

Abstract
Background:
Based on the previous national oral health survey in India, some variation was observed in oral health status and behavior between the urban and rural population. Thus, the present study aimed to assess the dental caries experience in deciduous dentition of 6-year-old urban and rural schoolchildren of Udaipur district and to evaluate the influence of socio behavioral characteristics on dental caries experience.
Materials and Methods:
A combination of multi stage and cluster sampling procedure was executed to collect a representative sample of 875, 6-year-old school children. Clinical examination for caries was conducted using dmft (decayed, missing and filled teeth) index. Socio - demographic information was collected prior to clinical examination in addition to information on oral health behavior by personal interviews.
Results:
Only 7.8% children reported of brushing their teeth twice or more than twice daily. Rural children visited the dentist less often than the urban children (P < 0.05). Greater proportion of boys (62.2%) experienced caries than girls (55.1%), decayed component constituted a major contribution for dmft. Multivariate analysis demonstrated the influence of gender, urbanization, tooth brushing frequency, dental visits, parent's education and occupation on caries occurrence.
Conclusions:
Rural children and boys experienced greater caries than their urban and girl counterparts. Caries experience was related to the parent's occupation and education. Moreover, caries occurrence was influenced by brushing frequency and dental visiting habits.
Keywords: Dental caries, education of parent, occupation of parent, urbanization
INTRODUCTION
India, a developing country, faces many challenges in rendering oral health needs. Majority of Indian population resides in rural areas, of which more than 40% constitute children.[1] Dental caries is the single most prevalent chronic childhood disease worldwide,[2] and it causes significant economic loss due to heavy expenses of dental treatment.[3]
During the past two decades many industrialized countries have experienced a dramatic reduction in the prevalence of dental caries and this is ascribed to improved changing living conditions, adoption of healthy lifestyles, improved self-care practices, effective use of fluorides and establishment of preventive oral care programs[4] while increasing levels of dental caries has been observed in developing countries.[5]
Petersen has observed[6] that at the population level, oral health outcomes are related to distal socioenvironmental factors and characteristics of the oral health services available. In addition to the use of oral health services, proximal modifiable risk behaviors such as oral hygiene practices, dietary habits, tobacco use and excessive consumption of alcohol were found. Across countries and oral health systems, the existence of a social gradient (economic characteristics and educational background) in dental caries prevalence was found.
The prevalence of dental caries in 5-year-old children in India has been reported to be 50%[7] which is comparatively lower than many other parts of Asia.[8] It has been reported that few developing countries recently introduced school based oral health education and preventive programmes aimed at improving oral health behavior and status of the child population and inspiring results were observed from such health projects that have been conducted in Indonesia, Brazil, Madagascar and China.[9]
In India, unlike other developing countries no oral health education or preventive programs are in action, the only attempt in the field of oral health at national level was the national oral health survey that has been conducted in different states. Based on the results, some variation was observed in oral health status and behavior between the urban and rural population along with variation among the states where population of Rajasthan presented better oral health status than other states.
Thus, the present study intended to assess the dental caries experience in deciduous dentition of 6 year old urban and rural schoolchildren of Udaipur district and to evaluate the influence of socio behavioral characteristics on dental caries experience.
MATERIALS AND METHODS
The target population constituted 6-year-old school children of Udaipur district. Ethical approval for conducting the present cross sectional survey was obtained from ethical committee of Darshan Dental College and hospital. Prior permissions were taken from the District Education Officer for conducting the survey in selected schools. Verbal consent was obtained prior to examination from each subject and parent (mother or father) provided the proxy informed written consent on behalf of school children.
This survey is part of a large survey conducted on 6 and 12-year-old schoolchildren of Udaipur district. To facilitate collection of representative sample, a combination of multistage and cluster sampling procedure was executed. At first stage, four rural areas and four urban areas were selected randomly from 8 rural and 4 urban panchayat samithis, respectively. Later at second stage, four schools (two primary schools and two upper primary schools) in the each selected location were selected randomly (two each for boys and girls). In regions where there were no separate schools for boys and girls, co-education schools were included. At third stage, a cluster of first and sixth standard children were selected. Thus a total sample of 875 first standard children participated in the study, selected from a total of 16 primary schools. Subjects present on the days of the survey were included while physically challenged and systemically ill children were excluded.
Clinical examination was conducted by a single investigator under adequate illumination and dmft (decayed, missing, and filled teeth) index[10,11] was used to evaluate dental caries. In order to minimize the intra examiner variability, 10% subjects who underwent the clinical examinations were randomly selected in each school by the recorder for repeated examinations. Kappa co-efficient for intra-examiner reliability was found to be 92% for dmft.
Socio-demographic information such as name, age, gender, place of residence, occupation and education of the parents in addition to information on oral health practices (tooth cleaning practices, use of oral hygiene aids, use of tooth paste and dental visiting habits) was collected prior to clinical examination by personal interviews carried out by investigator himself.
Occupation and education status of parents was classified according to occupation and education components of Kuppuswamy scale.[12]
Statistical Package for Social Sciences (SPSS 15.0, Inc., Chicago, IL) was used for statistical analysis of data. Fisher exact test was used to assess statistical difference in proportions between two groups. Unpaired t-test and one way ANOVA were used to evaluate the significant differences in means between two and three or more groups respectively. Binomial multiple logistic regression analysis was executed to assess the influence of various independent variables on the dental caries occurrence. The dependent variable dental caries was dichotomized as presence or absence of dental caries.
The independent variables that were significant in bivariate analysis were categorized as; gender (boys and girls), location (rural and urban), parent's occupation (professional or semi professional, unskilled or unemployed and other occupations), parent's education (>10 years of education, 1-10 years of education and illiterate), brushing frequency (sometimes or never and more than once a day) and dental visit (never been and had been to dentist at least once during lifetime). The effect of each independent variable was assessed adjusting for all other variables in the model. Odds ratio was calculated for all the variables with 95% confidence intervals.
RESULTS
Among the selected sample of 875 school children, 461 and 412 belonged to urban and rural locations respectively while 463 were boys and 412 were girls.
The caries prevalence and mean caries experience of 6-year-old children was found to be 58.9% and 1.69 (1.99) respectively as illustrated in Table 1. There was a significant difference for the caries prevalence between the genders with greater proportion of boys (62.2%) experiencing caries than girls (55.1%), decayed component constituted a major contribution in the total caries experience.
Table 1.
Dental caries prevalence and experience of 6-year-old schoolchildren according to location of residence and gender

Statistical analysis revealed significant differences for mean number of filled teeth between the locations of residence. Though insignificant, mean dmft among rural subjects (1.79) was greater than the urban individuals (1.60) while it was greater in boys (1.77) than girls (1.60).
Tables 2 and 3 display the caries experience in relation to parent's occupation and education respectively. Children whose fathers were professionals (1.25) experienced the lowest caries in contradiction to skilled (2.50). Children of semi-professional (1.00) and unskilled (2.23) mothers had lowest and highest caries experience, respectively. When parent's level of education was considered highest caries experience was observed among children of fathers (2.92) and mothers (2.82) who completed primary school education. Lowest mean dmft was among children of fathers who had a professional or honors degree and graduate or post-graduate mothers. One way ANOVA revealed significant differences between the parent's occupation and level of education for filled component of dmft.
Table 2.
Mean caries experience in primary dentition of 6-year-old children according to parent's occupation
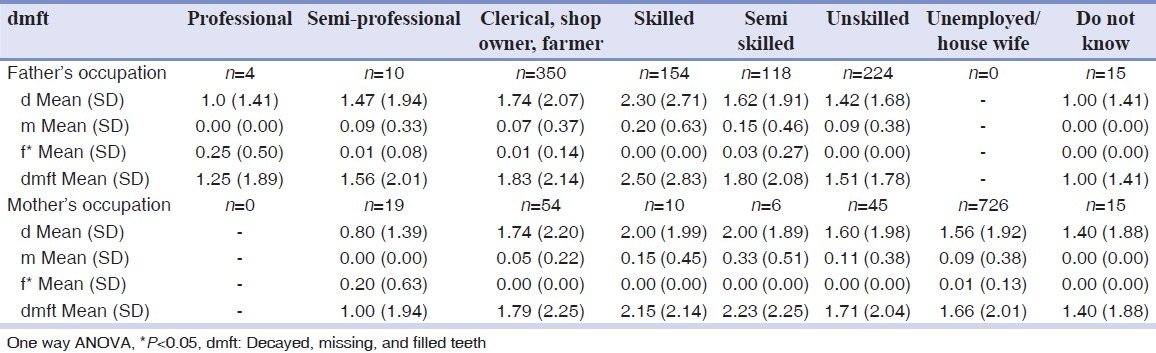
Table 3.
Mean caries experience in primary dentition of 6-year-old children according to parent's level of education
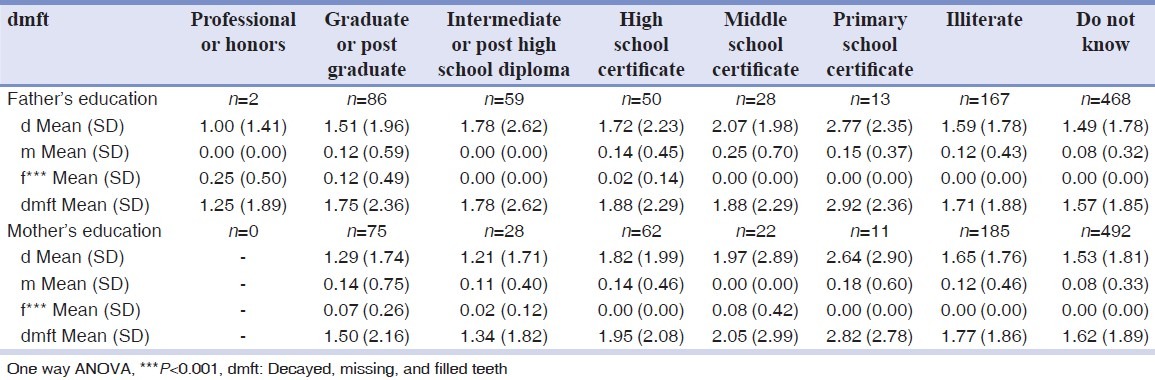
Table 4 documents the frequencies of oral health practices and statistically significant differences were observed by location and gender for most of the practices.
Table 4.
Percentage distribution of 6-year-old school children according to various oral health practices in relation to location and gender
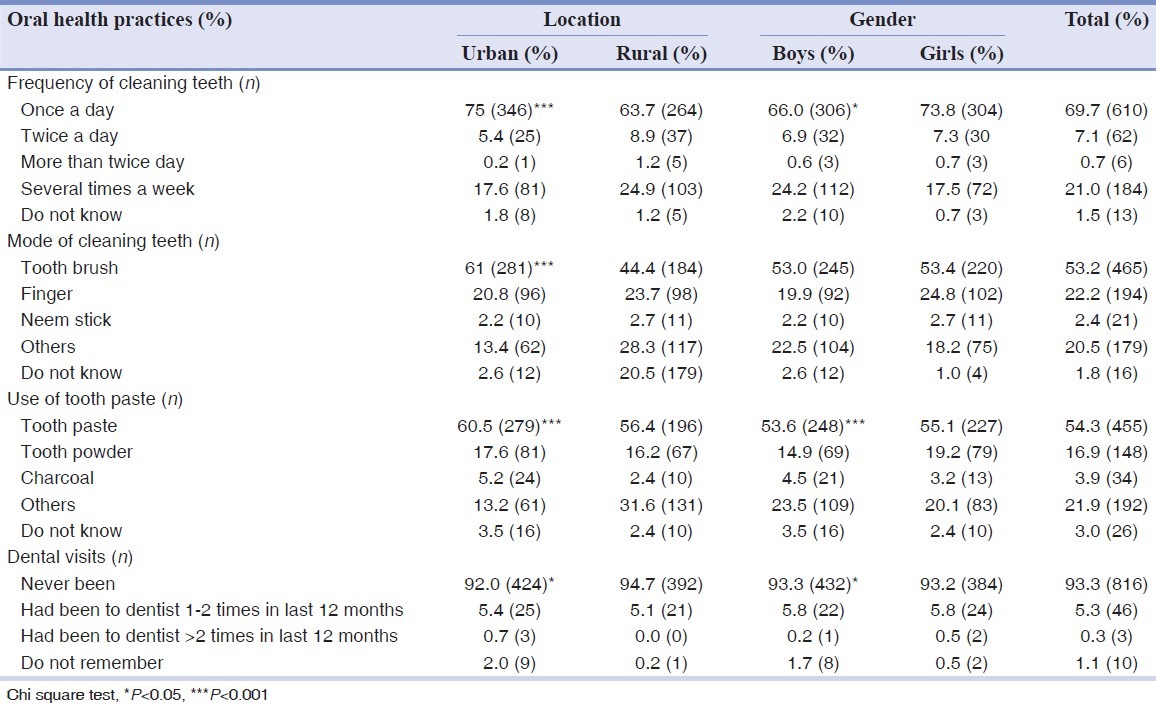
Among the urban children, 75% reported that they cleaned their teeth at least once daily against 63.7% of rural children. Barely half (53.2% and 54.3%) of the 6-year-old children said that they used toothbrush and toothpaste when they cleaned their teeth and only 7.8% children claimed of brushing twice or more than twice daily. Among the urban children who cleaned their teeth, 61% used tooth brush in comparison to 44.4% of rural children. There was significant difference between genders and location of residence for tooth paste usage, 60.5% of urban against 56.4% rural and 53.6% boys against 55.1% girls. Rural children visited the dentist less often than the urban children (P < 0.05) and 93.3% of children had never been to dentist.
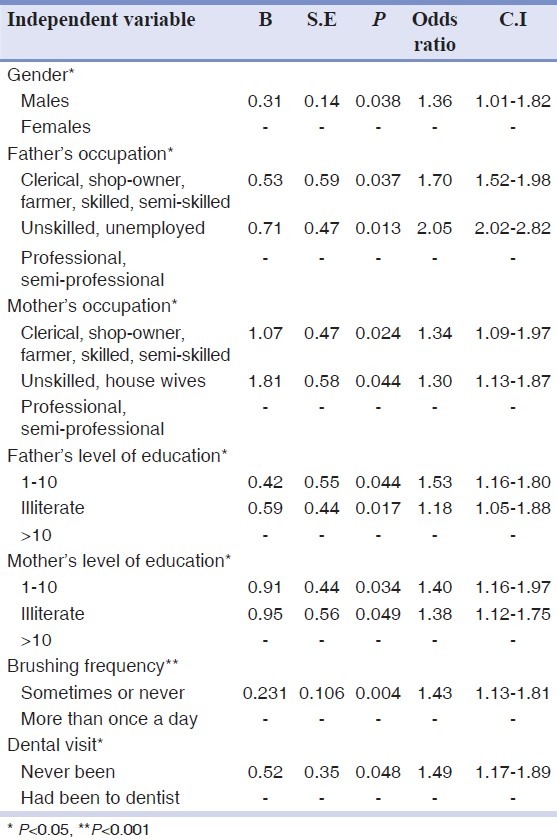
Logistic regression analysis was employed to determine the influence of various socio-behavioral variables on dental caries [Table 5]. Only those independent variables that had a significant influence on the dental caries occurrence are presented in the table. Boys were more likely to experience caries than their girl counterparts. Parent's occupation and level of education also played an important role, children of professional or semi professional parents and those who have completed at least 10 years of education were less likely to demonstrate caries. The association between oral hygiene practices and caries occurrence was evident, subjects who cleaned their teeth at least once a day were less likely to have caries than those who cleaned their teeth rarely or never (OR = 1.43; CI-1.13-1.81). Moreover, children those who never visited a dentist were almost one half times more likely to have dental caries than those who had been to dentist sometime in their life (OR = 1.49, CI-1.17-1.89).
Table 5.
Logistic regression analysis with presence or absence of caries as dependent variable and various socio-behavioral predictors as independent variables among 6-year-old schoolchildren of Udaipur district
DISCUSSION
The present study provides epidemiological data regarding dental caries experience in primary dentition of 6-year-old urban and rural schoolchildren of Udaipur district, which helps in planning preventive programmes for this population. In addition, emphasis was given to assess the effect of socio-behavioral risk factors on dental caries experience.
The survey was not conducted on a national scale and therefore, the data are not representative of the whole country. However, the sample is considered to be representative of the school children from whole district as the study population was randomly recruited from all the divisions of the district. The study sample was collected only from the schools as it was feasible. Thus, future studies are recommended for assessment of dental caries and its related factors among non-school going children of the district.
School children of first standard have been selected for the present study considering that the children of the first grade would be 6 or 7 years of age. The WHO recommended index age is 5 and the reason for recommending 5 years is that it is the age of interest in relation to caries in the primary dentition, which may exhibit changes over a shorter time span and it is the age when children begin primary school. However, it has been suggested by WHO that ages 6 or 7 can be used in countries where school entry is late.[13]
The mean dmft accounted to 1.69 approximating the mean dmft value of 5-year-old children of the whole nation[7] (1.8) but is greater than caries experience observed by a previous survey in Udaipur region (0.4) and Rajasthan state[14] (0.7), however it is much lesser than the mean dmft of 3.51 among Chennai school children.[15]
There was a significant difference for the caries prevalence between the genders with greater proportion of boys experiencing caries than girls, similar results were observed in previous studies from India and this difference had been attributed to parents’ exhibiting preferential behavior towards boys in India.[16–18]
Though insignificant, caries experience was higher in children living in rural than urban areas in harmony with the previous studies.[19,20] and this may be explained by differences in dental care habits, social norms and dental attitudes. However, urban school children had significantly greater filled teeth in contrast to no filled teeth in their rural counterparts. This is in accordance to a recent study from North Russia where urban school children had significantly greater filled teeth than rural ones.[21] This difference in filled teeth between the regions might be due to the greater accessibility of dental care in urban than the rural areas.
Parent's occupation significantly altered caries status with children of those parents in better occupations experienced lesser caries and comparable results were observed in a past study.[22] Moreover, similar findings were observed among 5 to 15-year-old school going children of Chidambaram in India where children of low socioeconomic status experience greatest caries.[23]
Parent's level of education significantly influenced the caries experience, a review of risk factors for dental caries in young children associated low father's and mother's education with high caries prevalence.[24]
The proportion of children claiming of brushing twice or more than twice daily was 7.8% which is very less when compared to children of Jordan[25] and Portugal.[19] Very few children paid dental visits and 93.3% had never been to a dentist, which is worse than 58% among Chinese children.[26] Rural children visited the dentist much less often than the urban children (P < 0.05) in agreement with 6-year-old children of Portugal.[19]
Varenee, et al., suggested that urban centers facilitate access to toothbrushes and toothpaste and the use of these hygiene measures are considered a sign of modern life style.[27] Consequently, 6-year-old urban children used tooth brush and tooth paste significantly more than rural individuals. The proportion of 6-year-old children with caries was 58.9% in the present study which is in accordance to the 50% of the national data.[7]
The most important predictors for caries occurrence were place of residence, gender, parent's level of education and brushing frequency. Additionally, visits to dentist significantly influenced caries status in 6-year olds. Thus, caries was related to many socio-behavioral factors in agreement with the previous studies.[28–30]
CONCLUSIONS
Rural children and boys experienced greater caries than their urban and girl counterparts. Caries experience was related to the parent's occupation and education. The present study population exhibited poor oral hygiene habits. Furthermore, caries occurrence was influenced by brushing frequency and dental visiting habits.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Thomas S, Tandon S, Nair S. Effect of dental health education on the oral health status of a rural child population by involving target groups. J Indian Soc Pedod Prev Dent. 2000;18:115–25. [PubMed] [Google Scholar]
- 2.Donahue GJ, Waddell N, Plough AL, Del Aguila MA, Garland TE. The ABCDs of treating the most prevalent childhood disease. Am J Public Health. 2005;95:1322–4. doi: 10.2105/AJPH.2004.057778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mansori Karkavandi T, Tavafzadeh Haghi S, Bouzari M, Bagherzamani A, Farhady A. Dent Res J. North America: 2008. Jan 1, [Last accessed on 2012 Sept 23]. A comparative study of dental caries prevalence in 35-44 and 6-12 year Old Iranian Villagers and Afghan Refugees living in villages of Isfahan province of Iran. Available from: http://www.drj.mui.ac.ir/index.php/drj/article/view/11 . [Google Scholar]
- 4.Zhu L, Petersen PE, Wang HY, Bian JY, Zhang BX. Oral health knowledge, attitudes and behaviour of adults in China. Int Dent J. 2005;55:231–41. doi: 10.1111/j.1875-595x.2005.tb00321.x. [DOI] [PubMed] [Google Scholar]
- 5.Hobdell MH. Economic globalization and oral health. Oral Dis. 2001;7:137–43. [PubMed] [Google Scholar]
- 6.Petersen PE. Sociobehavioural risk factors in dental caries – international perspectives. Community Dent Oral Epidemiol. 2005;33:274–9. doi: 10.1111/j.1600-0528.2005.00235.x. [DOI] [PubMed] [Google Scholar]
- 7.Bali RK, Mathur VB, Talwar PP, Chanana HB. National oral health survey and Fluoride Mapping 2002-2003 India. 1st ed. New Delhi: Dental Council of India and Ministry of Health and Family Welfare, Government of India; 2004. [Google Scholar]
- 8.Sakai O, Tsutsui T, Yagi M, Watanabe T, Warnakulasuriya S. Oral health in Asia. Oral Dis. 1995;1:98–9. doi: 10.1111/j.1601-0825.1995.tb00167.x. [DOI] [PubMed] [Google Scholar]
- 9.Petersen PE, Peng B, Tai B, Bian Z, Fan M. Effect of a school-based oral health education programme in Wuhan city, Peoples Republic of China. Int Dent J. 2004;54:33–41. doi: 10.1111/j.1875-595x.2004.tb00250.x. [DOI] [PubMed] [Google Scholar]
- 10.Klein H, Palmer CE, Knutson JW. Studies on dental caries. I. Dental status and dental needs of elementary school children. Public Health Rep. 1938;53:751–65. [Google Scholar]
- 11.Oral health surveys: Basic methods. 3rd ed. Geneva: WHO; 1987. World Health Organization. [Google Scholar]
- 12.Kumar N, Shekhar C, Kumar P, Kundu AS. Kuppuswamy's socioeconomic status scale-updating for 2007. Indian J Pediatr. 2007;74:1131–2. [PubMed] [Google Scholar]
- 13.Oral health surveys: Basic methods. 4th ed. Geneva: WHO; 1997. World Health Organization. [Google Scholar]
- 14.Bali RK, Mathur VB, Talwar PP, Chanana HB. National oral health survey and Fluoride Mapping 2002-2003 Rajasthan. 1st ed. New Delhi: Dental Council of India and Ministry of Health and Family Welfare, Government of India; 2004. [Google Scholar]
- 15.Mahesh Kumar P, Joseph T, Varma R, Jayanthi M. Oral health status of 5 years and 12 years school going children in Chennai city-An epidemiological study. J Indian Soc Pedod Prev Dent. 2005;23:17–22. doi: 10.4103/0970-4388.16021. [DOI] [PubMed] [Google Scholar]
- 16.Dhar V, Bhatnagar M. Dental caries and treatment needs of children (6-10 years) in rural Udaipur, Rajasthan. Indian J Dent Res. 2009;20:256–60. doi: 10.4103/0970-9290.57352. [DOI] [PubMed] [Google Scholar]
- 17.Rao A, Sequeira SP, Peter S. Prevalence of dental caries among school children of Moodbidri. J Indian Soc Pedod Prev Dent. 1999;17:45–8. [PubMed] [Google Scholar]
- 18.Saravanan S, Kalyani V, Vijayarani MP, Jayakodi P, Felix JW, Arunmozhi P, et al. Caries prevalence and treatment needs of rural school children in Chidambaram Taluk, Tamil Nadu, South India. Indian J Dent Res. 2008;19:186–90. doi: 10.4103/0970-9290.42948. [DOI] [PubMed] [Google Scholar]
- 19.de Almeida CM, Petersen PE, André SJ, Toscano A. Changing oral health status of 6- and 12-year-old schoolchildren in Portugal. Community Dent Health. 2003;20:211–6. [PubMed] [Google Scholar]
- 20.Wong M, Lo LE, Schwarz E, Zhang HG. Oral health status and oral health behaviors in Chinese children. J Dent Res. 2001;80:1459–65. doi: 10.1177/00220345010800051501. [DOI] [PubMed] [Google Scholar]
- 21.Gorbatova MA, Gorbatova LN, Pastbin MU, Grjibovski AM. Urban-rural differences in dental caries experience among 6-year-old children in the Russian north. Rural Remote Health. 2012;12:1999. [PubMed] [Google Scholar]
- 22.Enjary C, Tubert-Jeannin S, Manevy R, Roger-Leroi V, Riordan PJ. Dental status and measures of deprivation in Clermont-Ferrand, France. Community Dent Oral Epidemiol. 2006;34:363–71. doi: 10.1111/j.1600-0528.2006.00284.x. [DOI] [PubMed] [Google Scholar]
- 23.Moses J, Rangeeth BN, Gurunathan D. Prevalence of dental caries, socio-economic status and treatment needs among 5 to 15 year old school going children of Chidambaram. [Last cited on 2012 Jul 09];J Clin Diagn Res. 2011 5:146–51. Available from: http://www.jcdr.net/article_fulltext.asp?issn=0973-709x&year=2011&month=Februar&volume=5&issue=&page=&id=1156 . [Google Scholar]
- 24.Harris R, Nicoll AD, Adair PM, Pine CM. Risk factors for dental caries in young children: A systematic review of the literature. Community Dent Health. 2004;21:71–85. [PubMed] [Google Scholar]
- 25.Rajab LD, Petersen PE, Bakaeen G, Hamdan MA. Oral health behaviour of schoolchildren and parents in Jordan. Int J Paediatr Dent. 2002;12:168–76. doi: 10.1046/j.1365-263x.2002.00359.x. [DOI] [PubMed] [Google Scholar]
- 26.Petersen PE, Esheng Z. Dental caries and oral health behaviour situation of children, mothers and school teachers in Wuhan, People's Republic of China. Int Dent J. 1998;48:210–6. doi: 10.1111/j.1875-595x.1998.tb00479.x. [DOI] [PubMed] [Google Scholar]
- 27.Varenne B, Petersen PE, Ouattara S. Oral health behaviour of children and adults in urban and rural areas of Burkina Faso, Africa. Int Dent J. 2006;56:61–70. doi: 10.1111/j.1875-595x.2006.tb00075.x. [DOI] [PubMed] [Google Scholar]
- 28.Petersen PE, Hoerup N, Poomviset N, Prommajan J, Watanapa A. Oral health status and oral health behaviour of urban and rural school children in Southern Thailand. Int Dent J. 2001;51:95–102. doi: 10.1002/j.1875-595x.2001.tb00829.x. [DOI] [PubMed] [Google Scholar]
- 29.Petersen PE. Oral health behaviour of 6 year old Danish children. Acta Odontol Scand. 1992;50:57–64. doi: 10.3109/00016359209012747. [DOI] [PubMed] [Google Scholar]
- 30.Peng B, Petersen PE, Fan MW, Tai BJ. Oral health status and oral health behaviour of 12 year old urban schoolchildren in the People's Republic of China. Community Dent Health. 1997;14:238–44. [PubMed] [Google Scholar]