

Abstract
The aim of this study was to determine the clinical effect of Foeniculum vulgare on primary dysmenorrhoea. Sixty virgin girls with complaints of dysmenorrhoea were enrolled in this study, out of which 50 cases were completed the course of treatment and were divided in two groups (study and placebo) and were under treatment for two cycles. In study group a capsule of 30 mg fennel extract, four times a day for three days from start of their menstrual period and in placebo a capsule containing wheat flour in same dose was administered. Intensity of pain was reported by using a 10 - point linear analogue technique. In study group the mean age of menarche was 13.1 ± 0.1 and onset age of dysmenorrhoea was 14.5 ± 0.1 years. Both groups were relieved but there was significant difference between study and placebo group. Study group shown more effective results than placebo in pain relief (P`0.05). Based on the observations, it can be concluded that, fennel is an effective herbal drug for menstrual pain.
Keywords: Fennel, Foeniculum vulgare, pain, primary dysmenorrhoea
Introduction
Primary dysmenorrhoea is the most common gynaecological problem in menstruating women and the prevalence rate is up to 90% and is one of the most important causes of workplace absenteeism and decreasing quality of life among women.[1] It is found that about 13% to 51% women are absent at least once and 5% to 14% are often absent owing to the severity of symptoms.[2] About one in ten women are unable to perform their normal routine for 1-3 days of each menstrual cycle due to severe uterine cramping.[3] Dysmenorrhoea accounts for an annual loss of 600 million work hours and US $2 billion dollars in productivity.[4] Therefore, treatment of this pain is an important issue.
Primary dysmenorrhoea is treated with drugs such as, the non-steroidal anti-inflammatory agents including Mefenamic Acid, Ibuprofen that inhibit prostaglandin metabolism or with oral contraceptives to prevent ovulation or hormonal drugs.[5, 6] Accupressure and acupuncture,[4, 7] beta-blockers, regular physical exercise, Transcutaneous electrical nerve stimulation, presacral neurotomy and hysterectomy, etc. are certain other methods which may be helpful in relieving the signs and symptoms of the condition.[5, 8, 9]
Few studies have shown the effectiveness of herbal drugs in the treatment of dysmenorrhoea,[10-12] which highlighted the role of nutritional and metabolic factors as an important role in triggering menstrual problems and their treatment.[12] The effectiveness of herbal and dietary treatment is still under investigation and needs more careful studies.
In United States, herbal drugs were formally introduced in 1994.[12] In recent past, an increased momentum has been noticed towards utilization of herbal drugs in many disease conditions because of unfolded causes, possibility developing of adverse drug reactions of chemical drugs is one among them.[13] One of the suggested herbal drugs is fennel. Fennel is cultivated in many parts of Europe and Asia and much is imported from India, China and Egypt.[14] The essence of fruits of a grassy, fragrant plant known as Foeniculum vulgare variety dulce (fennel) from Apiaceae (Umbelliferae) family, has been used in the Mediterranean area to relieve painful menstruation for many years.[15] In one study fennel has shown anti-spasmodic effect on the isolated uterine of mouse.[16] In traditional medicine of Iran, some effects have been stated for fennel such as, anti bulging, galactagogue,[17, 18] anti-spasmodic etc.[19, 20]
Considering the significance of these properties; an attempt has been made to evaluate clinical efficacy of F. vulgare in primary dysmenorrhoea.
Materials and Methods
Study design
It is a Placebo controlled double blind clinical study. Virgin patients of 15-24 years age with moderate or severe dysmenorrhoea were considered for the study. Total 60 patients were screened, out of them 10 cases were excluded from the study due to evidences of other reasons like secondary/mild dysmenorrhoea, receiving other drugs, pre-existing diagnosed disease and history of hypersensitivity. Remaining 50 patients were enrolled and randomly divided into two groups. Each group administered with respective medicament for four times a day for three days from the first day of menstrual period. In the first group (Study group), patients received capsules containing 30mg fennel extract. The second group (Placebo group) received capsules containing wheat flour. The drugs were administered for two consecutive menstrual cycles. Each subject recorded pain intensity before using the drug, five consecutive hours after drug administration and at the end of the day.
Foeniculum vulgare essence was produced by distillation of fennel seeds with water vapour (Barij Essence Co, Iran produced drug and placebo) and was converted into pearl shape (30 mg). In order to isotropy each pearl was placed inside a capsule and was coded (by the Pharmacology laboratory in Babol Medical Sciences University).
Data collection instrument included a questionnaire with three parts:
Demographic characteristics
Medical and menstrual history
Pain intensity assessment scale
The validity of the questionnaire was assessed by content validation and for assessment of pain intensity, by using a visual scale, a 10cm line (0 -10 defined as no pain to intense pain). This scale is a standard scale.
Ethics and consent
The study protocol was approved by the Ethics Committee of Babol Medical Sciences University. Written informed Consents of subjects were obtained.
Statistical analysis
Statistical analyses were performed with the use of paired-t test. Values were expressed as mean±S.D. P values`0.05 were considered significant.
Results
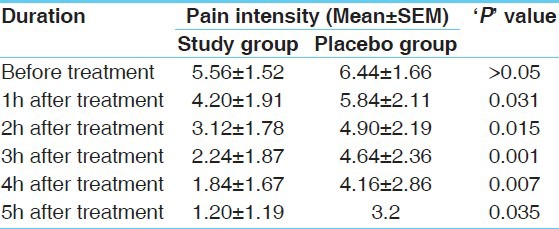
Two groups were matched for age (22±0.5), age of menarche (13.1±0.1) and onset age dysmenorrhoea (14.5±0.1). Mean duration of menstruation was 6.2±0.1 days with the mean cycle length of 28.6±0.4 days. There was no significant difference of period mean duration, mean amount of blood loss and mean pain intensity in between two groups (Pb0.05). This study shows reduced pain intensity in both the groups. Statistically significant (P`0.05) differences was found during 5 h after drug administration in both groups [Table 1].
Table 1.
Effect of therapies on mean intensity of pain in first 5 hours after treatment
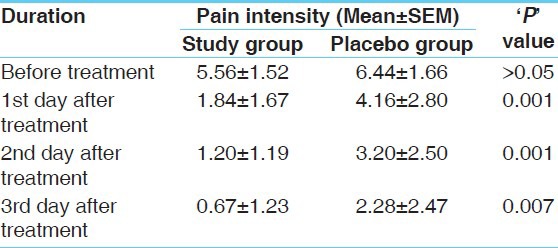
In order to evaluate the effect of fennel, the mean pain intensity of the two groups were compared day by day for first three days of menstruation for two cycles [Table 2]. There were significant differences (P`0.01) between the two groups during the first three days of the cycles.
Table 2.
Effect of therapies on mean intensity of pain in 3 days after treatment
52% of registered patients in study group stated the treatment as excellent, 20% reported as moderate and 28% as slight or no effect on pain. But in placebo group 8% reported excellent effect, 48% moderate and 44% stated the treatment has a slight or no effect.
Discussion
In this study the duration of menstruation among 70.5% of subjects was 6 days and menarche age among 63.5% were 13 years or before that. Some studies showed that the onset of menstruation in lower age and longer duration of menstrual period are risk factors for the severity of dysmenorrhoea.[12, 16]
Few studies suggest the efficacy of fennel in primary dysmenorrhoea with comparison to placebo.[21] Complete relief of pain was reported by 80% of the participants in another study by the administration of fennel and 73% of participants reported complete pain relief by Mefenamic acid in dysmenorrhoea.[22] Researches studied an effect of fennel on rat uterine contractions, demonstrated that FEO can inhibit contraction of isolated uterus that was induced by Oxytocin and PGE2.[16] Based on these conclusions, it can be assumed that, inhibition of contractions leads to pain relief in dysmenorrhoea. In addition, study on effect of fennel on colicky pain among infants suggests that fennel seed oil emulsion is superior to placebo in decreasing intensity of infantile colic.[19]
Although, some studies mentioned that fennel extract contains small amounts of Coumarins that could affect coagulation and bleeding,[23] no significant difference was observed in current study, in both groups. Results of the study are similar to the earlier work done in 1999.[21]
Conclusion
Available evidences suggests that, the common management is based on pharmacological preparations, where in 10-20% of women do not respond to this course of management. On the other hand use of herbs and other natural products are increasingly preferred. Regarding the effectiveness of fennel, it can be used to relieve the signs and symptoms significantly on primary dysmenorrhoea.
Acknowledgments
Authors are thankful to Barij Essence Co. Ltd, Iran for providing the fennel essential oil and research area of the University of Babol Medical Sciences for their financial support for this project.
References
- 1.Jamieson DJ, Stegge JF. The prevalence of dysmenorrhea, dyspareunia, pelvic pain and irritable bowel syndrome in primary care practices. Obstet Gynecol. 1996;87:55–8. doi: 10.1016/0029-7844(95)00360-6. [DOI] [PubMed] [Google Scholar]
- 2.Weissman AM, Hartz AJ, Hansen MD, Johnson SR. The natural history of primary dysmenorrhea: A longitudinal study. Br J Obstet Gynecol. 2004;111:345–52. doi: 10.1111/j.1471-0528.2004.00090.x. [DOI] [PubMed] [Google Scholar]
- 3.Marjoribanks J, Proctor ML, Farquhar C. Nonsteroidal anti-inflammmatory drugs for primary dysmenorrhea. Cochrane Database Syst Rev. 2003;4:CD001751. doi: 10.1002/14651858.CD001751. [DOI] [PubMed] [Google Scholar]
- 4.Tayler D, Miaskowski C, Kohn J. A randomized clinical trial of the effectiveness of an acupressure device for managing symptoms of dysmenorrhea. J Altern Complement Med. 2002;8:357–70. doi: 10.1089/10755530260128050. [DOI] [PubMed] [Google Scholar]
- 5.Berek JS. 13th ed. Philadelphia: Lippincott Williams and Wilkins; 2002. Novak’s Text book of Gynecology. [Google Scholar]
- 6.Ryan KJ, Barbieri RL, Berkowitz RS, Dunaif AE. 7th edition 1999. Kistner’s Gynecology and Women’s Health. [Google Scholar]
- 7.Helms J. Acupuncture for the management for primary dysmenorrhea. Obstet Gynecol. 1987;69:61. [PubMed] [Google Scholar]
- 8.Speroff L, Glass RH, Kase NG. 6th ed. Philadelphia: Lippincott Williams and Willkins; 1999. Clinical Gynecology Endocrinology and Infertility; pp. 557–75. [Google Scholar]
- 9.Scott JR, DiSaia PJ, Hammond CB, Spellacy WN. 8th ed. Philadelphia: Lippincott Williams and Wilkins; 1999. Danforth’s Obstetircs and gynecology. [Google Scholar]
- 10.Diyanati B, Momeni T. Tehran: Shahrashoob Press; 2001. Adverse effects of medical plants; pp. 84–94. [Google Scholar]
- 11.Shibata T, Morimoto T, Suzuki A, Saito H, Yanaihara T. The effect of shakuyukukenzo-to on prostaglandin in human urterine myometrium. Nippon Sanka Fujinka Zasshi. 1996;48:321–7. [PubMed] [Google Scholar]
- 12.Wilson ML, Murphy PA. Herbal and dietary therapies for primary and secondary dysmenorrhea. Cochrane Database Syst Rev. 2001;3:CDOO2124. doi: 10.1002/14651858.CD002124. [DOI] [PubMed] [Google Scholar]
- 13.Rojhan MS. Tehran: Khayyam Press; 1994. Cure with medicinal plants; pp. 110–3. [Google Scholar]
- 14.Evans WC. Edinburgh: W.B. Saunders; 2002. Trease and Evans Pharmacognosy; p. 264. [Google Scholar]
- 15.Zargari A. Tehran: Tehran University Publication; 1991. Medicinal plants; pp. 32–7. [Google Scholar]
- 16.Ostad SN, Soodi M, Shariffzadeh M, Khorshidi N, Marzban H. The effect of fennel essential oil on uterine contraction as a model for dysmenorrhea, pharmacology and toxicology study. J Ethnopharmacol. 2001;76:299–344. doi: 10.1016/s0378-8741(01)00249-5. [DOI] [PubMed] [Google Scholar]
- 17.Parfitt K. London: Pharmaceutical Press; 1999. Martindale-the complete drug reference; p. 1579. [Google Scholar]
- 18.Ody P. London: Dorling Kindersley; 1995. The Herb Society’s home herbal; p. 37. [Google Scholar]
- 19.Alexandrovich I, Rakovitskaya O, Kolmo E, Sidorova T, Shushunov S. The effect of fennel (Foeniculum Vulgare) seed oil emulsion in infantile colic: A randomized, placebo-controlled study. Altern Ther Health Med. 2003;9:58–61. [PubMed] [Google Scholar]
- 20.Crotteau CA, Wright ST, Eglash A. Clinical Enquiries.What is the best treatment for infants with colic? J Fam Pract. 2006;55:634–6. [PubMed] [Google Scholar]
- 21.Soodi M. Tehran: Tehran Medical Sciences University; 1999. Clinical studies on the effect of fennel in the treatment of dysmenorrhea [dissertation] [Google Scholar]
- 22.Modaress Nejad V, Asadipour M. Comparison of the effectiveness of fennel and mefenamic acid on pain intensity in dysmenorrhoea. East Mediterr Health J. 2006;12:423–7. [PubMed] [Google Scholar]
- 23.Ostad SN, Shariffzadeh M, Soodi M. Evaluation of toxicity of foeniculum vulgare variety dulce and its LD50. Barij Essence Pamphlet. 2000;1:24–6. [Google Scholar]