

Abstract
Background:
The aim of this study was to study the knowledge and attitude of the pediatricians and family physicians on the dental counterpart, i.e. pediatric dentistry and the objective of this study were to determine what can improve the knowledge and attitude on pediatric dentistry and suggest certain methodologies to more participation of physicians in improving oral health.
Materials and Methods:
A systematic random survey of 400 pediatricians and 400 family physicians received a questionnaire pertaining to individual details, approach towards pediatric dentistry, knowledge level and the training on oral health received.
Results:
Most of pediatricians and family physicians acknowledged the importance of pediatric dentistry. Less of pediatricians and more of family physicians predicted the parents may pose a barrier for referral. More number of pediatricians were aware of the oral benefits of breast feeding when compared to the family physician. Most of the practitioners in both groups were less aware of the first dental visit including ECC. Acknowledgement of the role in cleft lip and palate was more or less same in both groups of practitioners were as the effect of systemic disease on oral health was recognized by more number of pediatricians. Only a small percentage in both the groups acknowledged the cariogenicity of medicated syrups, which was substantiated by the fact that only a small number of physicians underwent dental training and most of them were accepting to undergo training.
Conclusion:
When basic medical training is provided in dental school, medical schools can also provide dental training. Dental lectures can also be incorporated into CME programs and recognition of pediatric dentistry by providing referral to needy patients have been suggested.
Keywords: First dental visit, preventive oral care, referral
INTRODUCTION
Despite the pronounced improvement of oral and dental status, dental caries is still a common dental disease. The factor which almost affects the preventive dentistry performance is the knowledge and function of the medical group concerning this issue. An important aspect of the child's general care should involve the first dental visit. The quality of preventive health care and the future oral health is determined by the first dental visit. Recommendations for early dental visits for children suggest its completion by 12 months of age.[1–4]
The medical office is considered an opportune site to reach large numbers of children who make a medical visit but not a dental visit. Physicians and their auxiliaries can assess risks for dental problems and counsel parents and their children about the prevention of these problems. They also can provide screening services for early detection of dental disease, provide advice about the need to seek dental care, and refer those in need. A key element of comprehensive care for children thus involves the coordination of services between medical and dental providers so that the appropriate health care professionals can provide appropriate services at the appropriate ages.[5] Saliva is the most non-invasive and the most available body fluid containing inorganic and organic compounds that forms a mirror of the body's health offering a distinct advantage over serum in being cost effective.[6] Saliva has been reliably used to detect HIV 1 and 2, and viral hepatitis A, B and C. It can also be used to monitor a variety of drugs including marijuana, cocaine and alcohol.[7]
Basic questions about the dental referral process and its outcomes remain unanswered. This study conducted in the city of Chennai and its suburbs is designed keeping in mind to gather the data on the level of knowledge of pediatric dentistry, importance of the first dental visit and referrals to a specialist for dental care. Even though similar studies have been recorded but this study is more comprehensive and recorded in an Indian urban region.
MATERIALS AND METHODS
This study uses information from baseline questionnaires, totaling 800, which are completed by various health care professionals. The list of pediatricians and family physicians were obtained from various private hospitals and associations in the year 2011 and the questionnaires were sent to them by mail as we felt that direct recording may affect the response. A comprehensive questionnaire were prepared based on studies done by Yahya and Solmaz,[8] Giuseppe et al.,[9] Georgia Cruz et al.[5] and Prakash et al.[10] The data was collected using a mailed self-administered questionnaire. The participants received a short questionnaire, a covering letter and an addressed, stamped return envelope. The items were evaluated through choosing one of the options completely, yes or no. The questionnaire was divided into the following four sections;
Individual details including: Name, age, sex, medical background
The approach of the practitioner towards pediatric dentistry and factors affecting it.
The knowledge level of the practice of pediatric dentistry in relation to age at which care should be started, maternal considerations, preventive methods and various common treatment methods. Importance regarding early childhood caries (ECC) has been included in this part of the questionnaire along with the cariogenic potential of medicated syrups.
Training on oral health received by the practitioner were recorded and willingness to receive training.
RESULTS
A total of 800 questionnaires (400 - pediatricians, 400 - family physicians) were mailed and a total of 696 of questionnaires were returned duly completed out of which 371 were from pediatricians and 325 from general physicians and the results were tabulated in four sections and discussed.
DISCUSSION
This survey was done with the need to emphasize on the fact that there is a need to improve the pediatrician / family physician and the pedodontist's relationship, as well as to study on the lacunae on the areas where the physicians need to improve the knowledge of oral health and to recognize the importance of pediatric dentistry. The approach of the practitioners [Table 1] showed that more than 80% of pediatricians and around 60% of general practitioners knew the existence of the specialty and the importance of the primary dentition and examining them. The results correlate with similar studies showing more number of pediatricians than general practitioners, knowing about the specialty and importance of the primary dentition.[10] Studies on oral examination by family physicians were not available but an American study showed that only 54% of pediatricians examined the oral cavity of more than half of the 0-3 year olds.[11] Certain cranio-facial abnormalities can be diagnosed soon after birth, like Pierre Robin syndrome with the characteristics of glossoptosis and cleft lip and/or palate, lesions such as ‘Bohn's nodules’ and ‘Esptein's pearls’ being embryonic remnants and neonatal teeth that can make nursing difficult along with a risk of aspiration[12] making examination of the oral cavity soon after birth a necessity.
Table 1.
Evaluation of the knowledge of the specialty of pediatric dentistry, importance of the primary dentition and referral attitudes among pediatricians and family physicians

It was noted that around 60% of the pediatricians and around 90% of the general practitioners felt that the parents will pose a barrier in the referral and importance of primary dentition. Studies on the relationship between parental attitude and its influence on the referral of patients were not available but age of the patient as an influencing factor for referral by pediatricians showed that practice that had infants or toddlers in the practice had lesser referral percentage.[5]
The knowledge and understanding of the health care providers [Table 2] showed that nearly 70% of the pediatricians and only 26% of the family physicians could relate the importance of breast feeding and oral health. During breast feeding the infants’ oral muscles are exercised strenuously in suckling, an important influence on the thrust and growth of the mandible, in addition to imparting maternal immunological components. Appropriate, health-promoting practices, such as breastfeeding, should be encouraged by healthcare professionals.[13] A study on children participating in the promotion of breastfeeding intervention trial, a cluster-randomized trial of a breast-feeding promotion intervention based on the WHO/UNICEF baby-friendly hospital initiative showed no evidence of beneficial or harmful effects of breast feeding at an early school age.[14] What the pedodontist needs to emphasize is the oral hygiene, duration of breast feeding in association with a pediatrician and preventive methods to decrease the possibility of dental caries.
Table 2.
Evaluation of knowledge of preventive practices and pediatric dentist's role in early intervention and special health care needs among pediatricians and family physicians
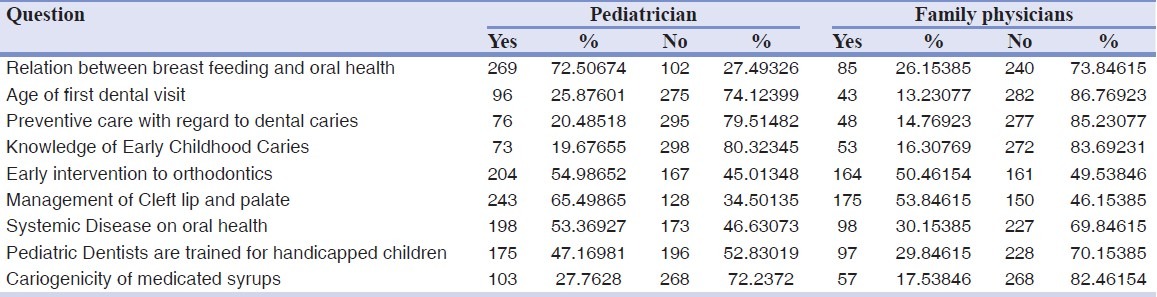
There was decrease in the percentage for both groups with respect to the knowledge of the age of first dental visit, preventive care and knowledge of early childhood caries (ECC) with less than 50% of family physicians being aware of the same. Similar Indian studies in showed that more than 90% of the pediatricians having knowledge of the same[15] but information from family physicians were not recorded. Analysis of Indian studies on the amount of oral health education received in the form of continuing medical education programs were not available yet most respondents received 2 h or less of preventive dental education during medical and specialty training. Pediatricians were better informed than family physicians in the areas of general dental knowledge and prevention counseling related to oral health.[16] This could be the reason why this study revealed a low percentage of family physicians having knowledge of ECC. The site of implementation of oral health education seems to be an important factor where the most effective site was that of the physician's office itself.[17] Children with ECC are three times more likely to develop dental caries in the permanent dentition.[18] A study in United States has suggested the one year dental visit should be performed for all children in the lower socioeconomic status and can be elective for the middle and higher socioeconomic group, however when the risk factors are high the 1 year dental visit can be implemented.[2] Pediatric dentistry as a specialty that provided early solutions to predictable orthodontic problems and its early role in cleft lip and palate as recognized by 50-60% of the pediatricians and around 50% of the family physicians. There are specific needs with regards to the child's oral development that can be identified in different stages of development. The dentist forms an important role in addressing the parent's concern of the aesthetics, early management involving preparing for surgery, management of pain, sepsis and when necessary dental extraction.[19]
The knowledge of effect of systemic disease on oral health had a higher response by around 53% of pediatricians and only 30% of the family physicians. Oral changes such as involvement of the temporomandibular joint and asymmetry of the mandible are seen in patients diagnosed with juvenile idiopathic diabetes[20] and Type I diabetes mellitus in children showed delayed dental development after the age of 10 with increase in periodontal disease and higher incidence of caries in those with poor metabolic control.[21] Defects if the tooth structure such as enamel hypoplasia is seen in patients with renal disease and tetracycline used to treat infection cause intrinsic staining in hemodialysis patient. Extrinsic staining can be prevented by using medication in the form of capsules rather than syrups.[22] Studies on oral health status of children admitted in a pediatric intensive care unit showed an significant increase in plaque accumulation and gingival inflammation between admissions citing the necessity for a better treatment regimen.[23] Poor oral health on the other hand as seen in patients with chronic kidney disease may contribute to protein energy wasting, inflammation, infections and atherosclerotic complications, justifying a necessity for increased dental care.[24]
Pediatric dentists as trained professionals in handling handicapped children were acknowledged only by 47% of the pediatricians and only 29% of the family physicians. The importance of early referral to a pediatric dentist is necessary as the specialty involves patient control, caries preventive and management under general anesthesia, special gingival care involving children, especially under anti-convulsion therapy, dental trauma protection and treatment were the approach is quiet different than that of normal children as the patient cooperation does not allow fixed replacement and finally early intervention orthodontics such as a well timed extraction program to achieve a fairly acceptable occlusion.[25]
Only 27% of pediatricians and 17% of family physicians acknowledged the importance of the cariogenicity of syrups prescribed in dental practice. It has been noted that though antibiotics can have an effect on bacteria, their role is minor in caries prevention when compared to fluoride.[26] A Brazilian study revealed that around 56% of the medicated syrups had a high sugar concentration, with pH values below the critical value and high acidity values, all of them increase the cariogenic and erosive potential.[27]
The third part of the questionnaire [Table 3] dealt with the knowledge level of the practitioners that only 27% of pediatricians and only 10% of general practitioners had received training in oral health and more than 90% of the practitioners were willing to undergo training in oral health. The most common barrier to participation in oral health-related activities in their practices was lack of training, which was cited by 41%. Less than 25% of pediatricians had received oral health education in medical school, residency, or continuing education.[11] Studies have shown than the rates of preventive oral care in medical offices were not influenced by the CME courses. Increased practice volume in pediatric offices showed a greater rate of preventive dental services offered when compared to family physicians showing a lesser volume of pediatric patients. An important aspect noted physicians was financial reimbursement that seemed be a significant incentive. Intensive CDE programs would be influential in later-trained practitioners.[28] There seem to be certain barriers in adopting dental services, such as integrating the preventive dental services into the practice routines in the form of insufficient time to plan for change or provide services, practice procedures, and practice turmoil, which could be easily overcome by changes in practice timing along with training. Resistance by staff and colleagues was another obstacle and the incentive system seems to come over this. Applying fluoride varnish was the third obstacle as the physician does not have a working position as in a dental chair. This can be overcome by knee to knee position and provision of training materials and in-office training with a child patient for demonstration is suggested.[29]
Table 3.
Evaluation of the training received by the physicians and willingness to receive training among pediatricians and family physicians

CONCLUSIONS
Since the day of Hippocrates, Father of Medicine, the Physician and Surgeon have made remarkable progress but there seems to be some missing in the relationship in the form of oral care, which should have been augmented by the dentist. The dental surgeon has undergone basic medical training including a thorough knowledge of head and neck anatomy; similarly the medical fraternity can be trained in the implementation of oral health. With the results obtained the following can be suggested.
Collaboration between pediatric dentists and physicians for implementation of oral health education programs.
Promote oral examination of neonates by a pedodontist soon after birth.
Promotion of healthy referral practice maintaining ethics, even though the literature review shows a favor towards monetary benefits.
Enhancing out-patient and in-patient based continuous review of long term admissions and implementation of preventive procedures.
Promote the need for increased specialty dental care for special children.
Advise pharmaceutical companies to promote and convert to syrups with sugar substitutes.
Counseling sessions for to be parents.
The need for an increased awareness of oral hygiene habits and insufficient awareness among the physicians apparently warrants the common effort of both dentists and physicians for a better outcome.
ACKNOWLEDGEMENT
Dr. B. R. Nammalwar MD, DCh, DM, Consultant Pediatric Nephrologist, Metha's Children's hospital.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Douglass JM, Douglass AB, Silk HJ. Infant oral health education for pediatric and family practice residents. Pediatr Dent. 2005;27:284–91. [PubMed] [Google Scholar]
- 2.Nainar SM, Straffon LH. Targeting of the year one dental visit for United States children. Int J Paediatr Dent. 2003;13:258–63. doi: 10.1046/j.1365-263x.2003.04602.x. [DOI] [PubMed] [Google Scholar]
- 3.Rayner JA. The first dental visit: A UK viewpoint. Int J Paediatr Dent. 2003;13:269. doi: 10.1046/j.1365-263x.2003.00463.x. [DOI] [PubMed] [Google Scholar]
- 4.Widmer R. The first dental visit: An Australian perspective. Int J Paediatr Dent. 2003;13:270. doi: 10.1046/j.1365-263x.2003.00461.x. [DOI] [PubMed] [Google Scholar]
- 5.dela Cruz GG, Rozier RG, Slade G. Dental screening and referral of young children by pediatric primary care providers. Pediatrics. 2004;114:e642–52. doi: 10.1542/peds.2004-1269. [DOI] [PubMed] [Google Scholar]
- 6.Greabu M, Battino M, Mohora M, Totan A, Didilescu A, Spinu T, et al. Saliva-a diagnostic window to the body, both in health and in disease. J Med Life. 2009;2:124–32. [PMC free article] [PubMed] [Google Scholar]
- 7.Lee JM, Garon E, Wong DT. Salivary diagnostics. Orthod Craniofac Res. 2009;12:206–11. doi: 10.1111/j.1601-6343.2009.01454.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Yahya BN, Solmaz S. The knowledge, approach and function of pediatricians in prevention of caries in Tehran. J Indian Soc Pedod Prev Dent. 2004;22:148–53. [PubMed] [Google Scholar]
- 9.Di Giuseppe G, Nobile C, Marinelli A, Angelillo I. Knowledge, attitude and practices of pediatricians regarding the prevention of oral diseases in Italy. BMC Public Health. 2006;6:176. doi: 10.1186/1471-2458-6-176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Prakash P, Lawrence HP, Harvey BJ, McIsaac WJ, Limeback H, Leake JL. Early childhood caries and infant oral health: Paediatricians’ and family physicians’ knowledge, practices and training. Paediatr Child Health. 2006;11:151–7. doi: 10.1093/pch/11.3.151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lewis CW, Boulter S, Keels MA, Krol DM, Mouradian WE, O’Connor KG, et al. Oral health and pediatricians: Results of a national survey. Acad Pediatr. 2009;9:457–61. doi: 10.1016/j.acap.2009.09.016. [DOI] [PubMed] [Google Scholar]
- 12.Sigal MJ, Levine N. Infant oral health care. Can Fam Physician. 1988;34:1419–24. [PMC free article] [PubMed] [Google Scholar]
- 13.Westover KM, DiLoreto MK, Shearer TR. The relationship of breastfeeding to oral development and dental concerns. ASDC J Dent Child. 1989;56:140–3. [PubMed] [Google Scholar]
- 14.Kramer MS, Vanilovich I, Matush L, Bogdanovich N, Zhang X, Shishko G, et al. The effect of prolonged and exclusive breast-feeding on dental caries in early school-age children.New evidence from a large randomized trial. Caries Res. 2007;41:484–8. doi: 10.1159/000108596. [DOI] [PubMed] [Google Scholar]
- 15.Murthy GA, Mohandas U. The knowledge, attitude and practice in prevention of dental caries amongst pediatricians in Bangalore: A cross-sectional study. J Indian Soc Pedod Prev Dent. 2010;28:100–3. doi: 10.4103/0970-4388.66747. [DOI] [PubMed] [Google Scholar]
- 16.Sanchez OM, Childers NK, Fox L, Bradley E. Physicians’ views on pediatric preventive dental care. Pediatr Dent. 1997;19:377–83. [PubMed] [Google Scholar]
- 17.Kressin NR, Nunn ME, Singh H, Orner MB, Pbert L, Hayes C, et al. Pediatric clinicians can help reduce rates of early childhood caries: Effects of a practice based intervention. Med Care. 2009;47:1121–8. doi: 10.1097/MLR.0b013e3181b58867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Li Y, Wang W. Predicting caries in permanent teeth from caries in primary teeth: An eight-year cohort study. J Dent Res. 2002;81:561–6. doi: 10.1177/154405910208100812. [DOI] [PubMed] [Google Scholar]
- 19.Rivkin CJ, Keith O, Crawford PJ, Hathorn IS. Dental care for the patient with a cleft lip and palate. Part 1: From birth to the mixed dentition stage. Br Dent J. 2000;188:78–83. doi: 10.1038/sj.bdj.4800393. [DOI] [PubMed] [Google Scholar]
- 20.Twilt M, Schulten AJ, Nicolaas P, Dulger A, van Suijlekom-Smit LW. Facioskeletal changes in children with juvenile idiopathic arthritis. Ann Rheum Dis. 2006;65:823–5. doi: 10.1136/ard.2005.042671. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Orbak R, Simsek S, Orbak Z, Kavrut F, Colak M. The influence of type-1 diabetes mellitus on dentition and oral health in children and adolescents. Yonsei Med J. 2008;49:357–65. doi: 10.3349/ymj.2008.49.3.357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ertugrul F, Elbek-Cubukcu C, Sabah E, Mir S. The oral health status of children undergoing hemodialysis treatment. Turk J Pediatr. 2003;45:108–13. [PubMed] [Google Scholar]
- 23.Franklin D, Senior N, James I, Roberts G. Oral health status of children in a paediatric intensive care unit. Intensive Care Med. 2000;26:319–24. doi: 10.1007/s001340051156. [DOI] [PubMed] [Google Scholar]
- 24.Akar H, Akar GC, Carrero JJ, Stenvinkel P, Lindholm B. Systemic consequences of poor oral health in chronic kidney disease patients. Clin J Am Soc Nephrol. 2011;6:218–26. doi: 10.2215/CJN.05470610. [DOI] [PubMed] [Google Scholar]
- 25.Levine N, Sigal MJ. Dental care for the handicapped. Can Fam Physician. 1989;35:369–74. [PMC free article] [PubMed] [Google Scholar]
- 26.Mariri BP, Levy SM, Warren JJ, Bergus GR, Marshall TA, Broffitt B. Medically administered antibiotics, dietary habits, fluoride intake and dental caries experience in the primary dentition. Community Dent Oral Epidemiol. 2003;31:40–51. doi: 10.1034/j.1600-0528.2003.00019.x. [DOI] [PubMed] [Google Scholar]
- 27.Neves BG, Farah A, Lucas E, de Sousa VP, Maia LC. Are paediatric medicines risk factors for dental caries and dental erosion? Community Dent Health. 2010;27:46–51. [PubMed] [Google Scholar]
- 28.Slade GD, Rozier RG, Zeldin LP, Margolis PA. Training pediatric health care providers in prevention of dental decay: Results from a randomized controlled trial. BMC Health Serv Res. 2007;7:176. doi: 10.1186/1472-6963-7-176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Close K, Rozier RG, Zeldin LP, Gilbert AR. Barriers to the adoption and implementation of preventive dental services in primary medical care. Pediatrics. 2010;125:509–17. doi: 10.1542/peds.2009-1008. [DOI] [PubMed] [Google Scholar]