

Abstract
The purpose of this study was to investigate the contribution of MSX1 gene to the risk of nonsyndromic cleft lip with or without cleft palate (NS-CL ± P) in the Korean population. The samples consisted of 142 NS-CL ± P families (9 with cleft lip, 26 with cleft lip and alveolus, and 107 with cleft lip and palate; 76 trios and 66 dyads). Three single nucleotide polymorphisms (SNPs: rs3821949, rs12532, and rs4464513) were tested for association with NS-CL ± P case-parent trios using transmission disequilibrium test (TDT) and conditional logistic regression models (CLRMs). Minor allele frequency, heterozygosity, χ2 test for Hardy-Weinberg equilibrium, and pairwise linkage disequilibrium (LD) at each SNP were computed. The family- and haplotype-based association test programs were used to perform allelic and genotypic TDTs for individual SNPs and to fabricate sliding windows of haplotypes. Genotypic odds ratios (GORs) were obtained from CLRMs using R software. Although the family-based TDT indicated a meaningful association for rs3821949 (P = 0.028), the haplotype analysis did not reveal any significant association with rs3821949, rs12532, or rs4464513. The A allele at rs3821949 had a significant increased risk of NS-CL ± P (GOR, 1.64; 95% confidence interval,1.03-2.63; P = 0.038, additive model). A positive association is suggested between MSX1 rs3821949 and NS-CL ± P in the Korean population.
Keywords: MSX1 SNP, Nonsyndromic Cleft Lip with or without Palate, Korean, Association Analysis
INTRODUCTION
Nonsyndromic cleft lip and/or palate (NS-CL/P) is a common congenital craniofacial deformity in humans and is known to be caused by a combination of genes and environmental interactions. The frequency of NS-CL/P is higher in Asian populations (1/500 or higher) than in Caucasian (1/1,000) or African populations (1/2,500) (1-4).
The muscle segment homeobox1 (MSX1) gene at 4p16.1 encodes a DNA-binding sequence and is expressed in spatially-restricted regions of the head during early development. Mutations in this gene have been known to be associated with NS-CL/P, Witkop syndrome, Wolf-Hirschhorn syndrome, and autosomal dominant hypodontia (5-7). In animals, homozygous Msx1-deficient transgenic mice exhibit cleft palate, deficiency of the alveolar bone in the mandible and maxilla, incisor development failure, and arrest of molar development (8, 9). Gong (10) showed that there was misregulation in the expression of the Msx1 gene in embryos of A/WySn mice with cleft palate.
Complete sequencing of MSX1 in humans has revealed several novel mutations, and it is estimated that approximately 2% of NS-CL/P patients carry mutations in this gene (6, 7, 11). There have been several association and linkage studies between MSX1 gene variants and NS-CL/P in humans (12-18). However, in terms of the Korean population, only one article has been published for association and linkage study between MSX1 single nucleotide polymorphisms (SNP) and NS-CL/P.
Park et al. (19) reported significant evidence of linkage in the presence of disequilibrium for 1170G/A of exon 2 and the disease risk decreased with the presence of the A allele (AA genotype: odds ratio, 0.26; 95% confidence interval [CI], 0.10-0.99). However, their study has several limitations as follows: They analyzed only novel SNPs with low occurrence frequency. The samples included cleft lip, cleft lip and palate, and cleft palate only. However, cleft palate only has been regarded as a separated identity etiologically and embryologically from clefts involving the lip with or without the palate (20). In addition, when trio-case with cleft palate only (n = 8) was excluded, the numbers of trio-case with cleft lip with or without palate was relatively small (n = 44; 14 with cleft lip, and 30 with cleft lip and palate).
Therefore, it is needed to determine the association and linkage relationship about tag SNPs in the Korean population and to confine the samples with nonsyndromic cleft lip with or without cleft palate (NS-CL ± P) in order to get meaningful results for epidemiologic studies of cleft patients. The purpose of this study was to investigate the contribution of the MSX1 gene to the risk of NS-CL ± P in the Korean population, whose samples are independent form those of Park et al. (19). We tested three tag single nucleotide polymorphism (SNP) markers in and around the MSX1 gene in Korean NS-CL ± P case-parent families using the transmission disequilibrium test (TDT) and conditional logistic regression models (CLRM).
MATERIALS AND METHODS
Subjects
The sample population consisted of 142 Korean NS-CL ± P families (90 males and 52 females; 9 with cleft lip, 26 with cleft lip and alveolus, and 107 with cleft lip and palate; 76 trios and 66 dyads, Table 1). Five orthodontists performed clinical investigation to diagnose NS-CL ± P. For mutation analysis and case-control studies, peripheral venous blood samples of patients and their parents were collected at either Seoul National University Dental Hospital (SNUDH) or Samsung Medical Center (SMC).
Table 1.
Demographic information of gender and cleft type
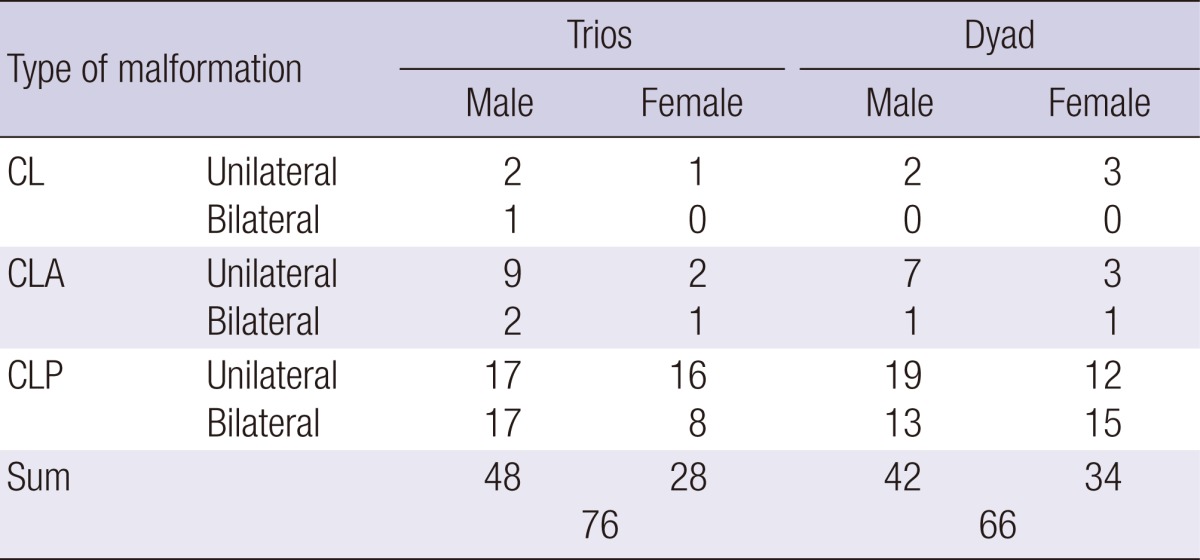
Each numerical number is the number of actual patient with CL, CLA, and CLP. CL, cleft lip only; CLA, cleft lip and alveolus; CLP, cleft lip and palate.
Extraction of genomic DNA and genotyping
Genomic DNA samples were extracted from peripheral venous blood lymphocytes using a commercial DNA extraction kit (Quiagen Inc., Valencia, CA, USA) and were genotyped using VeraCode Technology® (Illumina Inc., San Diego, CA, USA) at SNP Genetics Inc. (Seoul, Korea).
Selection of SNPs
SNP markers located from 2kb-5' to 2kb-3' of the MSX1 gene were obtained from literature review and the NCBI dbSNP database (http://www.ncbi.nlm.nih.gov/SNP/). Among tag-SNPs covering all SNPs in the MSX1 gene, three SNP markers with minor allele frequency (MAF) greater than 1% in the Japanese population (rs3821949, rs12532, and rs4464513) were selected using the web-based program TAG SNP selection (TagSNP; http://snpinfo.niehs.nih.gov/guide.htm#snptag) (21).
These SNPs achieved high "design scores" (a predictor of usable genotypes provided by Illumina Inc., San Diego, CA, USA). Their heterozygosity was greater than 0.1 in the Japanese population (www.hapmap.org/index.html.en). The genotype call rate and sample call rate were considered acceptable at ≥ 95%. Primers for each SNP were synthesized using Oligator technology (Illumina Inc.).
Statistical analysis
The MAF, heterozygosity, and χ2 test for the Hardy-Weinberg equilibrium (HWE) at each SNP were computed using the genotypes of parents. Pairwise linkage disequilibrium (LD) was computed as both D' and r2 for all SNPs using the Haploview program (http://www.broad.mit.edu/mpg/haploview/index.php/)(22-24).
The family-based association test program was used to perform allelic and genotypic transmission disequilibrium tests (TDTs) for individual SNPs and the haplotype-based association test program was used to fabricate sliding windows of haplotypes consisting of two and three SNPs (http://www.biostat.harvard.edu/fbat/default.html) (24, 25). The permutation option (26) was used to obtain empirical P values for observed versus expected transmission and to compute the -log10 P value for each SNP/haplotype within the MSX1 gene.
Genotypic odds ratios (GORs) for heterozygotes and homozygotes under additive, dominant, and recessive models were calculated separately for individual SNPs. A matched case-control dataset was generated with each NS-CL ± P case matched to three possible pseudo-control subjects created from the non-transmitted parental allele (24). The GORs were obtained from conditional logistic regression models for matched sets using publicly available subroutines in the R software (www.r-project.org).
Ethics statement
The study protocol was reviewed and approved by the institutional review board at each institution (SNUDH IRB CRI-G07002 and SMC IRB #2007-08-086, respectively). Informed consent was received from each subject before the sampling.
RESULTS
Demographic information for proband gender and cleft type
One hundred forty-two Korean NS-CL ± P families had 76 trios and 66 dyads. The cases included 90 males and 52 females; 9 with cleft lip (CL), 26 with cleft lip and alveolus (CLA), and 107 with cleft lip and palate (CLP) patients (Table 1).
MAF, heterozygosity, HWE, and LD analyses
The MAF for rs4464513 was lowest (0.295), while the MAFs for rs12532 and rs3821949 showed values of 0.359 and 0.484, respectively. None of the three SNPs exhibited any evidence of deviation from HWE (Table 2). Among three SNPs, the values of Pairwise LD (D'/r2) for pairs of rs3821949-rs12532, rs12532-rs4464513, and rs3821949-rs4464513 were 0.56/0.16, 0.74/0.21, and 0.97/0.71, respectively.
Table 2.
Marker information and transmission disequilibrium test (TDT) results for three single nucleotide polymorphisms (SNPs) in the MSX1 gene in cleft lip with or without cleft palate (CL±P) in 142 CL±P families

*Over-transmitted alleles are in bold type; †Transmission/non-transmission counts from heterozygous parents; ‡Significant P values for individual SNP and global P values for sliding windows of haplotypes of two and three SNPs from TDT analyses; §P < 0.05. MAF, minor allele frequency; HWE, Hardy-Weinberg equilibrium; TDT, transmission disequilibrium test; SNP, single nucleotide polymorphism.
TDT analyses for individual markers and haplotypes
Although the family-based TDT using individual SNPs indicated a significant association for rs3821949 (P = 0.028, Table 2), the haplotype analysis did not reveal any significant association with rs3821949, rs12532, or rs4464513 (Table 2). Because three SNPs used in this study are tag SNPs which are independent of each other, there was no synergic interaction between these SNPs and significance in haplotype analysis could not be exhibited.
Genotypic odds ratios (GOR)
The A allele at rs3821949 had a significant increased risk of NS-CL ± P in an additive model (GOR, 1.64; 95% CI, 1.03-2.63; P = 0.0384, Table 3).
Table 3.
Genotypic odds ratios (GORs) for heterozygotes and homozygotes for individual SNPs in 76 NS-CL±P trios

LD represents linkage disequilibrium; CI, confidence interval. *'N' and 'n' refer to the number of subjects carrying the genotype and the number of case/pseudo-control sets generated, respectively; †P values of χ2 tests for the conditional logistic regression model for each SNP; ‡P < 0.05.
DISCUSSION
Single marker analysis and genotypic odds ratio analysis in the present study exhibited that rs3821949 has a meaningful P value (P = 0.028, Table 2) and an increased risk of NS-CL ± P under an additive model (GOR, 1.64; 95% CI, 1.03-2.63; P = 0.038, Table 3). Huang et al. (27) also reported similar results for rs3821949 in the Han Chinese population living in Western China. However, if the number of samples were to be increased, there may be a more significant association in rs3821949 when considering the relatively low frequency (2%) of MSX1 mutations in NS-CL/P patients (6, 7). There is no reported result about association between MSX1 rs3821949 and NS-CL ± P in non-Asian population until now. Therefore, it is needed to confirm the ethnic differences in other populations.
In this study, the A allele at rs3821949 appears to increase the risk of NS-CL ± P, while the G allele is under-represented (Tables 2, 3). Huang et al. (27) suggested that the cleft lip and palate (CLP) patients showed a significant difference in allele frequency of rs3821949 (GG vs GA/AA) compared to cleft lip (CL) and cleft palate only (CP) patients. Therefore, further study is needed to investigate whether the association of SNP in rs3821949 is different according to cleft type with a large number of cases.
Numerous previous studies have investigated the role of the MSX1 gene in the etiology of NS-CL/P in different human populations (12, 27-30). Among the proposed pathogenic mutations, a rare SNP, P147Q, has been a mutation of interest. It has been found in approximately 2% of Vietnamese (7) and 1.2% of Han Chinese (27). However, Tongkobpetch et al. (11) reported that the P147Q mutation could not be pathogenic because there was no association between the P147Q variant and NS-CL/P in the Thai population. Since this study tested only three SNPs whose MAF was greater than 1.0% in the Japanese population (rs3821949, rs12532, and rs4464513) (21), the P147Q variant was not included as a SNP in the MSX1 gene in this study. Therefore, further study of the association of the P147Q variant with NS-CL/P in the Korean population might be needed.
The cause and time of formation of clefts vary; cleft lip and alveolus (CLA) results from fusion failure between the medial nasal process and maxillary process in the primary palate (lip and premaxilla), which takes place during the fourth to the seventh week of gestation; cleft palate (CP) results from fusion failure between the palatal processes in the secondary palate, which develops during the seventh to the twelfth week (20). Therefore, the developmental classification between CLA and CLP is needed for epidemiologic studies of cleft patients. However, considering the number of samples in the present study (cleft in the primary palate [n = 35; 9 with cleft lip and 26 with cleft lip and alveolus] and cleft in the primary and secondary palate [n = 107 with cleft lip and palate], Table 1), it is needed to increase the number of the cleft patients with lip and/or alveolus (CL and CLA) for investigating the possibility of difference in association and linkage between MSX1 SNPs and cleft type.
In conclusion, the results from this study suggest a positive association between MSX1 rs3821949 and NS-CL ± P in the Korean population.
ACKNOWLEDGMENTS
The authors thank all participants who donated samples and acknowledge Yu-Jin Seo (Seoul National University School of Dentistry), Ah-Young Lee (Samsung Medical Center, The Institute of Oral Health Science), Jung Sun Cho (Hallym University College of Medicine) for assisting during this work; and Duk Hwan Kim, Yong Ick Ji, Eunhyun Jung, and Se Young Cho for their contributions concerning DNA preparation for genotyping (Center for Genome Research, Samsung Biomedical Research Institute, Seoul, Korea). The authors declare no conflicts of interest.
Footnotes
This research was supported by the Basic Science Research Program, the National Research Foundation of Korea (NRF 2009-0069859) funded by the Ministry of Education, Science and Technology, Republic of Korea.
References
- 1.Vanderas AP. Incidence of cleft lip, cleft palate, and cleft lip and palate among races: a review. Cleft Palate J. 1987;24:216–225. [PubMed] [Google Scholar]
- 2.Wyszynski DF, Beaty TH, Maestri NE. Genetics of nonsyndromic oral clefts revisited. Cleft Palate Craniofac J. 1996;33:406–417. doi: 10.1597/1545-1569_1996_033_0406_gonocr_2.3.co_2. [DOI] [PubMed] [Google Scholar]
- 3.Mossey PA, Little J. Epidemiology of oral clefts: an international perspective. In: Wysznski DF, editor. Cleft lip & palate, from origin to treatment. New York: Oxford University Press; 2002. pp. 127–158. [Google Scholar]
- 4.Kim S, Kim WJ, Oh C, Kim JC. Cleft lip and palate incidence among the live births in the republic of Korea. J Korean Med Sci. 2002;17:49–52. doi: 10.3346/jkms.2002.17.1.49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Van den Boogaard MJ, Dorland M, Beemer FA, van Amstel HK. MSX1 mutation is associated with orofacial clefting and tooth agenesis in humans. Nat Genet. 2000;24:342–343. doi: 10.1038/74155. [DOI] [PubMed] [Google Scholar]
- 6.Jezewski PA, Vieira AR, Nishimura C, Ludwig B, Johnson M, O'Brien SE, Daack-Hirsch S, Schultz RE, Weber A, Nepomucena B, et al. Complete sequencing shows a role for MSX1 in non-syndromic cleft lip and palate. J Med Genet. 2003;40:399–407. doi: 10.1136/jmg.40.6.399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Suzuki Y, Jezewski PA, Machida J, Watanabe Y, Shi M, Cooper ME, Vietle T, Nguyen TD, Hai H, Natsume N, et al. In a Vietnamese population, MSX1 variants contribute to cleft lip and palate. Genet Med. 2004;6:117–125. doi: 10.1097/01.gim.0000127275.52925.05. [DOI] [PubMed] [Google Scholar]
- 8.Satokata I, Maas R. Msx1 deficient mice exhibit cleft palate and abnormalities of craniofacial and tooth development. Nat Genet. 1994;6:348–356. doi: 10.1038/ng0494-348. [DOI] [PubMed] [Google Scholar]
- 9.Thomas T, Kurihara H, Yamagishi H, Kurihara Y, Yazaki Y, Olson EN, Srivastava D. A signaling cascade involving endothelin-1, dHAND and msx1 regulates development of neural-crest-derived branchial arch mesenchyme. Development. 1998;125:3005–3014. doi: 10.1242/dev.125.16.3005. [DOI] [PubMed] [Google Scholar]
- 10.Gong SG. Phenotypic and molecular analyses of A/WySn mice. Cleft Palate Craniofac J. 2001;38:486–491. doi: 10.1597/1545-1569_2001_038_0486_pamaoa_2.0.co_2. [DOI] [PubMed] [Google Scholar]
- 11.Tongkobpetch S, Siriwan P, Shotelersuk V. MSX1 mutations contribute to nonsyndromic cleft lip in a Thai population. J Hum Genet. 2006;51:671–676. doi: 10.1007/s10038-006-0006-4. [DOI] [PubMed] [Google Scholar]
- 12.Lidral AC, Romitti PA, Basart AM, Doetschman T, Leysens NJ, Daack-Hirsch S, Semina EV, Johnson LR, Machida J, Burds A, et al. Association of MSX1 and TGFB3 with nonsyndromic clefting in humans. Am J Hum Genet. 1998;63:557–568. doi: 10.1086/301956. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Beaty TH, Wang H, Hetmanski JB, Fan YT, Zeiger JS, Liang KY, Chiu YF, Vanderkolk CA, Seifert KC, Wulfsberg EA, et al. A case-control study of nonsyndromic oral clefts in Maryland. Ann Epidemiol. 2001;11:434–442. doi: 10.1016/s1047-2797(01)00222-8. [DOI] [PubMed] [Google Scholar]
- 14.Fallin MD, Hetmanski JB, Park J, Scott AF, Ingersoll R, Fuernkranz HA, McIntosh I, Beaty TH. Family-based analysis of MSX1 haplotypes for association with oral clefts. Genet Epidemiol. 2003;25:168–175. doi: 10.1002/gepi.10255. [DOI] [PubMed] [Google Scholar]
- 15.Jugessur A, Lie RT, Wilcox AJ, Murray JC, Taylor JA, Saugstad OD, Vindenes HA, Abyholm F. Variants of developmental genes (TGFA, TGFB3, and MSX1) and their associations with orofacial clefts: a case-parent triad analysis. Genet Epidemiol. 2003;24:230–239. doi: 10.1002/gepi.10223. [DOI] [PubMed] [Google Scholar]
- 16.Vieira AR, Orioli IM, Castilla EE, Cooper ME, Marazita ML, Murray JC. MSX1 and TGFB3 contribute to clefting in South America. J Dent Res. 2003;82:289–292. doi: 10.1177/154405910308200409. [DOI] [PubMed] [Google Scholar]
- 17.Moreno LM, Arcos-Burgos M, Marazita ML, Krahn K, Maher BS, Cooper ME, Valencia-Ramirez CR, Lidral AC. Genetic analysis of candidate loci in non-syndromic cleft lip families from Antioquia-Colombia and Ohio. Am J Med Genet A. 2004;125A:135–144. doi: 10.1002/ajmg.a.20425. [DOI] [PubMed] [Google Scholar]
- 18.Schultz RE, Cooper ME, Daack-Hirsch S, Shi M, Nepomucena B, Graf KA, O'Brien EK, O'Brien SE, Marazita ML, Murray JC. Targeted scan of fifteen regions for nonsyndromic cleft lip and palate in Filipino families. Am J Med Genet A. 2004;125A:17–22. doi: 10.1002/ajmg.a.20424. [DOI] [PubMed] [Google Scholar]
- 19.Park J, Park BY, Kim HS, Lee JE, Suh I, Nam CM, Kang DR, Kim S, Yun JE, Go EN, et al. MSX1 polymorphism associated with risk of oral cleft in Korea: evidence from case-parent trio and case-control studies. Yonsei Med J. 2007;48:101–108. doi: 10.3349/ymj.2007.48.1.101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Conway H, Wagner KJ. Incidence of clefts in New York City. Cleft Palate J. 1966;3:284–290. [PubMed] [Google Scholar]
- 21.Xu Z, Taylor JA. SNPinfo: integrating GWAS and candidate gene information into functional SNP selection for genetic association studies. Nucleic Acids Res. 2009;37:W600–W605. doi: 10.1093/nar/gkp290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ardlie KG, Kruglyak L, Seielstad M. Patterns of linkage disequilibrium in the human genome. Nat Rev Genet. 2002;3:299–309. doi: 10.1038/nrg777. [DOI] [PubMed] [Google Scholar]
- 23.Barrett JC, Fry B, Maller J, Daly MJ. Haploview: analysis and visualization of LD and haplotype maps. Bioinformatics. 2005;21:263–265. doi: 10.1093/bioinformatics/bth457. [DOI] [PubMed] [Google Scholar]
- 24.Lee JK, Park JW, Kim YH, Baek SH. Association between PAX9 single-nucleotide polymorphisms and nonsyndromic cleft lip with or without cleft palate. J Craniofac Surg. 2012;23:1262–1266. doi: 10.1097/SCS.0b013e31824e27c7. [DOI] [PubMed] [Google Scholar]
- 25.Rabinowitz D, Laird N. A unified approach to adjusting association tests for population admixture with arbitrary pedigree structure and arbitrary missing marker information. Hum Hered. 2000;50:211–223. doi: 10.1159/000022918. [DOI] [PubMed] [Google Scholar]
- 26.Horvath S, Xu X, Laird NM. The family based association test method: strategies for studying general genotype: phenotype associations. Eur J Hum Genet. 2001;9:301–306. doi: 10.1038/sj.ejhg.5200625. [DOI] [PubMed] [Google Scholar]
- 27.Huang YQ, Ma J, Ma M, Deng Y, Li YD, Ren HW, Zhao GZ, Guo SS, Wang YY, Zhang GX, et al. Association between MSX1 variants and oral clefts in Han Chinese in western China. DNA Cell Biol. 2011;30:1057–1061. doi: 10.1089/dna.2010.1208. [DOI] [PubMed] [Google Scholar]
- 28.Jugessur A, Murray JC. Orofacial clefting: recent insights into a complex trait. Curr Opin Genet Dev. 2005;15:270–278. doi: 10.1016/j.gde.2005.03.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Blanco R, Chakraborty R, Barton SA, Carreño H, Paredes M, Jara L, Palomino H, Schull WJ. Evidence of a sex-dependent association between the MSX1 locus and nonsyndromic cleft lip with or without cleft palate in the Chilean population. Hum Biol. 2001;73:81–89. doi: 10.1353/hub.2001.0002. [DOI] [PubMed] [Google Scholar]
- 30.Singh VP, Ramu D. Association of MSX1 799 G>T variant with nonsyndromic cleft lip/palate in South Indian adolescent patients. Int J Paediatr Dent. 2012;22:228–231. doi: 10.1111/j.1365-263X.2011.01184.x. [DOI] [PubMed] [Google Scholar]