

Abstract
Aging has become one of the distinctive demographic phenomena in the 21st century and its social, economic and health implications are the most challenging issues. Senile Memory Impairment is a common condition characterized by mild symptoms of cognitive decline and occurs as a part of the normal aging process. It can be correlated to “Jarajanya Smrtibhramsha” according to Ayurveda. The present study deals with the efficacy of Guduchyadi Medhya Rasayana on Senile Memory Impairment. A total of 138 patients aged in between 55–75 years were registered and randomly divided into two groups as the trial and control groups. The drugs were administered for 3. The trial drug showed memory enhancement, anti-stress, anti-depressant and anxiolytic properties. The trial group showed better results in the management compared to the control group.
Keywords: Aging, Guduchyadi Medhya Rasayana, Senile Memory Impairment
Introduction
Aging has become a great issue for many countries due to a worldwide life prolongation. Number of people over 60 years has grown rapidly to 10% of the world population.[1] In India too, in the last decade, increasing population aged has been projected significantly.[2] So, it is associated with physiological, functional, and pathological changes affecting physical, psychological, emotional and social well-being.[3] The major consequences of the increasing number of individuals in advanced age group is the increase in number of patients suffering from age-related disorders. Conservative estimation revealed that 25% of the elderly persons have significant psychiatric symptoms[4] and the number of psychologicaly ill elderly persons was estimated to be 9 million in the year 2005.[5] Though psychological disorders are common among the aged, it frequently remains undetected and untreated. It induces functional disability, disturbs rehabilitation, burdens the health system and impairs the quality of life of elderly individuals.[6] Research based on the psychological health revealed that age-associated cognitive like memory disorders are found in high prevalence among the aged.[7] Subjective complaints from individuals with age-associated memory impairment often include difficulties in remembering names and words, etc. So, this condition is the result of physiological changes in the aging brain and not a specific neurological disorder.[8] In Ayurveda literature, impairment of memory is mentioned as Smritibhramsha which occurs due to vitiation of Rajas and Tamas Doshas in the mind.[9] The appearance of Jara (aging) at the appropriate age is termed as “Kalaja Jara”,[10] and memory impairment appears as a clinical Rupa (feature) of Jara,[11] hence Senile Memory Impairment can be correlated as Jarajanya Smritibhramsha according to Ayurveda.
In Sarangadhara Samhita, it is clearly emphasized that Medha (intellect) and Buddhi (wisdom) deteriorate in the fourth and ninth decades of life accordingly.[12] Both are closely associated with the mind and help for the normal function of the mind. If these components decrease in the mind, then it will affect the normal function of mind.
Moreover, Caraka has noted that cognitive functions are thoroughly affected in old age as Grahana (power of understanding), Dharana (power of retention), Smarana (power of memorizing), Vachana (speech) and functions of sense organs qualitatively.[13]
Importance of Medhya Rasayana on aging
The aging process occurs over all the body. It does not occur in the same way in every human being. People’s lifestyles also have additional influence on aging.[14] The decline in brain weight and volume, degeneration of intracellular organelles, changes in cellular DNA and RNA, neuronal degeneration as well as significant loss of synapses are the salient features of aging in the brain.[15] Therefore, psychological and neurological manifestations often form the hallmark of senility. Hence, Ayurveda clearly emphasizes that in the fourth and ninth decades of lifespan, individuals are subjected to the loss of Medha (intellect) and Buddhi (wisdom). Hence, it seems therapeutic measures of Medhya Rasayanas are exclusively needed for elders because they are brain tonics and improve the psychological faculties. It is responsible for Dhi (intelligence), Dhrti (retention power), Smriti (memory) and also possesses anti-stress and adaptogenic effect.[16]
Having considered all literary views and ideas as above mentioned, Guduchyadi Medhya Rasayana (GMR)[17] has been attempted to evaluate its efficacy on Senile Memory Impairment.
Materials and Methods
Selection of the patients
Total 138 patients having symptoms of memory impairment attending O.P.D. and I.P.D. of Department of Kaya Chikitsa of I.P.G.T. and R.A., Gujarat Ayurved University, Jamnagar were selected for the present study. A purposive sampling technique was adopted irrespective of their sex, religion, occupation, educational status, etc.
Criteria of inclusion
Patients aged 55 and above up to75 years of age.
- Complaints of memory impairment on the basis of short term and long term.
- Short term, e.g. misplacing objects, difficulty in remembering multiple items to be purchased, difficulty in recalling information quickly, problems in remembering names and telephone numbers.
- Long term, e.g. difficulty in recall of special events of personal life, difficulty in recall of previous histories of life and recognition.
Patients suffering from dementia.
Criteria of exclusion
Patients below 55 years and above 75 years of age.
Patients with evidence of delirium, confusion or other disturbances of consciousness, Parkinson’s disease, stroke, intracranial hemorrhage, brain tumors, history of alcoholism or drug dependence, use of any psychotropic drug, Alzheimer’s disease, diabetes mellitus, etc.
Investigations
Routine hematological and biochemical tests were carried out before and after the treatment. Among the biochemical tests, serum Acetylcholine Esterase (AChE) estimation, as a biomarker of Senile Memory Impairment, was carried out.
Plan of the study
Patients fulfilling the inclusion criterion were grouped in to two after obtaining written consent.
Group A (Trial Group)
Patients of this group were administered with the Granules of Guduchyadi Medhya Rasayana (GMR), which contains Guduchi (Tinospora cordifolia Wild.), Apamarga (Achyranthes aspera Linn.), Vidanga (Embelia ribes Burm. f.), Shankhapushpi (Convolvulus pluricaulis Chois.), Vaca (Acorus calamus Linn.), Haritaki (Terminalia chebula Zetz.), Kushtha (Saussurea lappa C.B. Clarke), Shatavari (Asparagus racemosus Wild.), Cow’s ghee and sugar.
Dosage: 5 g, 3 times per day, after meal
Anupana: Water in sufficient quantity
Duration: 3 months
Total, 73 patients were registered.
Group B (Control Group)
Patients of this group were administered Sarkaradi Granules (SG).
Dosage: 3 g, 3 times per day, after meal
Anupana: Water in sufficient quantity
Duration: 3 months
Total 65 patients were registered..
Both the drugs were prepared at Pharmacy, Gujarat Ayurved University, Jamnagar.
Criteria of assessment
Effects of Medhya Rasayana on memory impairment were assessed in two ways, i.e. as subjective and objective, before and after the treatment.
After completion of the treatment, the patients were graded into five groups based on their improvement in order to ascertain the overall therapeutic efficacy. The data so obtained were analyzed using SPSS and Sigma Stat statistical packages. Observations and results pertaining to clinical parameters were presented in tabular form along with the findings of statistical analysis. Paired “t” test was adopted to find out the effect of therapy for each group individually, while unpaired “t” test used for comparative effect.
Subjective criteria
Assessments on improvements in signs and symptoms were carried out using appropriately designed scoring method, with the scores ranging from 0 to 4. Cognitive state was assessed by Mini Mental State Examination.[18] and psychological health of the patients was evaluated with Hamilton Rating Scales for Depression and Anxiety.[19]
Objective criteria
Serum AChE estimation was carried out as a biomarker of Senile Memory Impairment.
Observations and Results
Total 138 patients of Senile Memory Impairment were registered in the study. Forty-three patients in the Group A (trial group) and 56 patients in the Group B (control group) completed the treatment, while 30 patients in Group A and 9 patients in Group B discontinued. In this study, various etiological factors were identified. Maximum number of patients reported Chinta (thoughts; 92%), followed by Krodha (anger; 83.3%), Shoka (worries; 70.2%), Chittodvega (anxiety; 64.4%), Bhaya (fear; 51.4%), Ruksha Ahara (dried food; 55.7%), Rattri Jagarana (awaking at night; 87%), etc.
Effect of therapy
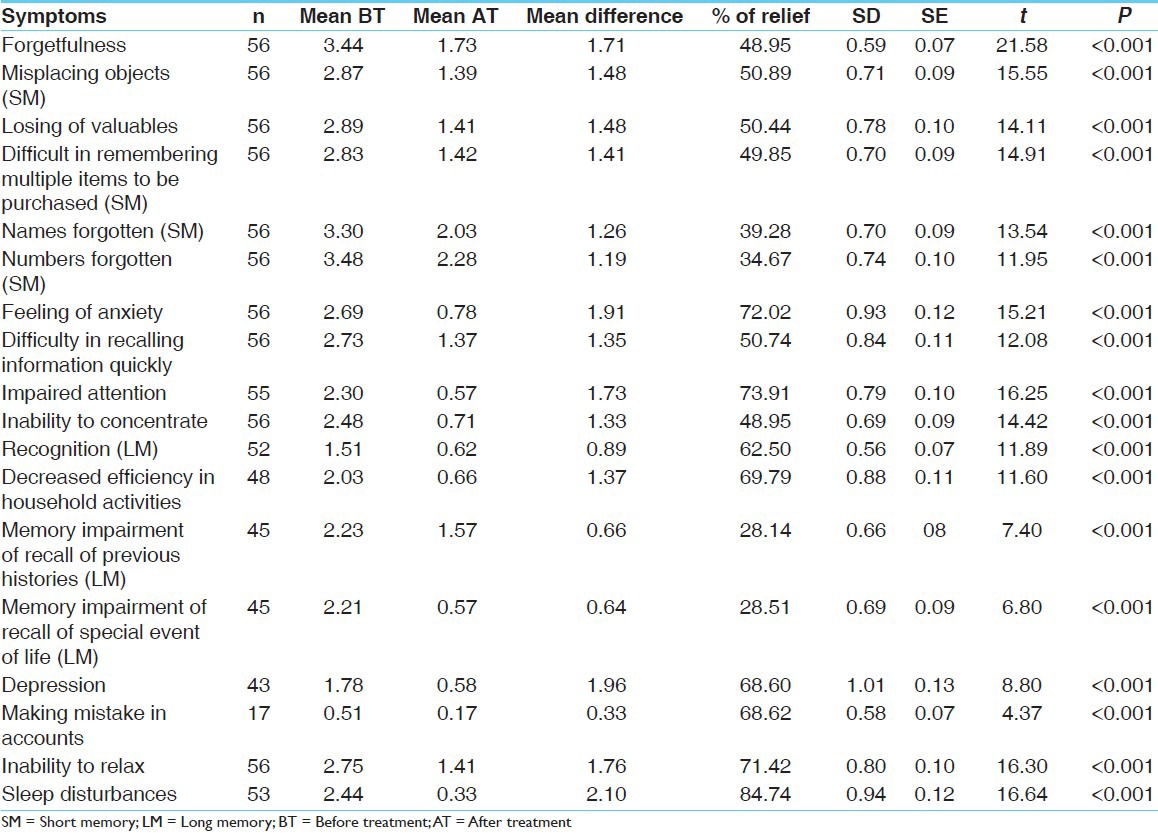
Both the groups showed highly significant (P`0.001) relief from all the chief complaints [Table 1 and Table 2].
Table 1.
Effect of GMR in Group A on the symptoms of Senile Memory Impairment
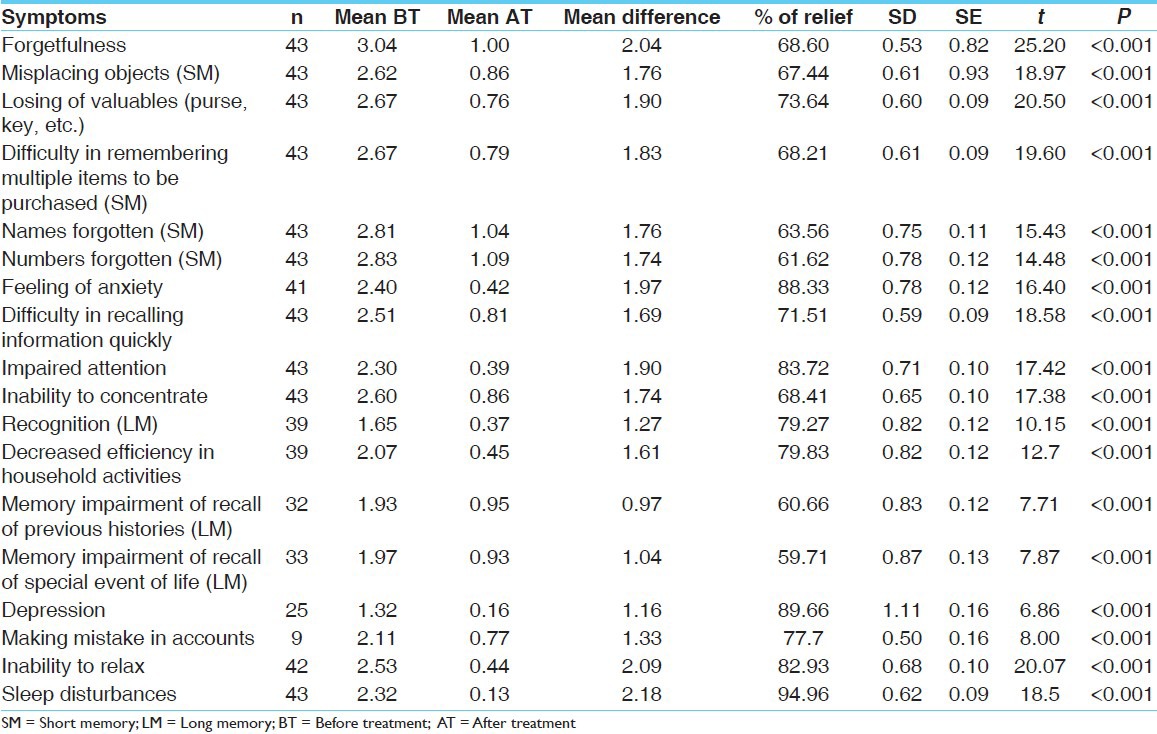
Table 2.
Effect of SG in Group B on the symptoms of Senile Memory Impairment
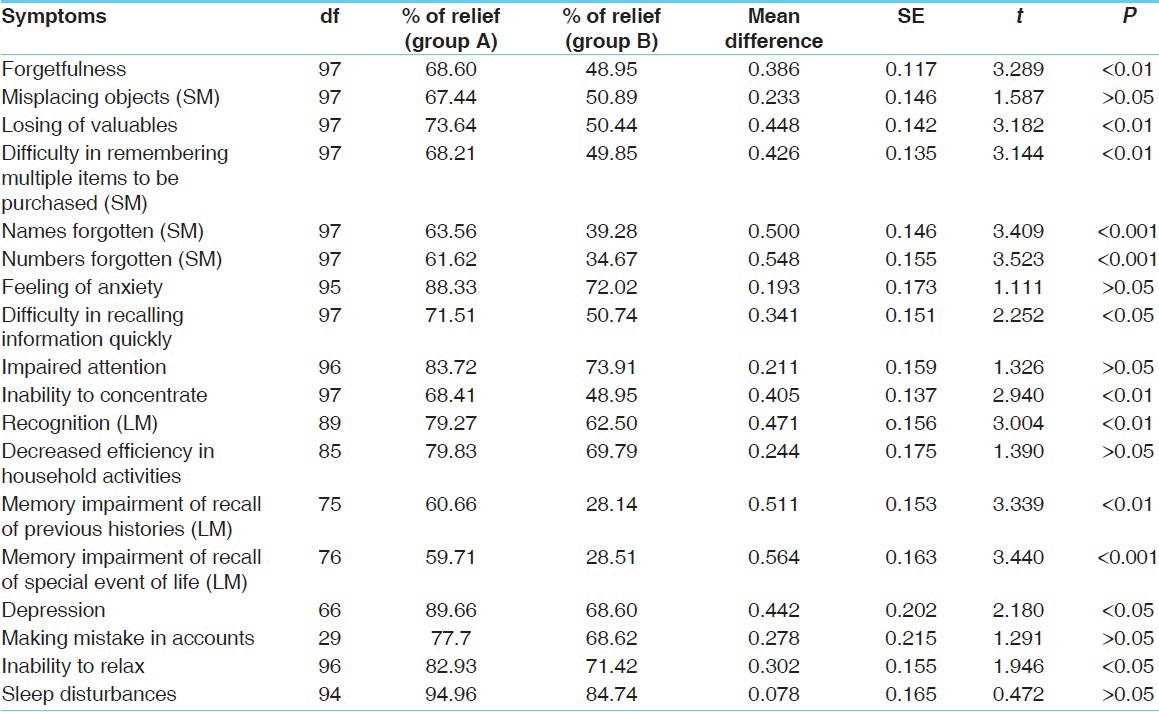
In comparison to Group B, Group A showed highly significant relief in symptoms such as names forgotten (63.56%), numbers forgotten (61.62%), and memory impairment in recalling special events in life (59.71%) at a level of P`0.001, and forgetfulness (68.60%), losing of valuables (73.64%), difficulty in remembering multiple items to be purchased (68.21%), inability to concentrate (68.14%), impaired recognition (79.7%), memory impairment of recall of previous histories (60.66%) at a level of P`0.01, and a significant relief (P`0.05) from difficulty in recalling information quickly (71.57%), depression (89.66%), and inability to relax (82.93%) [Table 3].
Table 3.
Comparison of the effects of GMR and SG on the symptoms of Senile Memory Impairment
With respect to Dosha Dushti, the Group A showed significant relief from Vata Dushti (85.48%), Pitta Dushti (94.15%) and in Kapha Dushti (84.3%), while the Group B showed significant relief from Vata Dushti (68.3%), Pitta Dushti (61.78%) and in Kapha Dushti (62.75%).
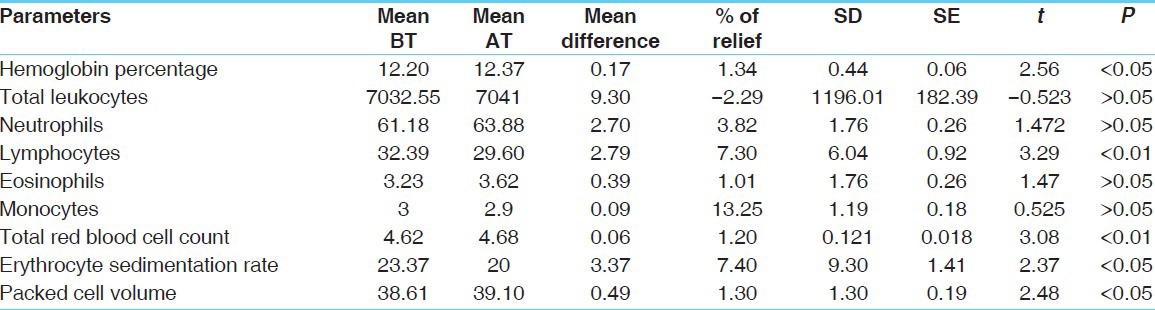
On Hamilton Anxiety Rating Scale, both the groups showed highly significant relief (P`0.001) from all the symptoms individually. In comparison to the results obtained from Group B, the Group A showed highly significant relief with respect to intellectual cognitive functions (79.03%), somatic (muscular) disorders (83.71%), depression (74.12%), and a significant relief from fear (81.11%). On Hamilton Depression Rating Scale, both the groups showed highly significant relief (P`0.001) from all the symptoms individually. However, the comparative results were insignificant. The results of symptoms of Mini Mental State Examination showed that both the groups provided highly significant (P`0.001) improvement individually. In comparison with SG, GMR showed highly significant improvement in registration (9.30%), attention and calculation (24.49%), and a significant improvement in language (13.51%) and in total score (14.89%) [Table 4]. The results obtained with hematological parameters reveal that Group A showed [Table 5] highly significant increase in total RBC (1.20%) count, a significant increase in Hb% (1.34%), packed cell volume (PCV) (1.30%) and a significant decrease in erythrocyte sedimentation rate (ESR) value (7.40%), while Group B showed highly significant decrease in RBC count (4.30%), PCV (3.34%), and a significant decrease in Hb% (1.55%).
Table 4.
Comparison of the effects of GMR and SG on the symptoms of mini mental state examination
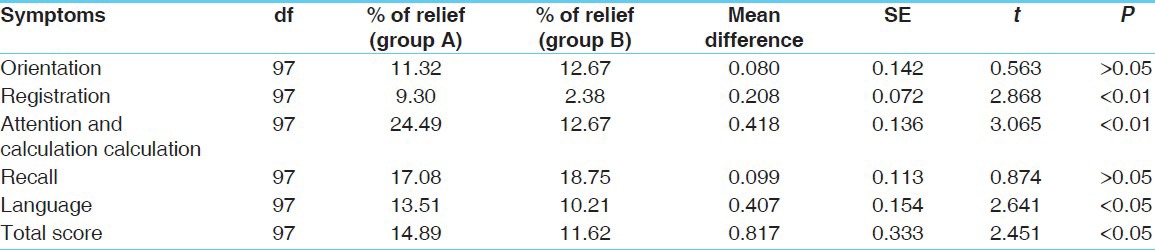
Table 5.
Effect of GMR on hematological parameters in Group A (n=43)
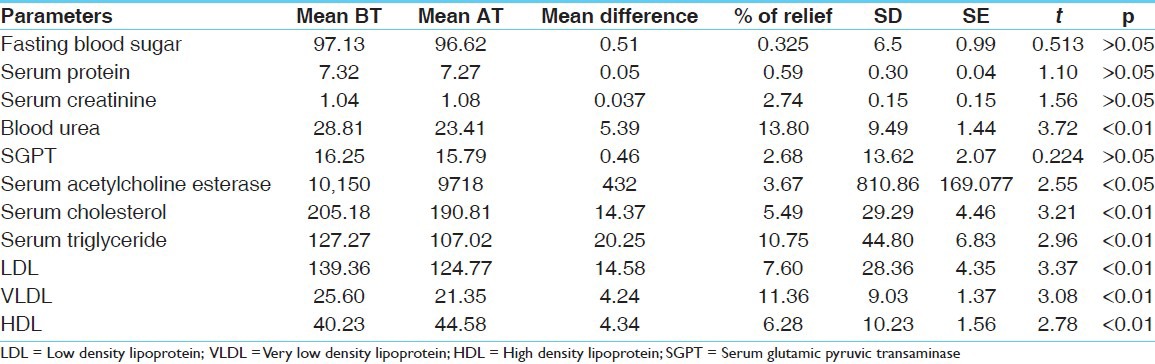
With regard to the biochemical parameters, Group A showed highly significant decrease (P`0.01) in serum cholesterol, serum triglyceride, low density lipoprotein (LDL), and very low density lipoprotein (VLDL) levels, while high density lipoprotein (HDL) increased highly significantly (P`0.01) and a significant decrease (P`0.05) was found in blood urea (13.80%) as well as serum AChE (3.67%) within normal limits [Table 6]. The Group B showed highly significant increase in blood urea (10.04%), but it was within normal limit. Other parameters were found to be statistically insignificant.
Table 6.
Effect of GMR on biochemical parameters in Group A (n=43)
Regarding the overall effect, Group A showed marked improvement in 18.6% patients, moderate improvement in 74.4% patients and mild improvement in 7.0% patients, while Group B showed moderate improvement in 32.2% patients and mild improvement in 67.8% patients.
Discussion
It has been mentioned in texts that GMR contributes to enhance the memory power within a short period. On the basis of Rasapanchaka, the pharmacotherapeutic properties reveal that it contains Katu, Tikta and Madhura in Rasa, and the effect of Katu and Madhura in Vipaka. Moreover, due to various properties of Tikshna, Laghu, Ruksha, Sara, Guru and Snigdha, it possesses markedly Ushna Virya and mildly Sheeta Virya. Accordingly, GMR was considered to be an effective treatment for Tridoshahara. In Ayurveda, it is clearly emphasized that Smritibhramsha (memory impairment) results due to Rajas and Tamasdoshas in the mind. These doshas are responsible for producing avarana over the mind. The relief from the symptoms has been found to be statistically highly significant.
These observations reveal that the drug might have counteracted or pacified Raja and Tamo Doshas, so Avarana of mind was removed and the disease was subsided or controlled. Further pharmacological studies have proven that Vaca (Acorus calemus Linn.) and Shankhapushpi (Convolvulus pluricaulis Chois) have anxiolytic, memory enhancing, anti-stress, antidepressant, tranquilizing and sedative activities.[20, 21] Further, it was found that there was a significant improvement by 14.84% on the total score of the Mini Mental State Examination [Table 4]. So, these evidences indicate the positive role of Medhya property of GMR on Senile Memory Impairment among elderly individuals. Considering the symptoms of memory impairment along with the cognitive decline, a highly significant result was obtained both from GMR and SG [Table 1 and Table 2]. However, in comparison, GMR has given better relief for the majority of symptoms [Table 3]. The Medhya Rasayanas are special Ayurvedic neuro nutraceuticals which are specific to brain and nervous system. They are claimed to promote cognitive function of the brain.[22] Further, it was mentioned in the Caraka Samhita that Shankhapushpi, a Rasayana drug, has the property of promoting intellect.[23] Moreover, Group B also showed improvement of memory due to the Medhya effect of ghee.[24] The serum AChE value has shown an upper range in both the groups before the treatment and a significant decrease was observed after the treatment in Group A [Table 6]. The recent advances in clinical research reveal that AChE activity is increased in human cerebrospinal fluid during aging[25] and scientists believe that dementia-related memory issues stem from the increased breakdown of acetylcholine due to a preponderance of AChE which degrades acetylcholine.[26] Furthermore, a decrease in AChE activity has noted in the treated animals, leading to an increase in the cholinergic activity in the brain.[27] The significant reduction of AChE in Group A shows that GMR exerts its effect on memory enhancement by increasing the cholinergic function by preventing the breakdown of acetylcholine in the aging human brain.
Conclusions
Senile Memory Impairment can be correlated to Jarajanya Smritibhramsha according to Ayurveda, and imbalance of Trigunas through aggravation of Rajas and Tamas Doshas in the mind leads to development of Senile Memory Impairment among elders. Modern literature reveals that Senile Memory Impairment is closely associated with cognitive decline during aging. All the patients of Senile Memory Impairment were having features of impairment of short memory and long memory in this study. Manasika Nidana (psychic factors), Aharaja (dietary) and Viharaja (behavioral) factors, which were reported by the patients, play a major role in the pathogenesis of Senile Memory Impairment by vitiating Rajas and Tamas Doshas in the mind. Those factors were Chinta (thoughts), Krodha (anger), Shoka (worries), Chittodvega (anxiety), Bhaya (fear), Moha (illusions), Ruksha Ahara (dried food), Ratri Jagarana (awaking at night), etc. GMR has shown statistically highly significant improvement on short memory impairment as well as long memory impairment in Senile Memory Impairment, at the level of P`0.001. Reduction of AChE showed enhancement of memory functions due to improvement of cholinergic actions in the human brain in the trial group (Group A). GMR has shown memory enhancing, antidepressant, anti-stress, and anxiolytic potential. Hence, Guduchyadi Medhya Rasayana therapy has proved so as to provide better improvement in comparison to the control group.
References
- 1.Ageing and Age Related Diseases. [Last accessed on 2010 Oct 24]. Available from: http://www.novapublishers.com .
- 2.Anonymas. New Delhi: Ministry of Health and Family Welfare; 2008. Report on “National Campaign on Ayurvedic and Siddha for Geriatric Health Care”, C.C.R.A.S, Department of AYUSH; p. 13. [Google Scholar]
- 3.Anonymous. Bauddhaloka, Mawata, Colombo 7, Sri Lanka: United National Population Fund, 202; 2004. Ageing Population in Sri Lanka; p. 226. [Google Scholar]
- 4.Sadock BJ, Sadock VA. Synopsis of Psychiatry. 10th ed. New Delhi: Published by Wolterskluwer (India) Pvt. Ltd; 2007. p. 1348. [Google Scholar]
- 5.Sadock BJ, Sadock VA. Synopsis of Psychiatry. 10th ed. New Delhi: Published by Wolterskluwer (India) Pvt. Ltd; 2007. p. 1348. [Google Scholar]
- 6. [Last accessed on 2010 October 24]. Available from: http://www.httpIjudmila.org/zzppd/2pgs7.pdf .
- 7.Dubey GP, Aruna Agrawal. Varanasi, India: I.M.S, B.H.U; 1996. Dixit SP Role of Bacopamonnier in prevention and Management of Dementia among aged. [Google Scholar]
- 8. [Last accessed on March]. Available from: http://www.med.nyu-edu/adc/forpatients/memory.html .
- 9.Agnivesha: Caraka Samhita, Cakrapani Datta’s Ayurveda Dipika. Sharirasthana. 7th ed 2002. [Google Scholar]; vaidya Sharma R.k, Vaidya Bhagwan Dash., editors. 101. Vol. 1. Varanasi: Chowkambha Sanskrit Series Office; p. 337. [Google Scholar]
- 10.Sushruta: Sushruta Samhita. 3rd ed. Vol.1 2007. [Google Scholar]; Vidhya Srikantha Murthy RK, editor. 4. Vol. 24. Varanasi: Chaukambha Orientalia; p. 175. [Google Scholar]
- 11.Madhavakara . Jararoganidana, Verse No 2-3. 2006. Madhava Nidanam with Madhukosa Sanskrit commentary. [Google Scholar]; Upadhyaya Y, editor. Varanasi: Chaukambha Prakshan; Part 2; p. 595. [Google Scholar]
- 12.Vaidya Murthy PH., translator. Sarngadhara Samhita. Pratham Khanda. 20. Vol. 6. Varanasi: Chaukambha Sanskrit Series Office; 2001. p. 56. [Google Scholar]
- 13.Agnivesha: Caraka Samhita, Cakrapani Datta’s Ayurveda Dipika. Vimanasthana. 7th ed 2002. [Google Scholar]; Sharma RK, Vaidya Bhagwan Dash, editors. 122. Vol. 8. Varanasi: Chowkambha Sanskrit Series Office; p. 277. [Google Scholar]
- 14. [Last accessed on October 14]. Available from: http://http://www.universe-review/R10-27 ageing.htm .
- 15. [Last accessed on 2008 July 11]. Available from: http://www.google.com/academic.research.microsoft.com/ age-associated-memory impairment-a-neuropsychological-and-epidemiological-study .
- 16.Singh RH. The Holistic Principles of Ayurvedic Medicine. 1st ed. Delhi: Chaukhamba Sanskrit Pratishthan; 1998. p. 207. [Google Scholar]
- 17.Rasayanadikara. 7th ed 2002. Yogaratnakara, with Vidyotini Hindi Commentary. [Google Scholar]; Bhisagratna Brahma Sankar Sastri., editor. New Delhi: Chaukambha Publication; p. 501. [Google Scholar]
- 18.Michael Swash, Michael Glynn. 22nd ed. Philadelphia, USA: Harcourt Publishers Limited; 2007. Hutchison’s Clinical Methods; p. 41. [Google Scholar]
- 19.Sadock BJ, Sadock VA. Synopsis of Psychiatry. 10th ed. New Delhi, India: Wolterskluwer (India) Pvt. Ltd; 2007. pp. 310–314. [Google Scholar]
- 20.Billore KV, Yelne MB, Dennis TJ. Database on Medicinal Plants used in Ayurveda. Vol. 7. Janakpuri, New Delhi: Central Council for Research in Ayurveda and Siddha; 2005. pp. 433–5. [Google Scholar]
- 21.Sharma PC, Yelne MB, Dennis TJ. Database on Medicinal Plants used in Ayurveda. Vol. 1. Janakpuri, New Delhi: Central Council for Research in Ayurveda and Siddha; 2000. pp. 469–71. [Google Scholar]
- 22.Singh RH, Narsimhamurthy K, Singh G. [accessed on 2010 Nov 27]. Available from: http://www.springerlink.com.Neuronutrient impact of Ayurveda Rasayana in Brain Aging .
- 23.Agnivesa: Caraka Samhita, Cakrapani Datta’s Ayurveda Dipika. Chikitsasthana, 1:3/30-31. 2nd ed 1996. [Google Scholar]; Sharma RK, Vaidya Bhagwandash. Vol. 111. Varanasi: Chowkhamba Sanskrit Series Office; p. 46. [Google Scholar]
- 24.Babu M.S.S, editor. Yogaratnakara. Vol. 1. Varanasi: Chowkhamba Sanskrit Series office; 2005. p. 132. [Google Scholar]
- 25. [accessed on 2010 Dec 1]. Available from: http://www.springerlink.com .
- 26. [accessed on 2010 Jun 12]. Available from: http://www.articlesnatch.com .
- 27. [accessed on 2010 Jun 12]. Available from: http://www.onlinepharmacytech.info .