

Abstract
Introduction
Junctional spinal disorders have become one of the greatest challenges in spinal deformity surgery. They can occur at any age but are mostly seen in adult deformity surgery and are most often observed as the patient gets older.
Definitions
Different forms can be individualized according to their types and location: one can observe simple segmental degeneration above or below instrumentation with or without spinal stenosis. Or the situation may be more complex with proximal junctional kyphosis, distal junctional kyphosis and intercalary junctional kyphosis where the junctional kyphosis occurs between two instrumented segments of the spine. Junctional scoliosis may also be observed as a new curve that did not exist after the index surgery.
Pathophysiology
Many different factors have been described being associated or the cause of junctional problems: old age, increased BMI, osteoporosis, etc. The role of pre-existing and postoperative sagittal imbalance plays a definitive role in their pathogenesis. As well the weakened posterior elements and or fatty degeneration of the posterior muscles are key factors in the occurrence of these problems. Multiple different radiologic parameters to describe and achieve perfect sagittal balance have been described knowing that the pelvic incidence of the patients is the key element that governs lumbar lordosis of the patient and hence the sagittal balance. Away from the spine one has to integrate the issues of the knees and the hips in the presentation of these junctional problems whether they are the cause or one of the consequences of the sagittal malalignment. Likewise the non-instrumented part of the spine (thoracic and or cervical spine) will also play a role in the pathogenesis or prevention of these junctional problems if they are stiff and or autofused along with their respective deformity.
Treatment
To prevent the occurrence of such junctional problems some basic surgical rules must be observed, but still lots remain unknown such as how much restoration of lordosis is really necessary, how to create a smoother transition between the instrumented and non-instrumented spine, which metal and where to use it, which implants to use as our widely used pedicle screw system may be one of the causes of these problems. Clinically these junctional problems can be asymptomatic and require only observation, or require revision surgery. Revision will require in most cases decompression of the neural elements, extension of the instrumentation and spinal osteotomies.
Conclusion
Definitively the issue of junctional spinal disorder after deformity surgery will require further extensive research to minimize this problem especially in our aging population.
Keywords: Junctional spine disorder, Adult spine deformity, Adult scoliosis, Proximal junctional kyphosis, Distal junctional kyphosis, Intercalary junctional kyphosis, Scoliosis complications
Historic and natural history perspectives
Surgery for scoliosis is no longer restricted to the pediatric age group. In the adult and/or elderly patients, de novo scoliosis has become an increasing problem. The incidence of degenerative scoliosis ranges from 29 % at age 54 and can get as high as 68 % in the population of 70 years [1, 2]. With the aging of our population and the increased demand in spinal surgery from our patients who want to live longer and want to lead a more comfortable life, spinal deformity surgeons operate on more and more elderly patients. With the advent of new technologies, stronger, however, more rigid instrumentation, powerful osteotomies, along with the degenerative process, we have been faced over the last decade with a new disease called adjacent segment disease after spinal deformity correction. In our classification of adult scoliosis in four different groups we had published 8 years ago, we subclassified the postsurgical scoliosis pathologies in the type 3 [3]. The purpose of the paper is to further define these adjacent segment pathologies after deformity surgery and give a better understanding of their causes, their prevention and treatment.
Definition (JD, PJK, DJK, IJK, JS)
The junctional spinal deformities (JD) can occur in young or pediatric patients, who have been treated usually for adolescent idiopathic scoliosis or Scheuermann’s kyphosis [4]. Such junctional problems are most of the time asymptomatic and observed early after the surgery and are often the results of surgical mistake such as improper selection level not encompassing the whole deformity, stopping short of the stable vertebra, disruption of anatomic structures or too much correction of deformities. In other cases these junctional problems can happen several decades after the index surgery and are related to progression of the curve above or below the instrumented or fused spine along with the degenerative process (Fig. 1). Elderly patients can develop junctional disease (JD) after the treatment of adult deformities and multisegmental degenerative disease. A junctional kyphosis may occur in the adjacent proximal part to a stabilised spinal area, this is called proximal junctional kyphosis (PJK) and it has been defined as 15° or more of angulation above a previous instrumentation (Fig. 2). However, there is definitively also JD happening usually in the form of a distal junctional kyphosis (DJK) either in the bone (Fig. 3) or in the adjacent disc(s) or both or as loss of lordosis (or segmental instability below a fixed spinal area) of the lumbar spine (Figs. 1, 3). In this part of the spine it concerns usually a lumbosacral adjacent problem with stenosis. This can be observed with or without junctional scoliosis (JS). At last an entity that has not been coined so far is the intercalary junctional kyphosis (IJK): this is observed in patients with two instrumentations that are not connected together: the non-instrumented spine (whether fused or not fused) in between the two instrumentations will fail either acutely or progressively because of the differential stiffness between the bone or ligaments alone and the instrumentation above or below. This may happen acutely or progressively or in the phase or progressive osteoporosis (Fig. 4). Finally, it is not rare to observe a combination of junctional problems in the same patient.
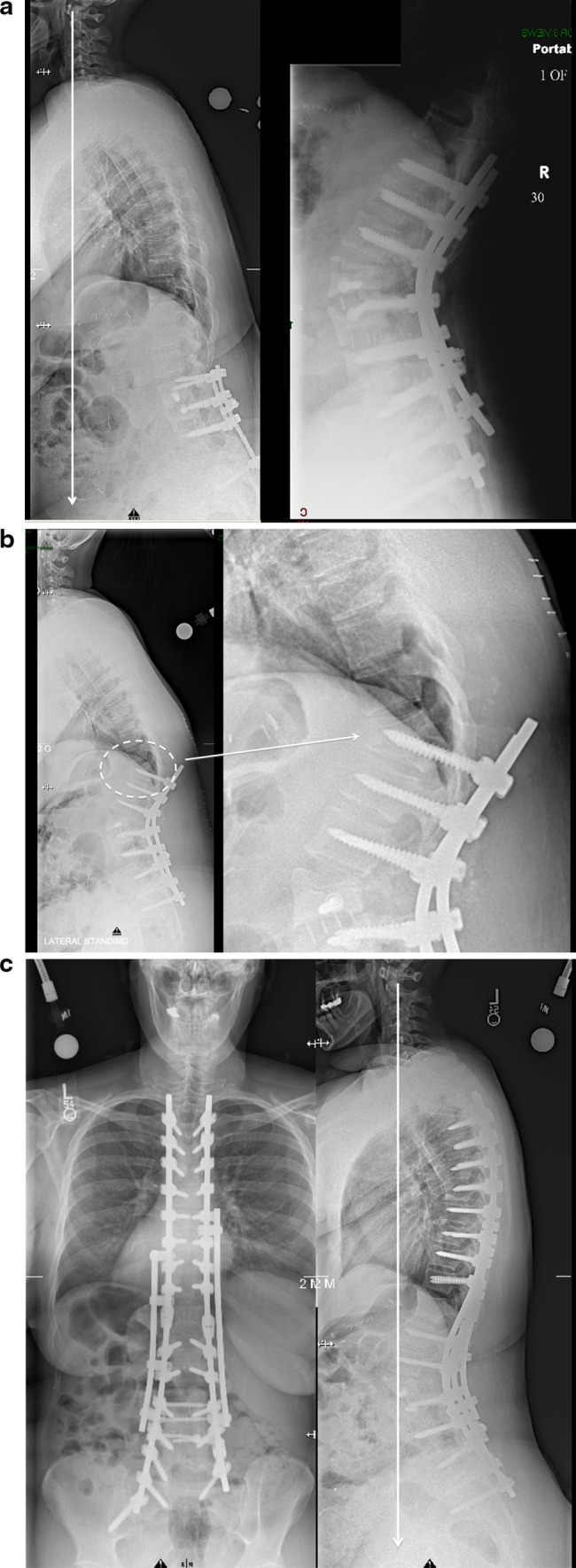
Fig. 1.

Junctional scoliosis with degeneration below a previous fusion. a 56-year-old patient with previous scoliosis surgery 25 years before complaining of severe leg pain, back pain and inability to stand up straight. b Below the fusion that extended to L4, one can see severe facet arthropathy; on the lateral x-rays there is loss of lumbar lordosis. The myelogram confirms the spinal stenosis (white arrow). c Surgery with extension of the instrumentation to the pelvis, TLIF and Smith Petersen osteotomies to restore the lordosis. Good sagittal and coronal balance
Fig. 2.
Proximal junctional kyphosis (PJK). a Flat back syndrome after multiple low back surgeries in a 45-year-old obese patient: treatment of the sagittal imbalance with a pedicle subtraction osteotomy at L2. Observe the rods left slightly longer proximally as though PJK was an anticipated risk. b 2 weeks postoperatively, patient feels a crack in her back: X-rays shows a proximal junctional kyphosis with fracture through the pedicle of T11 (dashed circle left and magnifiedpicture right). c Treatment with extension of the fusion proximally with end to end connectors and a four rods construct because of the increased BMI of the patient
Fig. 3.

Distal junctional kyphosis (DJK). a 32-year-old female with a history of ankylosing spondylitis and progressive thoracic kyphosis. b Treatment with multiple transdiscal osteotomies and one PSO at the apex of the thoracic curve: good restoration of sagittal profile. c 6 months postoperatively: progressive loss of reduction with distal junctional kyphosis (dashed circle). The instrumentation should have been extended down to L3 that was the stable sagittal vertebra. d Treatment with extension of the instrumentation to the sacrum and a new PSO at L3: good restoration of the sagittal balance
Fig. 4.

Intercalary junctional kyphosis (IJK). a 62-year-old patient with a history of scoliosis surgery 30 years ago and lumbosacral fusion 10 years ago: Progressive flat back deformity and kyphosis in the intercalary segment that was not instrumented (Dashed circle). b Correction with first stage: anterior 5/1 fusion with wedge allograft, second stage PSO at L2 and connection to the previous Harrington rod (the left iliac screw broke at 1-year follow-up and was asymptomatic)
Prevalence of junctional disease
There are some figures from statistics available concerning the proximal but not so much the DJK. The exact incidence of PJK is difficult to ascertain. In a recent study out of 1,218 cases, the incidence of PJK was determined as 5.8 % [5]. However, other studies, specifically in adult idiopathic scoliosis, have reported an incidence of 20 % [6] and after a certain type of spinal osteotomies the incidence has been reported to be 23 % [7]. Most series, however, deal with a fairly young population and obviously, as the patients get older the risk of junctional kyphosis after spine surgery is increased. Kim [8] observed a rate of 59 % of PJK in patients over the age of 55. The rate of DJK was reported to be 6.8 % after fusion for AIS at 2 years postop, however, the series was mostly a pediatric population [9]. Of interest would be to know indeed the real incidence of the proximal as well as the DJK in correlation with increasing age. The rate of JS below or above an instrumented fusion has so far not been reported. However, this is more likely to occur over time if the instrumented part of the spine was left with some imbalance. The rate of IJK has not been reported either. However, the more osteopenia or osteoporosis the more likely it will happen. In our experience of treating elderly patients (older than 70 years old) junctional kyphosis or at least some JD is observed regularly after long instrumentation.
Clinical and radiological presentation of different forms of junctional pathology
There are different modes of clinical presentation and failure, which can be visualised, in the imaging evaluation of the patient (standing X-rays with knees in extension, flex—ext X-rays, traction films, CT, MRI). Very little correlation has, however, been found between the clinical symptoms and the presence of radiologic evidence of JD whether it is PJK, DJK, IJK or JS. Each case has to be individually assessed with its clinical implications away from large statistical series that usually do not apply to a specific situation. We have summarized the most common failures modes and their characteristics in Table 1.
Table 1.
Characteristics and localization of different failures modes

PLC posterior ligament complex, VCF vertebral compression fracture, UIV upper instrumented vertebra
The proximal junction failure mode
A progressive deformity above a previous instrumentation that corresponds to the natural history of progressive kyphosis as observed in natural aging: This is related to loss of disc space height, and mild and uniform wedging of the vertebral bodies above (Fig. 5). This may or may not be painful, whether compensated or decompensated and may happen over a long period of time or quite rapidly after surgery.
An elongation through stretching of the posterior ligament complex without its disruption as often observed in young patients with good bone stock: One will often observe an acute wedging of the disc above the instrumentation. This may, however, lead over time to further progressive kyphosis.
A disruption of the posterior ligament complex (ligaments and capsules) (Fig. 6). This may lead along with the deformity to spinal stenosis enhanced by a secondary disruption of the posterior annulus of the disc with consecutive instability and even possible disc herniation, sometimes in the form of a massive prolapse of the whole disc fragments. Often the stenosis is also additionally aggravated by the hypertrophy of the posterior elements (ligamentum flavum, facet joint capsules and hypertrophy of the arthritic facet joints) (Fig. 6). The spinal stenosis can be of dynamic nature or it can be a fixed structural spinal stenosis. However, most of these anterior column failures are going together or are even preceded by a failure of the posterior tension banding system due to aging and degeneration of soft tissue like the ligaments, joint capsules and rupture of the posterior annulus of the disc as well as a concomitant weakness of the paravertebral muscles which may be characterised by fatty degeneration (in the extreme leading to camptocormia) or scarring from previous surgeries.
A fracture (often osteoporotic) mostly in combination with disrupted posterior ligament complex. The fracture may take the form of a wedge compression fracture of the upper instrumented vertebra (Fig. 7). The osteoporotic fracture may not only be limited to either the most proximal vertebral body which is included in the fixation, but also to the vertebral body above or several vertebral bodies above (Fig. 8). In rare cases the fracture can occur through the pedicles (Fig. 2).
Failure of the proximal vertebral fixation in the form of screw pull out, screw ploughing in the vertebral body or cutting out into the disc space (Fig. 6)
In some cases the junctional deformity takes the form of a dislocation of the spine above (most often) or below the instrumentation with possible neurologic complications (Fig. 9).
Fig. 5.

PJK related to natural history of progressive kyphosis as observed in natural aging: a degenerative scoliosis in 63-year-old obese female (fusion T10 pelvis). b Two years after decompression laminectomy instrumentation fusion T10 pelvis, one can observe a thoracic Cobb of 60°, patient pelvis is not retroverted, the plumb line is still behind the femoral heads. c Six years later the patient is now 69, there has been an increase in the PJK: Cobb is measured 80°. The patient remains asymptomatic, yet there is some imbalance with the plumb line falling in front of the femoral heads. The increased thoracic kyphosis parallels the ones observed in natural aging
Fig. 6.

PJK with failure of posterior ligament complex. a 62-year-old female, overweight, four previous lumbar spine surgeries: seen for intractable and leg pain and inability to stand straight. Notice the failure of the posterior ligament system (white arrows). b MRI and CT demonstrates the failure of the PLC with facet incompetency, spinal stenosis and end plate failure on both sides at L2/L1. There is also atrophy of the posterior musculature. c Treatment with posterior vertebral column resection, and instrumentation T3 to the sacro-pelvis [note the new PJK at T3 with cut out of the proximal screw in the disc space (dashed circle and white arrow), hopefully only mildly symptomatic]
Fig. 7.

PJK and fracture of the UIV (wedge compression fracture). a 60-year-old female with a history of multiple previous spine surgeries, osteoporotic compression fractures and sagittal decompensation. b Treatment with pedicle subtraction osteotomy at L2 and PSF sacrum to T10 (left). 2 weeks after surgery fracture of the UIV with wedge compression fracture (dashed circle and triangle) (middle and right picture). c Treatment with extension of the instrumentation to the upper thoracic spine: note the new PJK at the cervicothoracic junction (white arrow) (patient had some lower cervical pain)
Fig. 8.

Proximal and distal junctional disease, creation of a smooth transition. a 77-year-old patient, Parkinson, with previous circumferential surgery L3–L5 severe back and leg pain and inability to stand straight. b CT confirms the proximal and distal junctional disease with gas in the disc space at L2–L3 and L5–S1 (arrows left picture). MRI shows proximal junctional kyphosis with end plate fracture at T12 and L1 at distance from the L3–L5 fusion (arrows right picture). c Treatment with posterior fusion T10 pelvis with cement augmentation of the pedicle screws at T10, T11, T12 and L1 (arrows) (left picture). A few months later PJK with VCF of T10 and spinal stenosis (arrow on right). d Revision with extension to the upper thoracic spine using mostly sublaminar wires to decrease the stiffness of the instrumentation
Fig. 9.

PJK and fracture dislocation of the spine. a 56-year-old patient with a history of chronic steroid use and rheumatoid arthritis. Had previously undergone two surgeries: one for flat back deformity, and the previous one for PJK at the level of the TL junction that required extension to the upper thoracic spine. b Two months after her instrumentation: develops weakness in her legs CT scan shows a dislocated spine at the upper part of the instrumentation (dashed circle and arrow). c Surgery will be reduction of the dislocation extension of the fusion to the cervical spine: neurologic recuperation
The distal junctional failure mode
Progressive loss of lumbar lordosis, loss of disc height with disc degeneration: this may happen over years and can involve several segments of the lumbar spine: this is the typical description of the flat back syndrome after long Harrington instrumentation; this may or not be associated with spinal stenosis and increased lumbosacral curve (Fig. 1).
Acute wedging in the disc below the instrumentation: Often observed when the instrumentation stopped short of the first lordotic disc or at distance from the stable sagittal vertebra (Fig. 3) [4].
Fracture of the most distal instrumented vertebra that involves in most cases the inferior endplate.
Similar to the PJK there may be an osteoporotic fracture below the long rigid fixation, usually in the lower lumbar spine, and may also involve the sacrum with sacral insufficiency fracture or a fracture of the pars interarticularis below the fusion mass.
Failure of the instrumentation at the most distal level: This can be observed at all the levels, but is more often encountered at L5 [10]. This may raise the issue of stopping the fusion at this level instead of the sacrum specifically in extra long instrumentation and or in osteoporosis.
Spinal stenosis and or segmental instability underneath the instrumentation as described in the paragraphs above. Retrolisthesis or anterolisthesis of the whole instrumented spine may be observed (Fig. 8).
The intercalary junction failure mode
If the spine is not fused between the two instrumentations: a progressive kyphosis will be initially ligamentous, then destruction of the adjacent vertebral bodies usually follows. If the spine is fused between the two instrumentations: a progressive bent of the fusion mass or an acute fracture that can happen at any place between the two instrumentations or at the level of the lower instrumented or upper instrumented vertebra (Fig. 4). Another situation is an instrumentation that stops in a previous fusion mass and does not bridge the whole fusion mass: The risk is to observe progressive bending or acute fracture of the fusion mass where there is no instrumentation (Fig. 10).
Fig. 10.

Fracture through fusion mass below instrumentation. a 72-year-old female, 3 previous spine surgeries over 10 years. Patient has a L3 S1 fusion and instability/stenosis at L3/L2 and L2/L1 as well as lack of lordosis. b Posterior fusion with instrumentation down to L4 (L5 and S1 were not instrumented because the fusion was solid): 2 months after the surgery: acute pain: CT shows the fracture through the inferior aspect of L4 through the fusion mass (white arrows). c Revision and extension to S1
With better understanding of the significance of the sagittal alignment for the overall balance of the spine and the outcome of surgical corrections, it became obvious that many of these proximal, intercalary and distal junctional pathologies have a lot to do with a deficient observation of a physiological balance of the whole spine of an individual patient as expressed in the so-called spinosacral angle or other global descriptions of good sagittal alignment, like the positioning of the spinovertical axis (SVA) in relation to the posterior corner of the sacral endplate that should be less than 6 cm [11].
Risk factors for junctional kyphosis
In addition to an unfavorable sagittal alignment multiple other conditions and causative factors can be associated with the proximal as well as the DJK and pathology: we present the listing of the different causative factors from our experience or from the literature. A recent systematic review of the literature was published for risk factors and PJK [12].
From this review it appears that independent risk factors for PJK were older age, posterior fusions to the sacrum, combined anterior/posterior surgery, thoracoplasty, and an upper instrumented vertebra at T1–T3. Postoperative hypokyphosis as well as hyperkyphosis were associated risk for PJK. Despite the presence of PJK, no differences were noted in health-related quality of life outcomes.
From our experience we think that other factors contribute to PJK and clinical problems. Obesity, fatty degeneration of paravertebral muscles and consecutive lack of posterior tension banding forces, specifically when combined with poor quality and age-dependent posterior ligament complex (interspinous ligaments, supraspinous ligaments, joint capsules, ligamentum flavum, posterior annulus of the disc). Osteoporosis and/or osteopenia obviously go along with aging but can be observed in younger patients and are for us definitively a risk factor as well as patients on long standing steroids who have weakened posterior elements as well as bone. Neurologic situations (i.e., Parkinson) are also risk factors. Stopping the instrumentation at T1–T3 may increase from the published series the rate of PJK. However, in most cases this does not represent a clinical problem as opposed to stopping the fusion lower down (i.e., at T5 or T6) with more pronounced PJK and possible requirement of revision. Stiff instrumentation, with too rigid constructs with exclusive usage of pedicle screws from the pelvis up to the top of the construct is definitively a risk factor. At last an interesting concept reported by Lewis is the increased upper instrumented vertebra angle as defined on the intraoperative x-rays. This seems logical as if the tilt of the UIV is too much pronounced, all gravity forces will concentrate on the antero-superior aspect of the UIV instead of having a homogenous repartition on the whole superior endplate [13].
For the DJK some risk factors have been indentified in the literature and in our experience. Stopping short of the Cobb angle or short of the first lordotic disc or even at a distance fro the sagittal stable vertebra [4, 14] (Fig. 4). Stopping the fusion at L5 with risk of either fracture of L5 or pull out of the screw especially in elderly is a cause of DJK [15]. Stopping the instrumentation in S1 without protecting it with iliac screws expose to sacral insufficiency fracture and DJK.
Definitively, all these risk factors become more relevant when they coexist together or, when there is a pre-existent malalignment of the spine in the sagittal plane in the form of an already existing kyphosis. Likewise undercorrection of the deformity with insufficient correction of the kyphosis of one of the spine sections (thoracic, thoracolumbar as well as lumbar spine) will expose to PJK. This may occur in the form of a spinosacral angle lower than 125° or a positive SVA of more than 6 cm. Overcorrection of the lumbar lordosis will result in a spinosacral angle of more than 143° or a negative SVA, and this may end up with a compensatory kyphosis of the thoracic spine and consecutive vertebral compression fractures in case of co-existing osteoporosis [16]. Overcorrection as well as undercorrection may also end up with a distal junctional disorder: Massive prolapse of the L5/S1 disc and lumbosacral kyphosis with an unstable junction may be the result.
How much does the amount of pelvic incidence determine the risk of a secondary decompensation is difficult to predict, however, the pelvic incidence is a constant individual parameter, which does barely change during life. There is a direct correlation between the lumbar lordosis and the pelvic incidence. The pelvic incidence is about the amount of lumbar lordosis, respectively the lumbar lordosis should be about equal to the pelvic incidence ±10°. Therefore, a high pelvic incidence usually predicts a higher lumbar lordosis. A higher lumbar lordosis, again, triggers a bigger thoracic kyphosis. If the lumbar lordosis is relevantly decreased in a patient with a high pelvic incidence, then the thoracic spine is unable to compensate, specifically in elderly patients, as rigid osteophytes of the spine may fuse it. This may lead inevitably to an anterior translation of the center of C7 with a SVA highly positive (far beyond 6 cm). This may be initially compensated by a hip extension (relative to the retroverted pelvis). If there is not enough of hip extension reserve then patient will require flexing his knees to maintain his sagittal balance [17]. Le Huec [18] has given an excellent description of the sagittal imbalance and the degenerative cascade and its compensation mechanisms. We also refer to Roussouly [19] paper in this issue for the relevance of the PI in adult scoliosis and the compensation mechanisms of the spine.
Treatment concepts
The indication for treatment needs to be related to the different causes. Is it mostly a neurologic problem with spinal stenosis or is it a problem of the overall sagittal or/and frontal balance or both? Is it primarily a failure of the bony anterior column in the form of vertebral compression fractures due to weak bone and osteoporosis? Is it a failure of the posterior ligament complex? Or is it a combination of all the above?
Prevention
Many of those raised issues can be already approached prophylactically in order to avoid the occurrence of this pathology.
Factors that cannot be influenced by the surgeon
There are factors that cannot be changed by a surgeon. Such factors, which may be addressed already during the first surgery or before in a sense of prophylactic measures to overcome the risk of long fixations are:
Increased body mass index
It has been shown in our experience to correlate with the incidence of PJK. Obviously, larger stress on the top or at the bottom of the instrumentation may expose to increased load at the end of the fixation and therefore the proximal or distal junction. Yet this was not demonstrated in the literature definitely. However, observational experience shows that patients that are overweight, specifically elderly women, who may even have big breasts, have a higher tendency to go into a PJK (Figs. 2, 5 and 6). Furthermore, very often in these obese, mostly female post-menopausal patients there is definitively a fatty degeneration of the paravertebral muscles with a loss of strength and an increasing inability to erect the spine in physiological lordosis (within the worst scenario a camptocormia presentation).
Decreased bone mineral density
Osteoporosis leads to spontaneous vertebral compression fractures. It is therefore not unreasonable to assume a higher rate of PJK or distal JD in long instrumented fusions of the spine (Fig. 7). However, in most cases where surgery is needed, there is limited time to increase bone mineral density through pharmaceutical agents. Therefore, some of these patients may need prophylactic augmentation of their vertebral bodies, which are exposed to higher loads, even outside of the spinal fusion (Fig. 11). With the tendency of anterior load shift with a positive value of the sagittal vertical axis bigger than 6 cm, the vertebral bodies are increasingly loaded and therefore through creeping of this weakened bone subchondral fractures may occur with gradual compression of the vertebral body in a wedge form with a consequent development of kyphosis.
Fig. 11.

Creation of a smooth transition with vertebroplasties and hook. a 75-year-old patient with multiple previous surgeries intractable back and leg pain and inability to stand straight. b First stage is anterior femoral wedge allograft at 5/1, second stage 2 days later with posterior fixation T10 pelvis. c Close up view of the smooth transition creation: The T11 screws are inserted in a down going fashion and embedded in the cement above and around. Above in T10 only a supralaminar hook is inserted. At last above the instrumentation at T9 a prophylactic vertebroplasty is carried out
Old age with consequently weaker ligaments due to degeneration
This goes usually along with increased osteoporosis but old age goes also along with weaker ligament structures and capsules. Likewise, old age is often associated with increased overall kyphosis. A PJK may therefore only reflect a natural history of the aging spine under some circumstances and can even be very well tolerated, as we have observed (Fig. 5), when sufficient compensation mechanisms are present. What is known on the other hand is the natural tendency of the body to go back to the alignment position as prior to the surgery. Whether this phenomenon takes place in the brain of the patient is not known (Fig. 12).
Fig. 12.

PJK happening at a distance in the cervical spine. a 71-year-old female patient with degenerative scoliosis and sagittal and coronal imbalance. b After correction of her sagittal and coronal imbalance with S1 T10 fusion: good restoration of her balance. However, the 3 months lateral X-rays show the beginning of subluxation C3/C4 and at 10 months postop one can observe sagittal decompensation and cervical kyphosis observed with significant pain. c Close up view: C2–C3 is spontaneously fused, the segment C4–C7 severely osteoarthritic and stiff, the thoracic spine was also stiff. d Treatment with posterior cervical fusion C2–C5
Multiple previous surgeries: Definitively this represents a risk factor as the posterior musculature is either absent or has been replaced by scar (Fig. 6).
Different pelvic incidence (PI)
The issue of pelvic incidence and sagittal balance is a hot topic and there is in this special issue a whole paper from Roussouly that covers this complex problem. In his review of adult scoliosis it was found that in patients who had low PI it was easier to achieve sagittal balance after surgery [19]. Likewise Lonner [20] has shown that amongst patients with PJK the magnitude of the junctional kyphosis correlated directly with the degree of pelvic incidence after Scheuermann’s correction. Another paper shows that after PSO of the lumbar spine, one would observe frequently an increase in the thoracic kyphosis that would negatively affect the sagittal alignment. This was more likely to happen with patients with high pelvic incidence (high pelvic incidence = high lordosis) [21].
Intuitively, one may think that patients with a high pelvic incidence and therefore a snakier spine (with more lumbar lordosis) may be more prone to PJK than patients with low pelvic incidence. In other words, if a patient was born with small sagittal curves (low pelvic incidence), his lumbar lordosis and thoracic kyphosis will be of small values. If for any reason an instrumented fusion has to be done up to the thoracolumbar junction, the spine above with limited amount of natural kyphosis is less likely to go into further kyphosis (hip parameters). This is specifically true, when the thoracic spine still has some potential to correct into lordosis.
Hip and knee parameters
Little attention has been given to hip parameters and junctional kyphosis. We all know the difficulty to ascertain a hip flexion contraction in the presence of a rigid and/or fixed lumbar spine in a situation of kyphosis. To some degree what appears clinically as a flexion of the hip may correspond to a situation of hyperextension of the hips but with a kyphotic lumbar spine. With the advent of long standing films from the occiput to the ankles it is, however, now possible to assess the amount of hip flexion contracture and the available hip extension reserve. If there is a true hip flexion contracture the sagittal balance of the patient will remain stooped forward even after reconstruction. If the available extension of the hips along with the lumbar lordosis is not sufficient, a global flexed situation of the spine may occur and proper sagittal alignment may never be achieved.
Hosman [22] was the first to report on the issue of tight hamstrings and postoperative imbalance in patients who had surgery for Scheuermann’s kyphosis. Patients who had tight hamstrings were judged as lumbar compensators. In other words, the patients who had tight hamstrings had to compensate more in the lumbar spine after correction of the kyphosis. In the adult spine, no literature has addressed this issue of patients with tight hamstrings and flat back. Lazennec [17] recently gave a very thorough description of the relationship between the hip parameters and the overall sagittal balance of the patient. The situation can become very complex with the presence of hip or knee osteoarthritis, or total joint replacement with mixed pathologies (true hip flexion contracture or knee flexion contracture) and their implication on the sagittal balance.
Cervical spine and the upper thoracic non-instrumented spine
After looking at the foundation of the spine and the pelvic incidence and the lumbar lordosis, one should take a close look at the cervicothoracic spine that was not instrumented (Fig. 12). No literature has so far addressed this issue, although the recently published literature shows illustrative cases, where the junctional kyphosis of the upper thoracic spine is obvious. This may have an important bearing in the pathogenesis of PJK. Before corrective surgery of a patient with marked sagittal imbalance, usually the patient will try to bring his forward sight as horizontal as possible, thus increasing his cervical lordosis. To some extent, his cervical lordosis or cervicothoracic spine may be stiff and in a position of extension. Once the lumbar osteotomy has been performed, the patient’s horizontal gaze or sight may be restored through three different mechanisms: forward trunk flexion around the hip (or hip flexion), flexion of the cervical spine (if not stiff) or the spine may bend above the top of the instrumentation in order to bring the head to a more neutral position and with the possibility of a horizontal sight or gaze. Along with flexion/extension of the lumbar spine, we get a better understanding of the adaptive mechanism of the cervicothoracic spine by asking flexion/extension of these areas, preferentially in supine position with underlying rolls for maximal extension and underlying pillow under the head and flexion of the hips and knees in the so-called “parcel-position” for maximal flexion.
Neurological parameters
Some situations, like Parkinson’s syndromes, are very challenging for the spine surgeon and surgery for these patients may often result in instrumentation failure or the presence of a new imbalance [23, 24] (Fig. 8).
Factors where the surgeon may have some limited control
Levels of fusion to be instrumented
If the surgeon is free to pick whichever level for the instrumentation, usually the upper and the lower end vertebrae of the curve or kyphotic deformity are determined. However, some rules of spinal deformities and spine surgery may dictate other choices. PJK has been shown to increase in case of a fusion to the sacrum. However, there may be in many cases no choice, because a fusion to the sacrum cannot be avoided due to significant degenerative changes in the lowest lumbosacral segments. Many of these adult deformities may require a fusion to the sacrum or the pelvis to immobilise the severely degenerated lumbar and lumbosacral spine. For instance if the disc L5/S1 shows severe degeneration and sometimes in functional X-rays air inclusion, indicating a certain pathological movement in this segment, then a fusion in these elderly patients to the sacrum or even to the pelvis, where there is better bone anchorage for the screws, is inevitably necessary. Likewise, if the judged malalignment of the spine is too severe, a proper rebalancing of the spine is only possible, specifically in elderly people with osteoporosis, by including the sacro-pelvis which can be considered as an additional, most distal, big vertebra. Protecting the sacral fixation with iliac screw (uni- or bilateral) will prevent sacral insufficiency fracture too often observed in elderly patients after fusion to only S1. Initially it was also thought that if the spine instrumentation would stop at T10 (at the bottom of the rigid thoracic spine), PJK would be less likely. Literature has failed to support this and fusion to T11, T12 or L1 provided in most cases identical results, provided no focal kyphosis at these levels exists. It is most important to observe whether in the thoracic spine there is osteophyte formation bridging the intervertebral space, since this may prevent or decrease the rate of PJK. However, if this is not sure, then it is recommended to go as high as possible with the thoracic fixation in extremes to T2 or T3 in order to avoid such a junctional kyphosis. This fixation may be done with a technology, which is less rigid, like for instance sublaminar banding in the form of universal clamps (Fig. 8) and prophylactic augmentation of vertebral bodies (Fig. 11). However, all this technology support has not been proven until today in a bigger series to be reliable and sufficient to avoid in any case a PJK.
Decrease of stiffness of the instrumentation
Too stiff instrumentation has been recognised as a cause of junctional kyphosis proximally as well as distally. The stiffness can be modified in different ways:
Choice of metal
Obviously decreasing the stiffness of the instrumentation logically could help prevent the junctional kyphosis. This would mean decreasing the diameter of the rod and using more titanium instrumentation and less stainless steel and/or chrome cobalt. However, concerns for rod breakage, especially if an acute bend has been given to the rod, could be observed.
Choosing a composite metal
One of the options could in theory be using two different types of metal: for instance for a long fusion to the sacrum, one could use a strong and stiff instrumentation for the lumbosacral pelvic reconstruction and use cross connectors connected to a less rigid rod for the thoracic spine. However, also in this case, fatigue fractures of the rods, specifically at the connector site, may occur.
Using less implants
In order to decrease the stiffness of the instrumentation, one may have to think about using other implants than screws: If one is using screws, it may be advantageous, close to the end of the instrumentation, to leave some segments free without any pedicle screws, so the rod keeps its elastic movement and the whole construct is less stiff. The use of hooks has been advocated for instance for this purpose at the top of the instrumentation to create a smooth transition. The issue is, transverse process hooks do not have a very good purchase in osteoporotic spine and it may be better to use laminar or pedicle hooks. There is, however, always the risk that those hooks break or tear through the osteoporotic bone.
The use of sublaminar wires or now sublaminar tapes or bandings may decrease the overall rigidity and help create a more harmonious profile (Fig. 8).
Creating a transition from stiff instrumentation to a suppler one is probably the answer to some of the PJK we have created with too rigid instrumentation (Fig. 11) [25]. Overall we are faced with multiple different choices of metals and transition methods, but we still do not know which ones are most effective in preventing junctional kyphosis, since there is no series of homogenous case observational studies.
Leaving the rods slightly too long proximally has been one of our practice when stopping the fusion for instance at T10 in patients where the likelihood of PJK is high. If they do develop PJK a revision extension of the instrumentation to the upper thoracic spine is easy with simple connectors to the rods left long (Fig. 2 and 7).
Connecting to previous instrumentation: It has been our experience that in order to prevent IJK one must always connect to a previous instrumentation. We mean that we should never leave a portion (or intercalary segment) without instrumentation. The issue is the choice of metal (to connect to the previous instrumentation) as chrome cobalt and stainless steel are not compatible, however, titanium instrumentation can always be used for this purpose and the use of cross connectors, or side to side wedding bands should be used to prevent IJK.
Achieving a strong fixation at the upper end vertebra
Too often the UIV will fail, with either pullout of the pedicle screw or fracture of the vertebra itself or through the pedicle (Fig. 2). In order to avoid such a problem, some authors have advocated the need to cement the top instrumented vertebra with augmentation of the pedicle screws (Fig. 11). This may not prevent fracture of the UIV in all the cases, as we observed it once and as it has been demonstrated in the recent case report in the literature [26]. The disadvantage of cementing the pedicle screw at the top is that it creates a very stiff UIV and may be responsible for topping off above. This is one of the reasons why some authors advocate the need to cement the vertebra above the UIV, too, so there is a strong and mobile transition between the instrumented and non-instrumented spine (Fig. 11). The answer to these problems may be the use of cement with hooks and/or sublaminar wires and creation of smooth transitions (Fig. 11).
Performing osteotomies
Location of the osteotomies: little is known of the impact of spinal osteotomies on the induction of junctional kyphosis. Nothing has been written in the literature about the location of osteotomies and the incidence of PJK. Intuitively, one could think that the more distal the osteotomy is located, the less likely this could induce a PJK. Sixty to eighty percent of the lordosis is normally between L4 and S1 and therefore one should aim for creating the optimal lordosis in the lower lumbar spine.
The types of osteotomies and the incidence of PJK have not been clarified yet. Is it better, in order to avoid junctional kyphosis, to perform a unique osteotomy (Pedicle subtraction osteotomy (PSO)) that corrects the spine up to 30° of malalignment or is it better to perform several small osteotomies (Smith-Petersen osteotomies) at multiple levels? Another advantage of creating osteotomies distally is that they are more likely to help rebalance the patient with less correction needed. The disadvantage to perform them distally at L4 or L5 is that it is often the place of previous laminectomy and osteotomies have to be done through scar tissue. Additionally, L4 and L5 are deeper to access and nerve root injuries or bruises may have greater consequences than osteotomies done higher up in the lumbar spine. However, osteotomies done higher up in the lumbar spine or even at the thoracolumbar junction have the risk of creating cord damage at the conus level.
Location of the correction
In order to rebalance a patient in the sagittal plane, one can increase the lumbar lordosis of the patient and/or decrease the thoracic kyphosis. As the patient is aging, the thoracic kyphosis naturally gets worse through bone creeping process independently of previous operations. This leads to progressive change in the adjacent intervertebral discs with even further kyphosis [27]. The risk, therefore, to correct the sagittal imbalance through correction of the thoracic kyphosis is therefore to see the segments above the instrumentation to go into kyphosis with PJK. In the adult patients we rebalance the spine by restoring the natural lumbar lordosis with preservation of the thoracic kyphosis (except in cases of severe hyperkyphosis). Roussouly [19] recommends to preserve the thoracolumbar kyphosis in patients with high pelvic incidence.
Where to stop the instrumentation
In the adult population and even more so in the elderly, the upper UIV choice must be in most cases on a neutral vertebra and the instrumentation should encompass the whole sagittal Cobb angle. This is true also for the LIV. It is therefore admitted that in most cases one should not stop the instrumentation at the middle of the thoracic kyphosis (T7) but rather in the upper thoracic spine. Therefore, several choices are possible: Choose the thoracolumbar junction and stop at L1, T12, T11 or T10 or bring the instrumentation to the upper thoracic spine, i.e., to T2 or T3. However, which vertebra is less lightly to lead to a PJK and to the best functional result, there is very little established knowledge in this regard and there are also no guidelines that can be applied.
Destruction of the soft tissue at the UIV
Destruction of the ligament and soft tissue at the top of the instrumentation has been recognised as a risk factor of PJK: In order to decrease the risk, some obvious precautions should be taken. This is also true for the LIV. Proximal facets should be left intact during the proximal instrumentation. Likewise, supra- and intraspinous ligaments should be left intact. In some cases we agree that it may be a wishful hope when we are dealing with the soft tissue of an elderly patient with previous spine surgery where this tissue has a very low quality and no mechanical strength. In addition, very often the muscles are fatty degenerated. The instrumentation itself may destroy the soft tissue at the level of the UIV or LIV. A trend that is now observed is to use on top of the instrumentation transverse process hooks, so we do not destroy the soft tissue of the UIV. This can be done also with properly positioned pedicular hooks, which are more resistant to breaking out than transverse process hooks. The pedicular hooks can be combined as hook-screw construct and the whole midline with the supraspinous and interspinous ligaments can be spared from the preparation.
Achieving the perfect balance
As deformity surgeon, we think that we never create enough lumbar lordosis: To some extent this may be true in many cases. This allows correction of the sagittal malalignment. Lack of lumbar lordosis has been shown to correlate with poorer outcomes and therefore with the undercorrection of sagittal malalignment. However, looking at the overall elderly population, it is a well-known fact that a lot of the elderly population have a sagittal malalignment and yet still perform their daily activities well and do not require any treatment. It can only be emphasised that before we decide for any surgery we have to analyse the clinical picture of the patient in depth and compare it with the imaging and never operate on imaging alone. It may be better in many instances to achieve a compensated balance (plumb line between femoral head and sacrum) with less aggressive surgery, than a perfect sagittal balance (plumb line over the posterosuperior aspect of S1) that will require more extensive surgery and/or osteotomies.
The literature tells us that greater sagittal axis change exposes to PJK [28]. This is to some extent a synonym: worse the problem is initially, before any surgery, more likely we will have a problem after (here in the form of a PJK). However, we know that insufficient correction of the sagittal malalignment will expose to PJK as well as distal junctional deformity, but also overcorrection and too much lumbar lordosis may expose to junctional kyphosis too, as the compensation mechanism of the trunk will be to bend right above the instrumentation.
Therapeutic
Once the junctional problem has been identified one should first evaluate the patient clinically and try to identify the causes of the problem that led to the junctional problem: this has been extensively described above in the prophylactic measures. Very often nothing needs to be done if patient is little or asymptomatic (Fig. 5). If symptoms are severe enough or the deformity keeps being progressive revision surgery may be necessary. Such surgeries always require an extension of the instrumentation, in most cases neural decompression (except in younger patients without cord or neural elements compression) and realignment. One of the essential concepts is not to repeat the same mistakes done during the index surgery. Proximally extension of the instrumentation may require to be brought up to the upper thoracic spine or even to the cervical spine. For cervicothoracic PJK a short period of traction may be helpful [29]. Distally the instrumentation will have to be extended past the stenotic segments and stop above the first lordotic discs and will often require to be extended to the sacro-pelvis. Realignment may require all different types of osteotomies either simple SPO, or PSO or even vertebral column resection in some instances. Most revision should start from the posterior approach, but may require after appropriate alignment anterior column support. However, in some cases it may be judicious to start with anterior discectomies with wedge allograft at L4/L5 and or L5/S1 to restore as much as possible the lordosis. Planning osteotomies to achieve the desired sagittal alignment should be calculated and templated knowing that this will require to restore the appropriate lordosis of the lumbar spine. Undercorrection or more rarely overcorrection may lead to further junctional problem or persisting imbalance. The judicial use of instrumentation to prevent further junctional syndrome is recommended making smoother transition between the instrumented and non-instrumented spine, using cement augmentation or sublaminar wires.
Conclusion
Since the literature is still sparse about many aspects of spinal junctional disorders, specifically in the more and more frequently affected adult and elderly population a systematic clinical outcome research in standardised homogenous patient database as well as maybe better understanding of the neuromuscular control of the spine and the spinal balance may help over time to give some answers. As the population is getting older and older and those described problems become an every day problem in spinal services, there is an imperative to focus on this research in the future.
Conflict of interest
None.
Contributor Information
V. Arlet, Email: Vincent.arlet@uphs.upenn.edu
M. Aebi, Email: max.aebi@memcenter.unibe.ch
References
- 1.Jimbo S, Kobayashi T, Aono K, Atsuta Y, Matsuno T. Epidemiology of degenerative lumbar scoliosis: a community-based cohort study. Spine. 2012;37(20):1763–1770. doi: 10.1097/BRS.0b013e3182575eaa. [DOI] [PubMed] [Google Scholar]
- 2.Schwab F, Dubey A, Gamez L, El Fegoun AB, Hwang K, Pagala M, Farcy JP. Adult scoliosis: prevalence, SF-36, and nutritional parameters in an elderly volunteer population. Spine. 2005;30(9):1082–1085. doi: 10.1097/01.brs.0000160842.43482.cd. [DOI] [PubMed] [Google Scholar]
- 3.Aebi M. The adult scoliosis. Eur Spine J. 2005;10:925–948. doi: 10.1007/s00586-005-1053-9. [DOI] [PubMed] [Google Scholar]
- 4.Denis F, Sun EC, Winter RB. Incidence and risk factors for proximal and distal junctional kyphosis following surgical treatment for Scheuermann kyphosis: minimum five-year follow-up. Spine. 2009;34(20):E729–E734. doi: 10.1097/BRS.0b013e3181ae2ab2. [DOI] [PubMed] [Google Scholar]
- 5.Hostin R, McCarthy I, O’Brien M, Bess S, Line B, Boachie-Adjei O, Burton D, Gupta M, Ames C, Deviren V, Kebaish K, Shaffrey C, Wood K, Hart R, International Spine Study Group (2012) Incidence, mode, and location of acute proximal junctional failures following surgical treatment for adult spinal deformity. Spine (Phila Pa 1976) [Epub ahead of print] [DOI] [PubMed]
- 6.Yagi M, Akilah KB, Boachie-Adjei O. Incidence, risk factors and classification of proximal junctional kyphosis: surgical outcomes review of adult idiopathic scoliosis. Spine. 2011;36(1):E60–E68. doi: 10.1097/BRS.0b013e3181eeaee2. [DOI] [PubMed] [Google Scholar]
- 7.Hyun SJ, Rhim SC (2010) Clinical outcomes and complications after pedicle subtraction osteotomy for fixed sagittal imbalance patients: a long-term follow-up data.J Korean Neurosurg Soc 47(2):95–101 [DOI] [PMC free article] [PubMed]
- 8.Kim Y, Bridwell KH, Lenke LG, et al. Proximal junctional kyphosis in adult spinal deformity after segmental posterior spinal instrumentation and fusion. Spine. 2008;33(20):2179–2184. doi: 10.1097/BRS.0b013e31817c0428. [DOI] [PubMed] [Google Scholar]
- 9.Miller DJ, Jameel O, Matsumoto H, et al. Factors affecting distal end and global decompensation in coronal/sagittal planes 2 years after fusion. Stud Health Technol Inform. 2010;158:141–146. [PubMed] [Google Scholar]
- 10.Kwon BK, Elgafy H, Keynan O, et al. Progressive junctional kyphosis at the caudal end of lumbar instrumented fusion: etiology, predictors, and treatment. Spine. 2006;31(17):1943–1951. doi: 10.1097/01.brs.0000229258.83071.db. [DOI] [PubMed] [Google Scholar]
- 11.Barrey C, Roussouly P, Perrin G, et al. Sagittal balance disorders in severe degenerative spine. Can we identify the compensatory mechanisms? Eur Spine J. 2011;S5:626–633. doi: 10.1007/s00586-011-1930-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kim HJ, Lenke LG, Shaffrey CI, et al. Proximal junctional kyphosis as a distinct form of adjacent segment pathology after spinal deformity surgery: a systematic review. Spine. 2012;37(22 Suppl):S144–S164. doi: 10.1097/BRS.0b013e31826d611b. [DOI] [PubMed] [Google Scholar]
- 13.Lewis SJ, Abbas H, Chua S, et al. Upper instrumented vertebral fractures in long lumbar fusions: what are the associated risk factors? Spine. 2012;37(16):1407–1414. doi: 10.1097/BRS.0b013e31824fffb9. [DOI] [PubMed] [Google Scholar]
- 14.Cho KJ, Lenke LG, Bridwell KH, et al. Selection of the optimal distal fusion level in posterior instrumentation and fusion for thoracic hyperkyphosis: the sagittal stable vertebra concept. Spine. 2009;34(8):765–770. doi: 10.1097/BRS.0b013e31819e28ed. [DOI] [PubMed] [Google Scholar]
- 15.Kwon BK, Elgafy H, Keynan O, et al. Progressive junctional kyphosis at the caudal end of lumbar instrumented fusion: etiology, predictors, and treatment. Spine. 2006;31(17):1943–1951. doi: 10.1097/01.brs.0000229258.83071.db. [DOI] [PubMed] [Google Scholar]
- 16.Mac-Thiong JM, Roussouly P, Berthonnaud E, et al. Sagittal parameters of global spinal balance: normative values from a prospective cohort of seven hundred nine Caucasian asymptomatic adults. Spine. 2010;35(22):E1193–E1198. doi: 10.1097/BRS.0b013e3181e50808. [DOI] [PubMed] [Google Scholar]
- 17.Lazennec JY, Brusson A, Rousseau MA. Hip-spine relations and sagittal balance clinical consequences. Eur Spine J. 2011;20(Suppl 5):686–698. doi: 10.1007/s00586-011-1937-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Le Huec JC, Charosky S, Barrey C, et al. Sagittal imbalance cascade for simple degenerative spine and consequences: algorithm of decision for appropriate treatment. Eur Spine J. 2011;20(Suppl 5):699–703. doi: 10.1007/s00586-011-1938-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Roussouly P, Labelle H, Rouissi J et al (2012) Pre- and post-operative sagittal balance in idiopathic scoliosis: a comparison over the ages of two cohorts of 132 adolescents and 52 adults. Eur Spine J [DOI] [PMC free article] [PubMed]
- 20.Lonner BS, Newton P, Betz R. Operative management of Scheuermann’s kyphosis in 78 patients: radiographic outcomes, complications, and technique. Spine. 2007;32(24):2644–2652. doi: 10.1097/BRS.0b013e31815a5238. [DOI] [PubMed] [Google Scholar]
- 21.Lafage V, Ames C, Schwab F, et al. Changes in thoracic kyphosis negatively impact sagittal alignment after lumbar pedicle subtraction osteotomy: a comprehensive radiographic analysis. Spine. 2012;37(3):E180–E187. doi: 10.1097/BRS.0b013e318225b926. [DOI] [PubMed] [Google Scholar]
- 22.Hosman AJ, de Kleuver M, Anderson PG, et al. Scheuermann kyphosis: the importance of tight hamstrings in the surgical correction. Spine. 2003;28(19):2252–2259. doi: 10.1097/01.BRS.0000085097.63326.95. [DOI] [PubMed] [Google Scholar]
- 23.Bourghili A, Guerin P, Vital JM, et al. Posterior spinal fusion from T2 to the sacrum for the management of major deformities in patients with Parkinson disease: a retrospective review with analysis of complications. J Spinal Disord Tech. 2012;25(3):E53–E60. doi: 10.1097/BSD.0b013e3182496670. [DOI] [PubMed] [Google Scholar]
- 24.Koller H, Acosta F, Zenner J, et al. Spinal surgery in patients with Parkinson’s disease: experiences with the challenges posed by sagittal imbalance and the Parkinson’s spine. Eur Spine J. 2010;19(10):1785–1794. doi: 10.1007/s00586-010-1405-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Cahill PJ, Wang W, Asghar J, et al. The use of a transition rod may prevent proximal junctional kyphosis in the thoracic spine after scoliosis surgery: a finite element analysis. Spine. 2012;37(12):E687–E695. doi: 10.1097/BRS.0b013e318246d4f2. [DOI] [PubMed] [Google Scholar]
- 26.Fernández-Baíllo N, Sánchez Márquez JM, Sánchez Pérez-Grueso F et al (2012) Proximal junctional vertebral fracture-subluxation after adult spine deformity surgery. Does vertebral augmentation avoid this complication? A case report. Scoliosis 7(1):16 [DOI] [PMC free article] [PubMed]
- 27.Adams MA, Freeman BJ, Morrison HP, et al. Mechanical initiation of intervertebral disc degeneration. Spine. 2000;25(13):1625–1636. doi: 10.1097/00007632-200007010-00005. [DOI] [PubMed] [Google Scholar]
- 28.Lafage V, Smith JS, Bess S, et al. Sagittal spino-pelvic alignment failures following three column thoracic osteotomy for adult spinal deformity. Eur Spine J. 2012;4:698–704. doi: 10.1007/s00586-011-1967-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.McClendon J, Jr, O’Shaughnessy BA, Sugrue PA, Neal CJ, Acosta FL, Jr, Koski TR, Ondra SL. Techniques for operative correction of proximal junctional kyphosis of the upper thoracic spine. Spine. 2012;37(4):292–303. doi: 10.1097/BRS.0b013e318222dc8a. [DOI] [PubMed] [Google Scholar]