

Abstract
Developing a vaccine against the human immunodeficiency virus (HIV) poses an exceptional challenge. There are no documented cases of immune-mediated clearance of HIV from an infected individual, and no known correlates of immune protection. Although non-human primate models of lentivirus infection have provided valuable data about HIV pathogenesis, such models do not predict HIV vaccine efficacy in humans. The combined lack of a predictive animal model and undefined biomarkers of immune protection against HIV necessitate that vaccines to this pathogen be tested directly in clinical trials. Adaptive clinical trial designs can accelerate vaccine development by rapidly screening out poor vaccines while extending the evaluation of efficacious ones, thereby improving the characterization of promising vaccine candidates and the identification of correlates of immune protection.
Current Status of HIV Vaccines
The four HIV vaccine efficacy trials undertaken in the last 12 years have provided some insights into host immune protection (Figure 1). The first two phase III clinical trials of an HIV vaccine were initiated in 1998 by VaxGen Corp. The vaccine, a gp120 subunit immunogen mixed with alum adjuvant that generated only limited levels of neutralizing antibodies in phase I and II clinical trials, showed no efficacy either in men who have sex with men or injecting drug users (1-4). The next HIV vaccine efficacy trial, the STEP trial initiated seven years later in 2005, evaluated a vaccine that primarily stimulated T-cell immunity with a recombinant adenovirus (Ad5) vector. This immunogen induced robust T-cell responses to HIV gene products found inside the viral particle, as measured by ELISPOT and flow cytometry assays. However, despite the high immunogenicity of this vaccine, there was no reduction in acquisition or long-term control of post-infection viremia (5). Post hoc analyses (6) demonstrated that persons with specific HLA types, as well as those who developed a CD8+ T-cell response to certain Gag and Nef HIV epitopes, exerted immune pressure on the virus in vivo. Unfortunately, post hoc analysis demonstrated an unexpected interaction in those vaccine recipients who were both uncircumcised and immune to Ad5 prior to vaccination. Uncircumcised Ad5-seropositive male recipients experienced an increased rate of HIV infection for the first 18 months after the immunization regimen. This effect fortunately waned over time, such that between months 18 and 36 of follow-up the risk of acquisition among these men equaled that of placebo (5). The mechanism of these vaccine interactions remains undefined.
Figure 1. Timeline of HIV vaccine efficacy trials.

Shown is a time course of the four major clinical efficacy studies of HIV vaccine candidates performed over the past twenty years. The onset and completion of each trial is noted, together with the time required to evaluate efficacy and laboratory analysis. The Vaxgen studies analyzed the efficacy of a gp120 recombinant protein product, whereas the STEP trial evaluated efficacy of Ad5 viral vectors designed to stimulate T-cell immunity. The RV144 Thai trial tested a canarypox protein combination that stimulated CD4+ T cell and antibody responses.
More recently, the RV144 trial of the canarypox/envelope protein prime-boost combination vaccine conducted in Thailand demonstrated a 31% reduction in the frequency of acquisition of HIV infection among vaccinated heterosexual men and women in this low incidence community compared to the control group who received a placebo (7). The RV144 study was a landmark clinical trial in that it provided a proof of concept that a vaccine could prevent HIV-1 infection, although the degree of efficacy was not optimal and must be improved. The trial was initiated in mid-2003, with trial results reported in late 2009 (Figure 1). The success of this vaccine in reducing HIV acquisition has provided the impetus to develop HIV challenge models in non-human primates that mimic key aspects of HIV acquisition in humans. Such endeavors have been problematic previously because of the large number of animals required to conduct such experiments. If such models can be developed and validated, they might provide a useful platform for defining immune correlates for HIV vaccines designed to reduce acquisition of infection. Because of differences between human and non-human primate lentiviral infections, such studies cannot alone serve as the basis for future decision-making in the initiation of clinical trials.
The diversity of the immunological approaches taken by the different vaccine regimens that have entered human clinical efficacy trials highlights the lack of understanding of protective immune responses. Importantly, the long lag between the conduct and analyses of these trials bodes poorly for the development of an HIV vaccine; using this approach it could take decades to develop a globally effective vaccine (Figure 1). Here we suggest a way to link empiricism with laboratory science in order to develop a more rational and faster paced coordinated program for the development of an HIV vaccine.
Defining Immune Correlates of HIV Protection
Currently, there are no biomarkers that define a reduction in the acquisition of HIV infection. As such, no known measurements either in non-human primate models or human phase I/II trials of the frequency or magnitude of a specific immunological response or series of responses after vaccination are predictive of vaccine efficacy. Therefore, one of the major goals and challenges for the HIV vaccine field is to develop correlates of protection against HIV in the most time- and cost-effective way possible, hopefully minimizing the number of costly and lengthy efficacy trials. This is especially important as it is likely that improvement upon the RV144 trial will be incremental. Hence, a systematic program to link reduction in acquisition of HIV infection to an enhanced immune response to the vaccine regimen is needed. To date, the only widely accepted premise for a potentially efficacious vaccine to prevent acquisition of HIV infection is that the vaccine should include the HIV envelope (Env) protein. It also appears that a combination of viral vectors and recombinant subunit proteins may be desirable components of the vaccine. However, the underlying immunological mechanisms by which this combination vaccine regimen might reduce acquisition of HIV remains unknown.
Hypothesis-driven studies (8) in laboratory-based research are straightforward, but their application to human clinical research is more circuitous. Before the question of drug or vaccine efficacy can be answered, safety testing, validation of mechanism, and specificity issues must be addressed in preliminary studies. These studies themselves often provide unexpected information that generates new hypotheses. An efficacy trial, usually a randomized controlled trial, represents the ultimate test of concept that an intervention can ameliorate disease or prevent infection.
Clinical product development typically begins with phase I studies that evaluate the safety and biological activity of a drug, vaccine, or other intervention and proceeds ultimately to phase III efficacy trials that support licensure. The traditional pathway of product development consists of a series of “critical path” trials conducted according to individual protocols that generate and test an explicit hypothesis regarding the clinical efficacy of the intervention. The concept for advancing a drug or vaccine is based on an understanding of molecular and disease pathogenesis and the mechanistic basis for its action. But phase I studies are descriptive, and only begin to evaluate the safety and biological activity of the product under development. Phase II clinical trial evaluation affords an opportunity to discover less frequent side effects of the intervention and to provide better quantitation of the agent’s activity and safety in a larger and more diverse participant population. Increasingly, phase II trials are being conducted in stages, an initial stage exploring the safety and immunogenicity of the vaccine (phase IIa), and a later stage (phase IIb) in which a sufficiently large trial is performed in a population at increased risk for disease in order to provide some indication of efficacy. Such phase IIb studies may supply data that can refute, support, or expand the primary hypothesis and may even generate new hypotheses, creating a loop between the IIb and IIa phases to iteratively define the clinically predictive biomarker endpoints to use in phase IIa. Furthermore, it may be possible to identify an immunological correlate of protection. In the case of an HIV-1 vaccine, this correlate could be the adaptive neutralizing antibody response, CD8+ or CD4+ T-cell immunity, and/or innate immune responses. If such correlates were seen while the trial was in progress, the relevant group sizes could even be expanded to more definitively determine the significance of the correlate and the degree and durability of protection.
The transition from a phase II to a phase III trial allows for a definitive evaluation and a rigorous test of clinical efficacy. In the absence of a validated correlate of clinical efficacy, phase III trials remain critical to the drug or vaccine development process. Such trials are best undertaken when a signal of vaccine efficacy has already been detected in the phase IIb study.
Efficacy Signals from Phase II Trials
Given that we do not have an established immunological correlate of efficacy for an HIV vaccine, we believe that the successful development of an HIV vaccine requires multiple phase IIb hypothesis-generating studies with different HIV vaccine candidates. Using this approach, the hypothesis might be, for example, that broadly neutralizing antibodies confer protection against HIV infection or that T-cell immunity blocks infection at mucosal sites.
The key to progress stemming from phase II trials depends on two elements. First, a positive efficacy signal (such as that in the phase IIb RV144 trial) is essential if further testing of the product in question is to proceed. Such protective responses provide a proof-of-concept for the vaccine candidate. Second, an efficacy signal in a phase II trial might allow the identification of immunological correlates of protection and a strong rationale to proceed to a definitive phase III efficacy trial. The recently licensed vaccine against human papillomavirus (HPV) adopted this approach. A phase II proof-of-concept study with an HPV16 vaccine manufactured by Merck revealed striking efficacy against acquisition of HPV16 infection that correlated with an increase in anti-HPV16 antibodies (9). This observation laid the foundation for a definitive efficacy study with a multivalent HPV vaccine that contains a mixture of capsids from multiple HPV strains.
In the selection of vaccine candidates to enter phase IIb trials for the evaluation of efficacy signals, a rational approach is to prioritize and select candidates based on the hypothesis that the immune responses that they have been demonstrated to trigger will provide protection from established infection. The supporting evidence that should be required to advance a product into a phase IIb study is the validation of a robust response in prior human trials. Although success in nonhuman primate challenge studies can provide some information for prioritization, they have been minimally helpful to date in selecting optimal candidates for advanced testing in humans.
Priority should be given to the selection of vaccine candidates for efficacy trial testing if (1) the candidates test new hypotheses and therefore elicit immune responses that are significantly different, qualitatively or quantitatively, from previous candidates and (2) the candidates are predicted to provide protection based on current understanding of immunopathogenesis. In effect, phase IIb trials, in addition to providing insights into the clinical efficacy of the vaccine candidates, should also explore the different facets of the immune response that may confer protection. Such vaccine candidates may include those that induce neutralizing antibody responses, non-neutralizing antibodies that may interdict transmission at mucosal surfaces, innate immune responses, cell-mediated immune responses directed toward specific viral gene products, or a unique combination of these responses. In other words, the goal of these coordinated trials would be to “fill in the immunological space.”
A key ingredient in developing such coordinated studies is the nature of the study populations and the required degree of efficacy needed to develop an immune correlate. Phase II trials should be powered to demonstrate modest but significant effects, preferably protection from HIV acquisition that is >40% with a lower bound above 0%, and designed to allow for prospective and timely immunological analyses of blood and mucosal samples. Previous phase IIb trials such as the RV144 Thai trial were designed to allow for retrospective immunological analyses that may extend for two years after the completion of the trial, thus precluding rapid access to information that can be important for the design of new clinical trials that test other vaccine candidates. Moreover, the trials should be conducted in populations with a sufficiently high incidence of HIV infection that additional trials or adaptations of the trial can be performed and results obtained rapidly. Future approaches to clinical trial design should take these important issues into consideration.
Adaptive Trial Design
As immunological correlates of protection are critical to the development of an HIV vaccine and as correlates cannot be identified unless there is some degree of an efficacy signal, there is great potential value in accelerating the analysis and iterative design of potentially successful vaccine candidates. Unsuccessful prototypes are best discarded sooner rather than later. Without an immune correlate, relying solely on the traditional iterative clinical trial design is not optimal for the development of an HIV vaccine. Innovative clinical trial designs may prove useful for such decision-making and for prioritization of promising vaccine candidates.
Adaptive trial designs allow modification of the trial in response to data acquired during the study. They require access to evolving clinical data earlier in the process of vaccine development and may accelerate decisions about vaccines (10,11). Adaptive design means that one or more decision points are built into the trial, based upon interim trial results. Adaptations may be divided into two major types: those governed by pre-specified rules and those that make unplanned changes (12). We recommend the first type, which has ample flexibility; the second type may lead to bias, reduced statistical power, and may complicate interpretation of results (13). In general, this means that close monitoring of the trial is performed, allowing an adaptation of the trial after it has begun. This might mean stopping the trial for lack of efficacy, or adapting the trial if efficacy is observed. This adaptation could include vaccinating the placebo group for immune correlate analyses, adding a booster vaccination if vaccine efficacy appears to wane, or expanding the trial design to include a higher risk population. Despite the advantages of adaptive designs, there are certain caveats associated with the approach. For example, decisions may sometimes be based on preliminary data. Care must also be taken to preserve the integrity and objectivity of the trial.
Besides enabling more rapid assessment and elimination of ineffective vaccines, adaptive trial designs also may allow the definition of immunological and virological factors that affect HIV acquisition to be more readily defined. If vaccine efficacy studies are performed in populations with a high incidence of HIV infection, this information can be ascertained more expeditiously, with greater certainty, and possibly with greater cost efficiency. Additionally, if multiple phase II studies can be conducted in parallel, with the capability of examining efficacy endpoints and immune correlates in real time, the likelihood for advancing a successful vaccine to an efficacy trial in a more rapid time frame will increase greatly (Figure 2, lower panel). Moreover, the ability to see common immunological findings either with different vaccine regimens or the same vaccine regimen in different populations (e.g. men versus women) provides more than circumstantial evidence that such responses have an underlying biological basis.
Figure 2. Adaptive trial designs accelerate vaccine development.
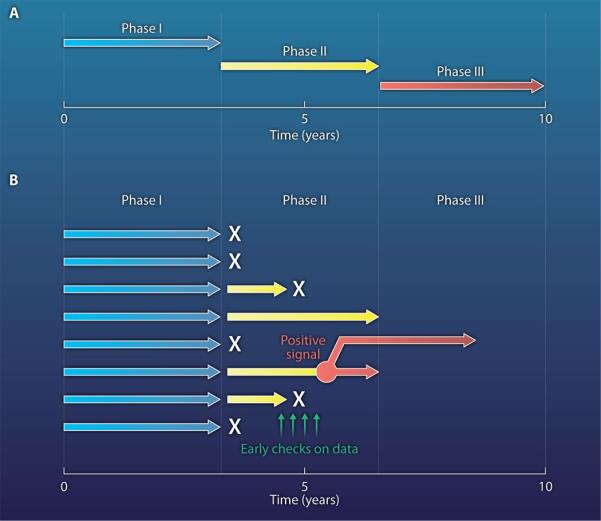
Alternative approaches are needed to assess the clinical efficacy of HIV vaccines. (A) The traditional approach to testing vaccine efficacy is iterative testing in phase I, II, and III clinical trials. (B) In contrast, adaptive trial designs enable real time analysis of immunogenicity and vaccine efficacy. This information can be used to make a decision to proceed to phase III efficacy trials much sooner than with a traditional clinical trial approach. The ability to run multiple trials in parallel and focus on an optimal vaccine candidate could save considerable time by avoiding multiple iterations of the phase I, II and III testing cycle.
Once compelling data supporting a specific hypothesis—e.g. that a defined mucosal antibody response or innate immune signature is associated with reduced acquisition of HIV infection after vaccination—have been solidified through phase II studies, definitive phase III efficacy studies would be warranted. Such a strategic pathway requires a long-term view of HIV vaccine development, otherwise there may be temptations to only test the latest attractive hypotheses in the absence of sufficient data, which may or may not prove valid. Systematic evaluation of vaccine candidates as described above would be the most likely pathway leading to ultimate success.
The RV144 Trial and Future HIV Vaccines
The field now stands at a crossroads and faces two main challenges: how does one build on previous efforts and define parameters for moving forward, and how can the clinical development of an HIV vaccine be accelerated while the field simultaneously addresses basic scientific issues key to the ultimate success of the effort? Continued vaccine-related basic research is needed to provide a better understanding of the complex mechanisms by which HIV establishes infection, evades host immune responses, and is sometimes controlled naturally. Understanding the earliest events in infection, particularly within the first few hours to days at the portals of entry, is a particular priority. Ongoing research on the immunological correlates of protection in the RV144 trial has not yet allowed the field to rule out or to favor any specific cellular or humoral mechanisms of protection. Improvement upon the results of the RV144 trial with other vaccine candidates may require vaccine designs that induce an integrated immune response including innate, cellular, and humoral immunity.
The RV144 trial has provided an important lead with regard to preventing HIV-1 infection. The question now is to determine how best to capitalize on this result and chart the most direct pathway to success. Work is ongoing to aggressively determine any observable immunological correlates of protection in the RV144 clinical trial. This task will be difficult, although hopefully not impossible, due to the small number of clinical samples available. Future clinical trials should have the resources to obtain adequate clinical samples for the real-time study of immune responses generated by the vaccine. The field will also need to intensively investigate vaccine candidates in human efficacy trials that have attributes designed to improve on the results obtained in the RV144 trial. Such attributes might include more potent vectors for expression and immunogenicity of HIV envelope immunogens, and HIV envelope immunogens that can induce durable, broad responses of both traditional neutralizing and non-neutralizing antibodies at mucosal surfaces. The non-human primate SIV infection model is likely to offer important insights into the pathogenic events at mucosal surfaces at the time of transmission. Such studies should be closely linked and coordinated with ongoing clinical trials in humans such that they contribute to the generation and testing of relevant hypotheses. These efforts are consistent and aligned with the approaches and philosophy articulated in the 2010 strategic plan of the HIV Global Vaccine Enterprise (14).
Conclusion
The results from the HIV vaccine efficacy trials conducted in the last 12 years provide optimism that developing an effective HIV vaccine is possible. However, a review of HIV vaccine efficacy trials has indicated that the pace of conduct of such trials is painfully slow and that acceleration of clinical vaccine research is needed. Unfortunately, neither current preclinical non-human primate models or even early phase human clinical trials provide a sound scientific basis for developing data on what types of immune responses or signatures, whether they be humoral, adaptive, or innate, are associated with vaccine-induced protection. Such signatures require close collaboration between sophisticated laboratory investigations and human vaccine efficacy trials. Adaptive trial designs must be implemented if we are to engage in a more systematic and methodical approach to HIV vaccine development. Changing the approach to clinical translational research—from sequential human trials that take years for completion to parallel adaptive hypothesis-generating clinical trials evaluated in real time—can both inform the field with regard to the immunological basis for the prevention of HIV infection and accelerate the path to a highly effective HIV vaccine.
Footnotes
Development of an HIV vaccine could be accelerated by testing candidate vaccines using adaptive clinical trial designs.
REFERENCES
- 1.Flynn NM, Forthal DN, Harro CD, Judson FN, Mayer KH, Para MF. Placebo-controlled phase 3 trial of a recombinant glycoprotein 120 vaccine to prevent HIV-1 infection. J Infect. Dis. 2005;191:654–665. doi: 10.1086/428404. [DOI] [PubMed] [Google Scholar]
- 2.Gilbert PB, Peterson ML, Follmann D, Hudgens MG, Francis DP, Gurwith M, Heyward WL, Jobes DV, Popovic V, Self SG, Sinangil F, Burke D, Berman PW. Correlation between immunologic responses to a recombinant glycoprotein 120 vaccine and incidence of HIV-1 infection in a phase 3 HIV-1 preventive vaccine trial. J Infect. Dis. 2005;191:666–677. doi: 10.1086/428405. [DOI] [PubMed] [Google Scholar]
- 3.Gilbert PB, Ackers ML, Berman PW, Francis DP, Popovic V, Hu DJ, Heyward WL, Sinangil F, Shepherd BE, Gurwith M. HIV-1 virologic and immunologic progression and initiation of antiretroviral therapy among HIV-1- infected subjects in a trial of the efficacy of recombinant glycoprotein 120 vaccine. J Infect. Dis. 2005;192:974–983. doi: 10.1086/432734. [DOI] [PubMed] [Google Scholar]
- 4.Pitisuttithum P, Gilbert P, Gurwith M, Heyward W, Martin M, van Griensven F, Hu D, Tappero JW, Choopanya K. Randomized, double-blind, placebo-controlled efficacy trial of a bivalent recombinant glycoprotein 120 HIV-1 vaccine among injection drug users in Bangkok, Thailand. J Infect. Dis. 2006;194:1661–1671. doi: 10.1086/508748. [DOI] [PubMed] [Google Scholar]
- 5.Buchbinder SP, Mehrotra DV, Duerr A, Fitzgerald DW, Mogg R, Li D, Gilbert PB, Lama JR, Marmor M, Del Rio C, McElrath MJ, Casimiro DR, Gottesdiener KM, Chodakewitz JA, Corey L, Robertson MN. Efficacy assessment of a cell-mediated immunity HIV-1 vaccine (the Step Study): a double-blind, randomised, placebo-controlled, test-of-concept trial. Lancet. 2008;372:1881–1893. doi: 10.1016/S0140-6736(08)61591-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rolland M, Tovanabutra S, deCamp AC, Frahm N, Gilbert PB, Sanders-Buell E, Heath L, Magaret CA, Bose M, Bradfield A, O’Sullivan A, Crossler J, Jones T, Nau M, Wong K, Zhao H, Raugi DN, Sorensen S, Stoddard JN, Maust BS, Deng W, Hural J, Dubey S, Michael NL, Shiver J, Corey L, Li F, Self SG, Kim J, Buchbinder S, Casimiro DR, Robertson MN, Duerr A, McElrath MJ, McCutchan FE, Mullins JI. Genetic impact of vaccination on breakthrough HIV-1 sequences from the Step trial. Nat Med. doi: 10.1038/nm.2316. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rerks-Ngarm S, Pitisuttithum P, Nitayaphan S, Kaewkungwal J, Chiu J, Paris R, Premsri N, Namwat C, de Souza M, Adams E, Benenson M, Gurunathan S, Tartaglia J, McNeil JG, Francis DP, Stablein D, Birx DL, Chunsuttiwat S, Khamboonruang C, Thongcharoen P, Robb ML, Michael NL, Kunasol P, Kim JH. Vaccination with ALVAC and AIDSVAX to prevent HIV-1 infection in Thailand. N. Engl. J Med. 2009;361:2209–2220. doi: 10.1056/NEJMoa0908492. [DOI] [PubMed] [Google Scholar]
- 8.Nabel GJ. The coordinates of truth. Science. 2009;326:53–54. doi: 10.1126/science.1177637. [DOI] [PubMed] [Google Scholar]
- 9.Koutsky LA, Ault KA, Wheeler CM, Brown DR, Barr E, Alvarez FB, Chiacchierini LM, Jansen KU. Proof of Principle Study Investigators, A controlled trial of a human papillomavirus type 16 vaccine. N. Engl. J. Med. 2002;347:1645–1651. doi: 10.1056/NEJMoa020586. [DOI] [PubMed] [Google Scholar]
- 10.Coffey CS, Kairalla JA. Adaptive clinical trials: progress and challenges. Drugs R. D. 2008;9:229–242. doi: 10.2165/00126839-200809040-00003. [DOI] [PubMed] [Google Scholar]
- 11.Chow S-C, Chang M. Adaptive Design Methods in Clinical Trials. Chapman and Hall/CRC; Boca Raton, FL: 2007. [Google Scholar]
- 12.Emerson SS. Issues in the use of adaptive clinical trial designs. Stat. Med. 2006;25:3270–3296. doi: 10.1002/sim.2626. [DOI] [PubMed] [Google Scholar]
- 13.Food and Drug Administration . Guidance for Industry: Adaptive Design Clinical Trials for Drugs and Biologics, Draft Guidance. U.S. Department of Health and Human Services; 2010. [Google Scholar]
- 14.Council of the Global HIV Vaccine Enterprise The 2010 scientific strategic plan of the Global HIV Vaccine Enterprise. Nat. Med. 2010;16:981–989. doi: 10.1038/nm0910-981. [DOI] [PubMed] [Google Scholar]