

Introduction
Control of sexually transmitted infection (STI) remains challenging in most regions; Latin America (LA) is no exception. The Latin American and Caribbean Association for the Control of Sexually Transmitted Infections (ALAC-ITS)1 implemented a survey to collect information on STI programmes in the region.
This paper highlights some important sexual behavioural trends from recently published literature and presents key results of the survey of STI programmes, identifying weaknesses, strengths and opportunities for STI control in LA.
Methods
ALAC-ITS developed a survey to assess reporting, epidemiology and organisational aspects of STI programmes. The survey was distributed in November 2007 by email to the directors of the national STI programmes in 20 ALAC-ITS member countries. The following 19 countries returned the survey: Argentina, Bolivia, Brazil, Chile, Colombia, Costa Rica, Cuba, Ecuador, El Salvador, Guatemala, Honduras, Mexico, Nicaragua, Panama, Paraguay, Peru, Dominican Republic, Uruguay and Venezuela. Haiti did not respond. The data analysed were shared and validated at a meeting in March 2008, with representatives from 18 national STI programmes, ALAC-ITS, and international agencies. In addition, we have updated information on some countries with data from the national STI programmes and ALAC-ITS members. Data related to syphilis have been published.2 We have complemented the data presented with literature review.
Results
Sexual behaviour in LA
A recent analysis of sexual behaviour around the world revealed that age at first sexual intercourse in LA varies from a median of 16.5 to 17.5 years for men and 15.5 to 17.5 years for women.3 From analyses of demographic and health surveys from eight countries (Bolivia, Brazil, Colombia, Dominican Republic, Guatemala, Nicaragua, Paraguay and Peru) conducted between 1990 and 2000, researchers have found that premarital sexual activity has been increasing.4 There is a trend towards increased uptake of contraception, which varies from 6% for Guatemala to 27% in Colombia. These results also show that condom use increased, although the contribution of condom use to contraceptive protection represents only 10–20% of all contraceptive methods. However, the increase in contraceptive use is not sufficient to decrease the risk of pregnancy due to increased sexual activity, nor other risks associated with unsafe sex (eg, STIs). In 1990, a Brazilian study showed that 30% of sexually active adolescent males from low-income areas reported having had an STI at least once.5 In Peru, from a 2006 population-based survey of asymptomatic men 18–29 years old, we found 28% reported having had urethral discharge, genital ulcers or genital warts in the 12 months before the survey (P J Garcia, personal communication, 2008).
Data on sexual partnerships in LA shows over-reporting of partners by men and under-reporting by women.3 Estimates of proportions of men who have sex with men vary from 6% to 20%.6
Epidemiological situation of STIs
All countries have mandatory reporting of AIDS and HIV infection, except Brazil and Uruguay, which do not require reporting of HIV infection. Mandatory reporting of other STIs, however, varies greatly across countries (table 1).
Table 1.
Sexually transmitted infections for which mandatory reporting is required, LAC region, 2007
|

It is not easy to characterise accurately the epidemiological situation of STIs in the LA region from the data collected by the national STI programmes; in contrast with HIV/AIDS, the surveillance and reporting systems differ considerably from one country to another with regard to definitions—clinical versus syndromic versus laboratory based—and even those using laboratory-based diagnosis differ with regard to the type of tests available.
A total of 539 063 STI cases, including syndromic notifications, were reported by the 19 countries for 2006 (table 2). Compared with 1999 WHO estimates of 38 million new cases of five curable STIs in LA,7 the numbers reported from the national STI programmes represent a very small proportion of the expected incident STI cases. Several STIs are not reported because of difficulties with STI diagnosis and recognition of cases. Studies in LA have shown that private physicians provide a substantial proportion of health delivery for STIs, and such cases are not reported at the national level.8–10 In addition, patients with STI often bypass formal healthcare systems and seek care in the informal sector (eg, pharmacies), as has been documented for LA.11 Members of the national STI programmes of 10 of the 19 countries responding to our survey estimated that 25–50% of STI cases are seen at pharmacies.
Table 2.
Cases of sexually transmitted infection (STI) reported by national STI programmes, LAC region, 2006
| Country | Syphilis | Congenital syphilis | Gonorrhoea | Chlamydia | HSV | Condyloma | Urethral discharge | Vaginal discharge | Genital ulcers | Other | Total |
| Argentina | 672 | 579 | 4046 | – | – | – | 26 510 | – | – | 676 | 32 483 |
| Bolivia | – | – | – | – | – | – | 3841 | – | 7504 | – | 11 345 |
| Brazil | – | 5789 | – | – | – | – | – | – | – | – | 5789 |
| Chile | 2993 | 53 | 1313 | – | – | – | – | – | – | – | 4359 |
| Colombia | 3000 | 773 | 1624 | 5226 | 2190 | – | – | – | – | 8312 | 21 125 |
| Costa Rica | 1040 | 96 | 1287 | – | – | – | – | – | – | – | 2423 |
| Cuba | 1970 | 0 | 5660 | – | – | 4155 | 2423 | 87 024 | – | 81 342 | 182 574 |
| Ecuador | 1885 | 110 | 2962 | – | 1393 | – | 2330 | – | 2073 | 177 | 10 930 |
| El Salvador | 443 | 9 | 1086 | – | 971 | 1018 | – | – | – | 7535 | 11 062 |
| Guatemala | 234 | 5 | – | – | – | 700 | 682 | – | 394 | 42315 | 44 330 |
| Honduras | 626 | 46 | 4366 | 11 998 | 355 | 1176 | 2250 | – | 100 | – | 20 917 |
| México | 2562 | 78 | 1256 | – | 1982 | 24 131 | 35 649 | – | – | 801 | 66 459 |
| Nicaragua | 662 | 5 | 1558 | – | – | 892 | – | – | – | – | 3117 |
| Panamà | – | 16 | – | – | – | – | – | – | – | – | 16 |
| Paraguay | 1065 | 220 | – | – | – | – | 42 | 5281 | 32 | 174 | 6814 |
| Perú | 4521 | 517 | 790 | 719 | – | – | 6117 | – | 4391 | – | 17 055 |
| Dominican R | – | – | – | – | – | – | – | – | – | – | 0 |
| Uruguay | 1415 | 125 | 7 | 654 | – | 31 | 31 | – | – | – | 2263 |
| Venezuela | 3000 | 2 | 10 000 | 20 000 | 10 000 | 15 000 | 20 000 | – | 18 000 | – | 96 002 |
| Total | 26 088 | 8423 | 35 955 | 38 567 | 16 891 | 47 103 | 99 875 | 92 305 | 32 494 | 141 332 | 539 063 |
Organisational aspects of STI programmes in LA
All the countries surveyed reported that STI management is integrated into primary care services. In addition, they reported 241 ‘specialised’ STI clinics in the 19 LA countries. Syndromic management of STIs is now universally accepted as the standard of care throughout the region, although acceptance of this policy took much longer in countries such as Uruguay and Ecuador (2006) than in Brazil (1994). General practitioners, as well as specialists in infectious diseases, gynaecology, urology and dermatology, are responsible for treating STI cases in most of the countries, although nurses and midwives also see and manage cases.12
Most countries reported providing services to all individuals seeking care for an STI through ministry of health clinics, where consultations for STIs are free of charge for any patient (general or high-risk population) in 14 of 19 countries and STI drugs are offered free of charge in 17 of 19 countries (Colombia and Uruguay do not offer free treatment for STIs). Paraguay and Bolivia reported that condoms are not regularly offered as part of STI management.
All countries except Colombia, El Salvador and Paraguay offer partner notification services. Most of the countries (12 of 19) have implemented partner notification solely by asking patients to notify their partners; only four used a combined patient and health provider notification strategy. National STI programme staff estimated that notification reaches <25% of the partners in STI cases.
STI screening and services for specific populations
As shown in table 3, STI screening is almost universal for female sex workers (conducted in 16 of 19 countries) and mostly includes HIV and syphilis testing, although five countries also report screening for gonorrhoea. STI screening of pregnant women is also common and includes syphilis and HIV testing. STI screening for other groups is less common.
Table 3.
Sexually transmitted infection (STI) screening and services available for specific populations, LAC region, 2007
|
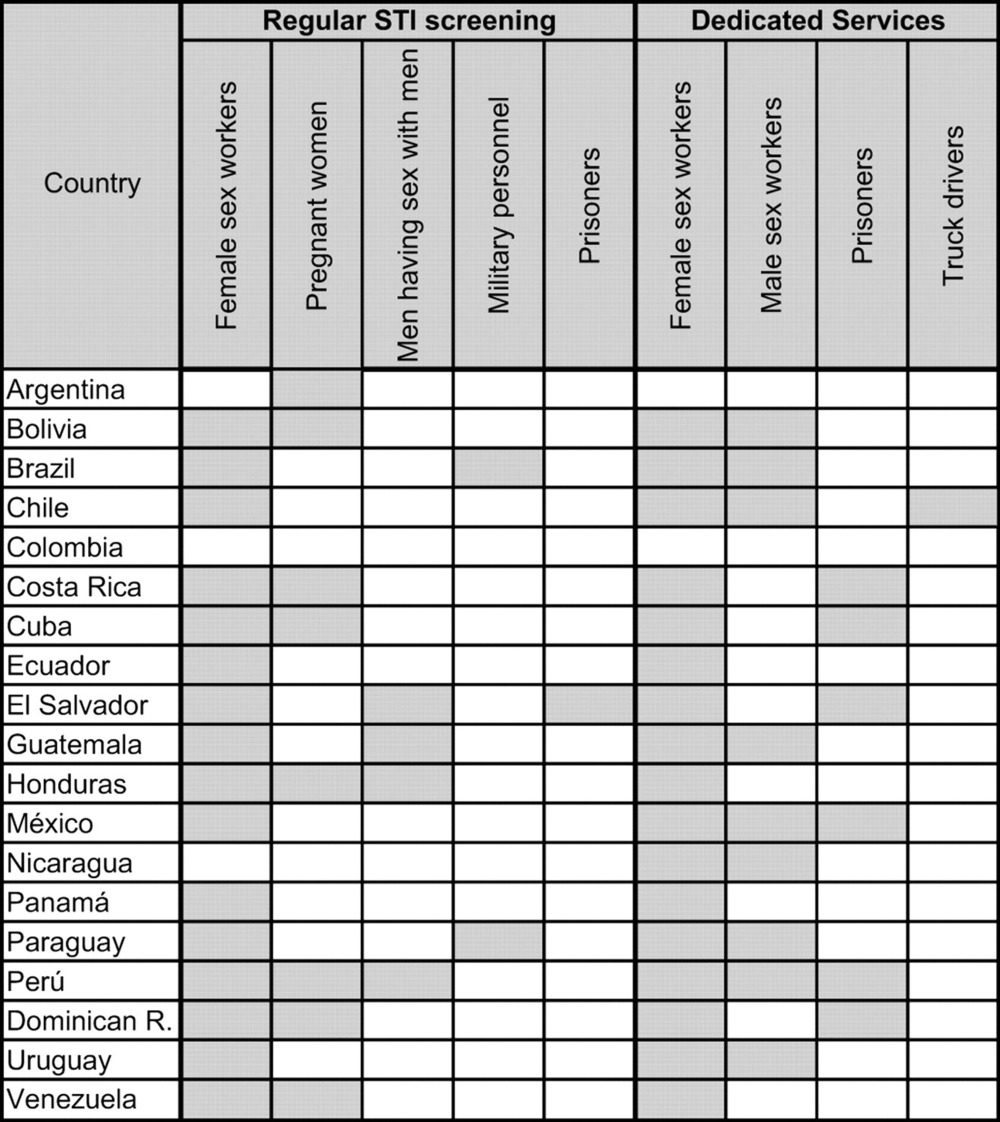
Dedicated STI services for specific populations are also common in the LA region, and were reported by all countries except Colombia—which provides no differentiated care—and Argentina—which did not respond to the question. Female sex workers are the most common beneficiaries of differentiated services, although there are also services for male sex workers, prisoners and truck drivers in some countries.
Antibiotic resistance and Neisseria gonorrhoeae
Only nine of the countries surveyed (47%) have implemented surveillance of resistance of Neisseria gonorrhoeae strains to antibiotics currently used. In the region, strains resistant to penicillin and tetracycline are widely disseminated, and strains with intermediate resistance to ciprofloxacin are also circulating. Four countries, Chile, Costa Rica, Mexico and Panama, no longer recommend ciprofloxacin for gonococcal infections; instead, the current recommendation is ceftriaxone, which is much more costly and logistically more difficult because it requires parenteral administration.
Discussion
Under-reporting of STIs is extremely common in national STI programmes in LA, and there is no regional consensus on what STIs to report and how to report the STI data. STI syndromic management is being used in all the countries surveyed, and there are specialised clinics for STIs across LA, with different types of clinicians (medical doctors with and without appropriate specialties and other health providers such as nurses and midwives) offering STI management. This diversity represents an important strength. However, costs and availability of condoms differed between countries, and there are major issues about partner notification. Services for different populations such as sex workers (female and male), prisoners and truck drivers have been implemented in some, but not all, countries.
The current state of STI control in LA shows that advances have been made and that new and continuing challenges lie ahead. There is great potential for learning from each other in the LA region, to share lessons learnt, improve information and surveillance systems, and move towards the provision of better STI prevention and care services in the region.
Key messages.
STI control remains challenging in the Latin American (LA) region.
The increase in contraceptive use in LA (including condoms) is not sufficient to decrease the risk of pregnancy due to increased sexual activity, nor other risks associated with unsafe sex and STIs.
Under-reporting of STIs is extremely common in national STI programmes in LA, and there is no regional consensus on what or how STIs are reported.
HIV reporting is similar across the countries studied, but STI reporting is highly variable.
STI syndromic management is used in all countries surveyed, partner notification is low, and condom availability differed by country.
Footnotes
Competing interests: None.
Contributors: PJG wrote the manuscript and contributed to the development of the initial survey instrument and the analysis of the data presented. ASB contributed to the development of the survey instrument and the writing of the manuscript. EG designed and analysed the initial survey. Members of ALAC-ITS contributed data. All listed authors contributed to the preparation of the manuscript.
Provenance and peer review: Commissioned; externally peer reviewed.
References
- 1. Ross JD, Garcia PJ, Zenilman J, et al. Summary of proceedings of the IUSTI Global Challenges Symposium (ISSTDR 2007/10th IUSTI World Congress). Int J STD AIDS 2009;20:130–4 [DOI] [PubMed] [Google Scholar]
- 2. Galban E, Benzaken A. Situación de la sífilis en 20 países de Latino América y El Caribe: año 2006. DST-J Bras Doencas Sex Transm 2007;19:166–72 [Google Scholar]
- 3. Wellings K, Collumbien M, Slaymaker E, et al. Sexual behaviour in context: a global perspective. Lancet 2006;368:1706–28 [DOI] [PubMed] [Google Scholar]
- 4. Ali MM, Cleland J. Sexual and reproductive behaviour among single women aged 15-24 in eight Latin American countries: a comparative analysis. Soc Sci Med 2005;60:1175–85 [DOI] [PubMed] [Google Scholar]
- 5. Childhope. Gender, sexuality, and attitudes related to AIDS among low income youth and street youth in Rio de Janeiro, Brazil. New York, NY: Childhope, 1997 [Google Scholar]
- 6. Cáceres C, Konda K, Pecheny M, et al. Estimating the number of men who have sex with men in low and middle income countries. Sex Transm Infect 2006;82(Suppl 3):iii3–9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. World Health Organization, Department of HIV/AIDS Global Prevalence and Incidence of Selected Curable Sexually Transmitted Infections: Overview and Estimates. Geneva, Switzerland: World Health Organization, 2001. WHO reference number: WHO/HIV_AIDS/2001.02 and WHO/CDS/CSR/EDC/2001.10. [Google Scholar]
- 8. Hanson K, Berman P. Private health care provision in developing countries: a preliminary analysis of levels and composition. Health Policy Planning 1998;13:195–211 [DOI] [PubMed] [Google Scholar]
- 9. Garcia PJ, Holmes KK. STD trends and patterns of treatment for STD by physicians in private practice in Peru. Sex Transm Infect 2003;79:403–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Hsieh EJ, Blas MM, La Rosa Roca S, et al. Sexually transmitted infections and private physicians in Peru, 2003. Rev Panam Salud Publica 2006;20:223–9 [DOI] [PubMed] [Google Scholar]
- 11. García PJ, Cárcamo CP, Chiappe M, et al. Sexually transmitted and reproductive tract infections in symptomatic clients of pharmacies in Lima, Peru. Sex Transm Infect 2007;83:142–6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Hsieh EJ, García PJ, Roca SL. Male midwives: preferred managers of sexually transmitted infections in men in developing countries? Rev Panam Salud Publica 2008;24:271–5 [DOI] [PubMed] [Google Scholar]