al. Penumbra system : a novel mechanical thrombectomy device for large-vessel occlusions in acute stroke. AJNR Am J Neuroradiol. 2010;31:628–633. doi: 10.3174/ajnr.A1924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Machi P, Lobotesis K, Maldonado IL, Costalat V, Vendrell JF, Riquelme C, et al. Endovascular treatment of tandem occlusions of the anterior cerebral circulation with solitaire FR thrombectomy system. Initial experience. Eur J Radiol. 2012;81:3479–3484. doi: 10.1016/j.ejrad.2011.12.032. [DOI] [PubMed] [Google Scholar]
- 19.Papanagiotou P, Roth C, Walter S, Behnke S, Politi M, Fassbender K, et al. Treatment of acute cerebral artery occlusion with a fully recoverable intracranial stent : a new technique. Circulation. 2010;121:2605–2606. doi: 10.1161/CIRCULATIONAHA.110.948166. [DOI] [PubMed] [Google Scholar]
- 20.Park H, Hwang GJ, Jin SC, Jung CK, Bang JS, Han MK, et al. A retrieval thrombectomy technique with the Solitaire stent in a large cerebral artery occlusion. Acta Neurochir (Wien) 2011;153:1625–1631. doi: 10.1007/s00701-011-0999-0. [DOI] [PubMed] [Google Scholar]
- 21.Rha JH, Saver JL. The impact of recanalization on ischemic stroke outcome : a meta-analysis. Stroke. 2007;38:967–973. doi: 10.1161/01.STR.0000258112.14918.24. [DOI] [PubMed] [Google Scholar]
- 22.Saver JL. Number needed to treat estimates incorporating effects over the entire range of clinical outcomes : novel derivation method and application to thrombolytic therapy for acute stroke. Arch Neurol. 2004;61:1066–1070. doi: 10.1001/archneur.61.7.1066. [DOI] [PubMed] [Google Scholar]
- 23.Smith WS, Sung G, Saver J, Budzik R, Duckwiler G, Liebeskind DS, et al. Mechanical thrombectomy for acute ischemic stroke : final results of the Multi MERCI trial. Stroke. 2008;39:1205–1212. doi: 10.1161/STROKEAHA.107.497115. [DOI] [PubMed] [Google Scholar]
- 24.Smith WS, Sung G, Starkman S, Saver JL, Kidwell CS, Gobin YP, et al. Safety and efficacy of mechanical embolectomy in acute ischemic stroke : results of the MERCI trial. Stroke. 2005;36:1432–1438. doi: 10.1161/01.STR.0000171066.25248.1d. [DOI] [PubMed] [Google Scholar]
- 25.The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med. 1995;333:1581–1587. doi: 10.1056/NEJM199512143332401. [DOI] [PubMed] [Google Scholar]
- 26.Tomsick T, Broderick J, Carrozella J, Khatri P, Hill M, Palesch Y, et al. Revascularization results in the Interventional Management of Stroke II trial. AJNR Am J Neuroradiol. 2008;29:582–587. doi: 10.3174/ajnr.A0843. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Wick MC, Klocker J, Jaschke W, Chemelli A. Endovascular popliteal thrombectomy using the self-expanding, retrievable Solitaire recanalization device. J Endovasc Ther. 2012;19:34–36. doi: 10.1583/11-3680.1. [DOI] [PubMed] [Google Scholar]
- 28.Zaidat OO, Suarez JI, Santillan C, Sunshine JL, Tarr RW, Paras VH, et al. Response to intra-arterial and combined intravenous and intra-arterial thrombolytic therapy in patients with distal internal carotid artery occlusion. Stroke. 2002;33:1821–1826. doi: 10.1161/01.str.0000020363.23725.67. [DOI] [PubMed] [Google Scholar]
- 29.Zangerle A, Kiechl S, Spiegel M, Furtner M, Knoflach M, Werner P, et al. Recanalization after thrombolysis in stroke patients : predictors and prognostic implications. Neurology. 2007;68:39–44. doi: 10.1212/01.wnl.0000250341.38014.d2. [DOI] [PubMed] [Google Scholar]