

Abstract
Objective
The cortical width below the mental foramen of the mandible determined from panoramic radiographs is a useful screening tool for identifying elderly individuals with a low skeletal bone mineral density (BMD). However, whether the mandible cortical width (MCW) is useful for identifying a low skeletal BMD in men and women of 40 years or younger is not known.
Methods
The BMD of the calcaneus was measured by ultrasonography bone densitometry in 158 men and 76 women aged 18–36 years. A logistic regression analysis adjusted for age was used to calculate the odds ratios and 95% confidence interval (CI) of having a low calcaneal BMD, according to the quartiles of the MCW. The areas under the receiver operator characteristic curve (AUC) for identifying participants with a low calcaneal BMD using the MCW were assessed to evaluate the diagnostic efficacy of the MCW.
Results
In men, the adjusted odds ratios of a low calcaneal BMD associated with the second, third and lowest quartiles of MCW were 5.66 (95% CI, 0.61–52.23), 5.43 (95% CI, 0.59–50.18) and 33.22 (95% CI, 3.97–276.94), respectively, compared with the highest quartile, while no significant trend in the adjusted odds ratios was observed in women. The AUC for identifying participants with a low calcaneal BMD based on the MCW was 0.796 (95% CI, 0.702–0.890) in men and 0.593 (95% CI, 0.398–0.788) in women.
Conclusion
MCW determined from panoramic radiographs can be used to identify undetected low calcaneus BMD in young adult men, but not in young adult women.
Keywords: osteoporosis, young adult, ultrasonography, mandible
Introduction
The occurrence of osteoporotic fractures contributes to subsequent new fractures, decreases quality of life and increases mortality risk and incremental medical costs. In Japan, the number of patients with hip fractures in 2005 was approximately three times that in 1987.1 Mortality after hip or spine fractures is relatively high (10%–20%), especially in men.2 In comparison, the number of patients aged 65 years or older with hip fractures in the United States has decreased gradually since 1996.3 The incidence decrease in the United States is coincident with increased use of bisphosphonates. The early detection of patients at risk of osteoporosis and the administration of medication for osteoporosis, such as bisphosphonates and selective oestrogen receptor modulators, can reduce the incidence of hip and other major osteoporotic fractures. Conversely, osteonecrosis of the jaw, a side effect of bisphosphonate, has attracted worldwide attention since first being reported by Marx in 2003,4 although most cases are related to high intravenous injections of bisphosphonates in cancer patients.5 It would be preferable for medical professionals to identify men and women aged 40 years or younger at risk of osteoporosis because they can be treated with exercise and diet therapy without medication.
Many studies have demonstrated the usefulness of cortical indices, such as cortical width and shape, determined from panoramic radiographs, in identifying elderly individuals with undetected low skeletal bone mineral density (BMD) or osteoporosis, especially post-menopausal women.6 Previously, an association between age and the cortical width below the mental foramen of the mandible was observed in 170 Japanese females aged 3–88 years and 99 Japanese males aged 8–69 years.7 In that study, the mandible cortical width (MCW) increased rapidly between 10 and 20 years and decreased rapidly between 50 and 60 years in females only. The distribution of several cortical indices of the mandible on panoramic radiographs and significant associations among age, dentition status and cortical indices of the mandible, including the MCW, were reported in 500 British females aged 25–74 years.8 These two studies evaluated the relationship between age and the MCW, but not between the MCW and the BMD of the entire skeleton. Given the lack of data on the association between the MCW and skeletal mineral status, whether the MCW is also a useful indicator for identifying undetected low skeletal BMD in men and women aged 40 years or younger has remained unknown. Therefore, we sought to clarify the association between the MCW and calcaneal BMD in men and women aged 40 years or younger and to determine whether the MCW is sufficient to identify young adults with undetected low calcaneal BMD.
Materials and Methods
Participants
Of the students attending the School of Dentistry and School of Dental Hygiene at Matsumoto Dental University, Shiojiri, Japan who had panoramic radiographs taken during clinical teaching, 234 healthy students (158 men and 76 women) aged 18–36 years participated in this study. All subjects gave informed consent before the study. The mean ages (±standard deviation (SD)) of the men and women were 24.3 (±3.7) years and 22.9 (±3.3) years, respectively. Students previously or currently undergoing orthodontic treatment were excluded from the study. The ethics committee of Matsumoto Dental University reviewed and approved the study protocol.
BMD assessment and dental panoramic radiography measures
BMD at the right calcaneus as a percentage of the speed of sound (SOS) compared with the young adult mean for each gender was determined using quantitative ultrasonography (QUS; CM-200, Furuno, Kobe, Japan). Two examiners from the Department of Oral and Maxillofacial Radiology of Matsumoto Dental University used a QUS to measure the right calcaneus of three volunteers three times at 1 week intervals to evaluate the intra and interexaminer reproducibility. The coefficient of variation obtained from these data was considered reproducibility. The mean intra and interexaminer reproducibilities were 3.8% and 2.1%, respectively. Low calcaneal BMD was defined as a SOS <80% of the young adult mean, according to the definition of the Japanese Society for Bone and Mineral Metabolism.9
Panoramic radiographs were obtained within the month before the QUS measurement with an AZ-3000 (Asahi, Kyoto, Japan) instrument. Two experienced radiological technologists took these radiographs. A digital radiography system (Regius Model 170; Konica Minolta Holdings, Tokyo, Japan) was used for the radiographs in all subjects. The panoramic radiographs were developed using a laser imager (Drypro SD-P, Konica Minolta Holdings, Tokyo, Japan). All the panoramic radiographs used in this study were satisfactory for taking the measurements. The MCW was measured by an oral radiologist (AT) with 22 years clinical experience.
The MCW was measured bilaterally on the radiographs at the site of the mental foramen, as in our previous study (Figure 1).7 A line was drawn parallel to the long axis of the mandible and tangential to the inferior border of the mandible. A line was constructed perpendicular to this tangent. This line intersected the inferior border of the mental foramen and along this line the MCW was measured using callipers. Mean MCWs of left and right sides of the mandible were used in this study. The coefficient of variation due to positioning and operator error in the cortical width measurement was <2%. 50 randomly selected radiographs were remeasured (by AT) at 2 week intervals between measurements. A second investigator (NS) remeasured these 50 randomly selected radiographs. From this data, the intra and interobserver variations were calculated for the MCW measurement. The intraobserver variation in the cortical width measurement was 0.1 mm, which was similar to the interobserver variation.
Figure 1.
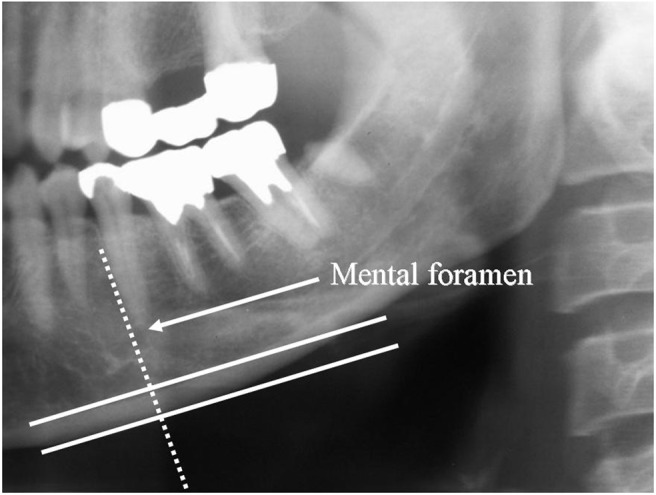
A line was drawn parallel to the long axis of the mandible and tangential to the inferior border of the mandible. A line (dotted line) was constructed perpendicular to this tangent. This line intersected the inferior border of the mental foramen, and along this line mandibular cortical width (the distance between the two parallel solid lines) was measured using callipers
Data analysis
Pearson's correlation coefficient was calculated to evaluate the correlation between age, the MCW and calcaneal BMD measured by QUS. Analysis of covariance (ANCOVA) adjusted for age was used to evaluate the differences in the MCW and calcaneal BMD between men and women. A logistic regression analysis adjusted for age was used to calculate the odds ratios and 95% confidence interval (CI) of having a low calcaneal BMD according to the quartiles of the MCW in men and women.
The areas under the receiver operator characteristic (ROC) curve (AUC) for identifying participants with a low calcaneal BMD using the MCW were measured to evaluate the diagnostic efficacy of the MCW. For the test (low calcaneal BMD or non-low calcaneal BMD) that yielded the MCW (continuous data), the cut-off threshold of the MCW was shifted systematically over the measurement range and the observed pairs of sensitivity 1-specificity were established for each different operating point. Based on these observed pairs, the ROC curve was obtained and the AUC was calculated. According to an arbitrary guideline, we distinguished between non-informative (AUC = 0.5), less accurate (0.5 < AUC < 0.7), moderately accurate (0.7 < AUC < 0.9), highly accurate (0.9 < AUC < 1) and perfect tests (AUC = 1). The data were analysed using the Statistical Package for the Social Sciences (SPSS) v8.0 (SPSS, Chicago, IL). P < 0.05 was considered statistically significant.
Results
Of the participants, 197 (84.2%; 130 men and 67 women) had a normal calcaneal BMD and 37 (15.8%; 28 men and 9 women) had a low calcaneal BMD. In men, age was significantly associated with calcaneal BMD (r = −0.251, P = 0.001), but not with the MCW (r = −0.055, P = 0.492). In contrast, in women, age was not significantly associated with either calcaneal BMD (r = −0.130, P = 0.262) or MCW (r = 0.043, P = 0.709). In all 234 participants, the BMD of the right calcaneus was significantly correlated with the MCW (r = 0.328, P < 0.001). In the 158 men, the calcaneal BMD was significantly correlated with the MCW (r = 0.391, P < 0.001). In the 76 women, the calcaneal BMD was significantly correlated with the MCW (r = 0.260, P < 0.05).
ANCOVA adjusted for age revealed that the MCW tended to be greater in men than in women (4.75 mm vs 4.56 mm, P = 0.094). Women had a greater calcaneal BMD than men (101.6% vs 98.4%) in this study, but the difference was not significant (P = 0.20).
When the MCW in the 158 men was divided into quartiles, the MCWs in the highest (n = 39), second (n = 40), third (n = 40) and lowest quartiles (n = 39) were 7.01 mm – 5.21 mm, 5.20 mm – 4.73 mm, 4.72 mm – 4.14 mm and 4.13 mm – 2.89 mm, respectively. Since the magnification factor is about 1.2 in both genders when we measure inferior cortex of the mandible below the mental foramen, the actual cortical widths in the highest through lowest quartiles were considered to be 5.84 mm – 4.34 mm, 4.33 mm – 3.94 mm, 3.93 mm – 3.45 mm and 3.44 mm – 2.41 mm. The adjusted odds ratios of a low calcaneal BMD associated with the second, third and lowest MCW quartiles were 5.66 (95% confidence interval (CI), 0.61–52.23), 5.43 (95% CI, 0.59–50.18) and 33.22 (95% CI, 3.97–276.94), respectively, compared with the highest quartile (Table 1).
Table 1. Unadjusted and age-adjusted odds ratio and 95% confidence interval of low calcaneal bone mineral density (BMD) according to mandibular cortical width in adult men aged 40 years or younger.
| Unadjusted (range) | Age-adjusted (range) | |
| Highest quartile | 1 | 1 |
| Second quartile | 5.73 (0.64–51.51) | 5.66 (0.61–52.23) |
| Third quartile | 5.57 (0.62–49.99) | 5.43 (0.59–50.18) |
| Lowest quartile | 30.13 (3.75–241.89) | 33.22 (3.97–276.94) |
When the MCW in the 76 women was divided into quartiles, the MCWs in the highest through lowest quartiles were 6.50 mm – 5.19 mm, 5.18 mm – 4.60 mm, 4.59 mm – 3.88 mm and 3.87 mm – 2.98 mm, respectively. However, no significant trend in the adjusted odds ratios was observed in women. A logistic regression analysis revealed that the MCW was not a significant predictor of low calcaneal BMD in women.
In all participants, the AUC for identifying participants with low calcaneal BMD based on the MCW was 0.745 (95% CI, 0.658–0.832), implying that the diagnostic efficacy of the MCW is moderate. However, it was 0.796 (95% CI, 0.702–0.890) in men and 0.593 (95% CI, 0.398–0.788) in women (Figure 2), suggesting that the MCW is a useful screening tool for low calcaneal BMD in men but not in women.
Figure 2.

The receiver operator characteristic curve for identifying participants with a low calcaneal bone mineral density by mandibular cortical width in men (A) and women (B)
Discussion
This study is the first to demonstrate an association between the MCW and general skeletal BMD in men and women aged 40 years or younger. We found that adult men aged 40 years or younger with an undetected low calcaneal BMD could be identified by the MCW measured on panoramic radiographs, while young adult women with an undetected low calcaneal BMD could not be detected. These findings are inconsistent with the results of many studies of triage screening for osteoporosis in elderly men and women.6 The simple correlation coefficient between the heel BMD measured using QUS and the MCW was 0.394 (P < 0.001) in 262 Japanese men aged 80 years.10 This result is similar to that of our current study. In contrast, a moderate correlation (r = 0.471, P < 0.001) was found in 397 Japanese women aged 80 years. Similar correlations (r = 0.4–0.5) between the skeletal BMD measured using QUS or dual energy X-ray absorptiometry (DXA) and MCW were observed in elderly individuals, especially post-menopausal women in previous studies.6 Our result for young adult women and previous results for post-menopausal women suggest that the correlation between MCW and skeletal BMD increases in the post-menopausal period owing to the rapid decrease in both the MCW and skeletal BMD after menopause. In fact, a rapid decline in the MCW was observed after the age of 50,7 which is the mean age at which menopause occurs worldwide.
The MCW increases rapidly in the second decade in women, while it increases gradually from the second to third decades in men.7 Since occlusal function due to the permanent teeth is established during the second decade, this might affect the formation of the cortical bone of the mandible locally and individually. The maturation of the entire skeleton in young adult women, including the jaws, is influenced by several factors, such as the age of menarche, menstruation cycle, nutritional intake and physical activity.11 Trabecular bone, which comprises most of the calcaneus, is sensitive to these factors, which may be why the correlation between the MCW and calcaneal BMD was relatively low in the young adult women (22.9 ± 3.3 years) in our study. In post-menopausal women, menopause is the major factor contributing to the rapid decrease in the BMD of the skeleton, including the jaws. A rapid decrease in the number of remaining teeth is observed in post-menopausal women, regardless of good oral care, compared with men.12 As some studies have reported, dentition status may influence the MCW.13,14 However, further adjustment for the number of teeth remaining did not change the odds ratios of having low spine BMD or spinal osteoporosis estimated using DXA among the MCW quartiles in our recent study.15 This suggests that tooth loss does not contribute greatly to the decrease in the MCW in post-menopausal women.
In this study, we used the calcaneal BMD, measured using QUS, as a representative of general skeletal status, although DXA measurement is considered the gold standard for determining osteoporosis status. However, QUS of the calcaneus was reported to be a better predictor of osteoporotic fractures than DXA.16 Also, the predictive value of QUS measurements of the calcaneus for vertebral fractures was significantly higher than that of DXA of the spine and hip, even after adjusting for confounding variables, in a recent study.17 Given the many similar reports on the diagnostic efficacy of QUS of the calcaneus for predicting osteoporotic fractures, we used this method rather than DXA in this study.
Although most patients with osteoporosis are elderly women, osteoporosis in men is becoming an increasingly important public health problem. Men who sustain fractures have an increased mortality risk. The cumulative mortality at 12 months among hip-fracture patients compared with the general population was 37.1% (9.9%) in men and 26.4% (9.3%) in women for all Danish patients (more than 41 000 people) with hip fractures.2 Being male and having a trochanteric fracture were risk factors for death in 480 Japanese men and women with hip fractures.18 In this study, we showed that it may be possible to identify adult men aged 40 years or younger who are at risk of having low skeletal BMD by using the MCW determined from panoramic radiographs. If we identify such men in dental clinics and refer them to medical professionals for further investigation and lifestyle intervention, the mortality related to osteoporotic fractures in men could be greatly reduced. Conversely, our results indicate that women aged 40 years or younger at risk of having a low skeletal BMD cannot be identified.
Women had a greater calcaneal SOS than men in this study, but the difference was not significant. This result concurs with that of a previous study in which the SOS at the calcaneus measured using QUS was similar in males and females in 632 healthy adolescents (321 males and 311 females) aged 12–17 years recruited from a larger cohort study (the Japanese Population-based Osteoporosis Study (JPOS)), although men were significantly taller, heavier and had a higher BMD of the radius than women, according to DXA.19 In their study, no association was observed among the SOS at the calcaneus, age and body size. The QUS index reflects not only bone density but also bone quality, so no significant difference may be found in the SOS at the calcaneus between men and women.
In triage screening for osteoporosis, both cortical width and shape detected on panoramic radiographs have been applied to identify individuals, especially post-menopausal women, with undetected low skeletal BMD or osteoporosis. Several cortical indices, including cortical shape (erosion), were evaluated in 500 British females aged 25–74 years and a class 3 cortex (a severely eroded cortex) was found in women aged 35 and 39 years in a previous study.8 A “trabecular tail from the cortex” may have been misdiagnosed as class 36 or these women may have had amenorrhoea or other lesions affecting bone metabolism. Furthermore, a class 2 cortex (a mildly to moderately eroded cortex) appeared in women aged 25–29 years and many more subjects had class 2 than class 1 (normal cortex) between the ages of 25 and 44 years. This finding is curious, because class 2 indicates increased bone resorption around the Haversian canals in the cortex of the mandible. Usually, the BMD of the general skeleton declines rapidly in the peri- and post-menopausal periods; the authors may have misdiagnosed class 1 as class 2. A “trabecular tail from the cortex” seems to be a typical pattern in which class 1 is misdiagnosed as class 2. Since no worldwide consensus exists on reading cortical shape, we used only cortical width in our study.
Our study has some limitations. First, we did not evaluate the occlusal function of the participants, although students who had undergone orthodontic treatment were excluded. The possibility exists that occlusal function influences the association between the MCW and calcaneal BMD. In fact, we found that the MCW in men tended to be greater than that in women. Adjusting for occlusal function might influence the results. The second limitation is the effect of lifestyle, including dietary intake and exercise. Since our participants were students at the School of Dentistry and School of Dental Hygiene, they represent a relatively homogeneous population in terms of lifestyle. However, mechanical stress due to habitual exercise may strongly influence the calcaneal BMD. Third, the mean age of both the men and the women was relatively young (24.3 ± 3.7 years and 22.9 ± 3.3 years, respectively). Inclusion of more adults aged 30–40 years might have altered the results. Fourth, relatively few female participants were enrolled in this study. A small sample size (three volunteers) for the determination of intra and interobserver reliabilities for ultrasonography may also limit our results. Further study, including more participants and information about contributing factors, such as dietary intake and exercise, is necessary to clarify our results.
In conclusion, the diagnostic efficacy of the MCW in identifying low calcaneal BMD was sufficient for triage screening in adult men aged 40 years or younger, but was insufficient in women aged 40 years or younger. Our results suggest that undetected low calcaneus BMD can be identified in young adult men by using MCW derived from panoramic radiographs in order to refer them to medical professionals for further investigation; however, undetected low calcaneus BMD in young adult women cannot be identified in this way.
Acknowledgments
This work was supported in part by a grant-in-aid from the Japan Society for the Promotion of Science (No. 21592404) and Matsumoto Dental University Research Foundation Grant 2008.
References
- 1.Muraki S, Yoshimura N. Incidence of and prognosis for osteoporotic fracture. Clin Calcium 2006;16:1431–1437 (in Japanese) [PubMed] [Google Scholar]
- 2.Kannegaard PN, van der Mark S, Eiken P, Abrahamsen B. Excess mortality in men compared with women following a hip fracture. National analysis of comedications, comorbidity and survival. Age Ageing 2010;39:203–209 [DOI] [PubMed] [Google Scholar]
- 3.Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB. Incidence and mortality of hip fractures in the United States. JAMA 2009;14:1573–1579 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Marx RE. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: a growing epidemic. J Oral Maxillofac Surg 2003;61:1115–1117 [DOI] [PubMed] [Google Scholar]
- 5.Yoneda T, Hagino H, Sugimoto T, Orha H, Takahashi S, Soen S, et al. Bisphosphonate-related osteonecrosis of the jaw: position paper from the Allied Task Force Committee of Japanese Society for Bone and Mineral Research, Osteoporosis Society Japan, Japanese Society of Periodontology, Japanese Society for Oral and Maxillofacial Radiology and Japanese Society of Oral and Maxillofacial Surgeons. J Bone Miner Metab 2010;28:365–383 [DOI] [PubMed] [Google Scholar]
- 6.Taguchi A. Triage screening for osteoporosis in dental clinics using panoramic radiographs. Oral Dis 2009. 2010;16:316–327 [DOI] [PubMed] [Google Scholar]
- 7.Taguchi A, Tanimoto K, Suei Y, Wada T. Tooth loss and mandibular osteopenia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995;79:127–132 [DOI] [PubMed] [Google Scholar]
- 8.Ledgerton D, Horner K, Devlin H, Worthington H. Radiomorphometric indices of the mandible in a British female population. Dentomaxillofac Radiol 1999;28:173–181 [DOI] [PubMed] [Google Scholar]
- 9.Yamamoto K. Definition and diagnostic criteria of osteoporosis in Japan. Clin Calcium 2001;11:19–24 (in Japanese) [PubMed] [Google Scholar]
- 10.Okabe S, Morimoto Y, Ansai T, Yoshioka I, Tanaka T, Taguchi A, et al. Assessment of the relationship between the mandibular cortex on panoramic radiographs and the risk of bone fracture and vascular disease in 80-year-olds. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;106:433–442 [DOI] [PubMed] [Google Scholar]
- 11.Borer KT. Physical activity in the prevention and amelioration of osteoporosis in women: interaction of mechanical, hormonal and dietary factors. Sports Med 2005;35:779–830 [DOI] [PubMed] [Google Scholar]
- 12.Meisel P, Reifenberger J, Haase R, Nauck M, Bandt C, Kocher T. Women are periodontally healthier than men, but why don't they have more teeth than men? Menopause 2008;15:270–275 [DOI] [PubMed] [Google Scholar]
- 13.Dutra V, Yang J, Devlin H, Susin C. Radiomorphometric indices and their relation to gender, age, and dental status. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;99:479–484 [DOI] [PubMed] [Google Scholar]
- 14.Gulsahi A, Yüzügüllü B, Imirzalioglu P, Genç Y. Assessment of panoramic radiomorphometric indices in Turkish patients of different age groups, gender and dental status. Dentomaxillofac Radiol 2008;37:288–292 [DOI] [PubMed] [Google Scholar]
- 15.Taguchi A, Ohtsuka M, Tsuda M, Nakamoto T, Kodama I, Inagaki K, et al. Risk of vertebral osteoporosis in post-menopausal women with alterations of the mandible. Dentomaxillofac Radiol 2007;36:143–148 [DOI] [PubMed] [Google Scholar]
- 16.Stewart A, Kumar V, Reid DM. Long-term fracture prediction by DXA and QUS: a 10-year prospective study. J Bone Miner Res 2006;21:413–418 [DOI] [PubMed] [Google Scholar]
- 17.Hollaender R, Hartl F, Krieg MA, Tyndall A, Geuckel C, Buitrago-Tellez C, et al. Prospective evaluation of risk of vertebral fractures using quantitative ultrasonography measurements and bone mineral density in a population-based sample of postmenopausal women: results of the Basel Osteoporosis Study. Ann Rheum Dis 2009;68:391–396 [DOI] [PubMed] [Google Scholar]
- 18.Muraki S, Yamamoto S, Ishibashi H, Nakamura K. Factors associated with mortality following hip fracture in Japan. J Bone Miner Metab 2006;24:100–104 [DOI] [PubMed] [Google Scholar]
- 19.Ikeda Y, Iki M, Morita A, Aihara H, Kagamimori S, Kagawa Y, et al. Ultrasonography bone densitometry of the calcaneus, determined with Sahara, in healthy Japanese adolescents: Japanese Population-based Osteoporosis (JPOS) Study. J Bone Miner Metab 2004;22:248–253 [DOI] [PubMed] [Google Scholar]