

Abstract
Nasopalatine canal cyst may occur within the nasopalatine canal or in the soft tissues of the palate, at the opening of the canal, where it is called the ‘cyst of the palatine papilla’. These are normally asymptomatic, constituting casual radiological findings. We present a case report of a male patient with infected nasopalatine canal cyst seen clinically as swelling over palate. Radiographic interpretation should be thoroughly performed for maxillary anterior region and any occlusal radiograph in routine radiography to screen this entity and must be distinguished from other maxillary anterior radiolucencies by the clinician.
Background
The nasopalatine canal usually contains remnants of the nasopalatine duct, a primitive organ of smell, as well as the nasopalatine vessels and nerves. Occasionally, a cyst is formed in the nasopalatine canal when these embryonic epithelial remnants of the nasopalatine duct undergo proliferation and cystic degeneration.1 It may occur within the nasopalatine canal or in the soft tissues of the palate, at the opening of the canal, where it is called the ‘cyst of the palatine papilla’.2 The nasopalatine canal cyst was first described in 1914 by Meyer. These lesions, also known by other names such as anterior middle cyst, maxillary midline cyst, anterior middle palatine cyst and incisor duct cyst, were regarded as fissural cysts in the past.3 4 The spontaneous proliferation theory appears to be the most likely explanation (a number of studies have reported cystic degeneration in the incisor duct and on the midline of the palate in human fetuses).3 4 Owing to a lack of representative studies, it is not fully clear whether nasopalatine duct cysts (NPDCs) are more common in Caucasians, blacks or Asians.5 This cyst comprises about 1% of all maxillary cysts3 5 with slight male predilection, the mean age being 42.5 years.4 These are normally asymptomatic, constituting casual radiological findings, though sometimes (in 17% of cases) patients report pain due to the compression of structures adjacent to the cyst, particularly when the latter becomes overinfected, or in patients who wear dentures that compress the zone.3 It appears as a well-corticated, round or heart-shaped radiolucency circumscribed to the maxillary interincisal region in the midline. We present a case report of a male patient with nasopalatine canal cyst, quite uncommon among the jaw cysts and an entity of interest to the clinicians which may be overlooked when asymptomatic.
Case presentation
A 35-year-old man reported to the department of oral medicine and radiology with a complaint of pus discharge from the palate for 6 months. The suppuration started spontaneously from the palate in the anterior part as minute drops 6 months previously without any accompanying pain or swelling. The suppuration increased in quantity with time gradually and after 2 months this caused him discomfort in terms of taste and eating food. There was no extraoral swelling or nasal obstruction (figure 1A). Intraoral examination revealed a slight swelling on the anterior palatal aspect where pus could be expressed on palpation of the swelling (figure 1B) which was soft to firm in consistency and non-tender. The maxillary incisors were vital with no carious lesions or associated history of trauma to the teeth.
Figure 1.
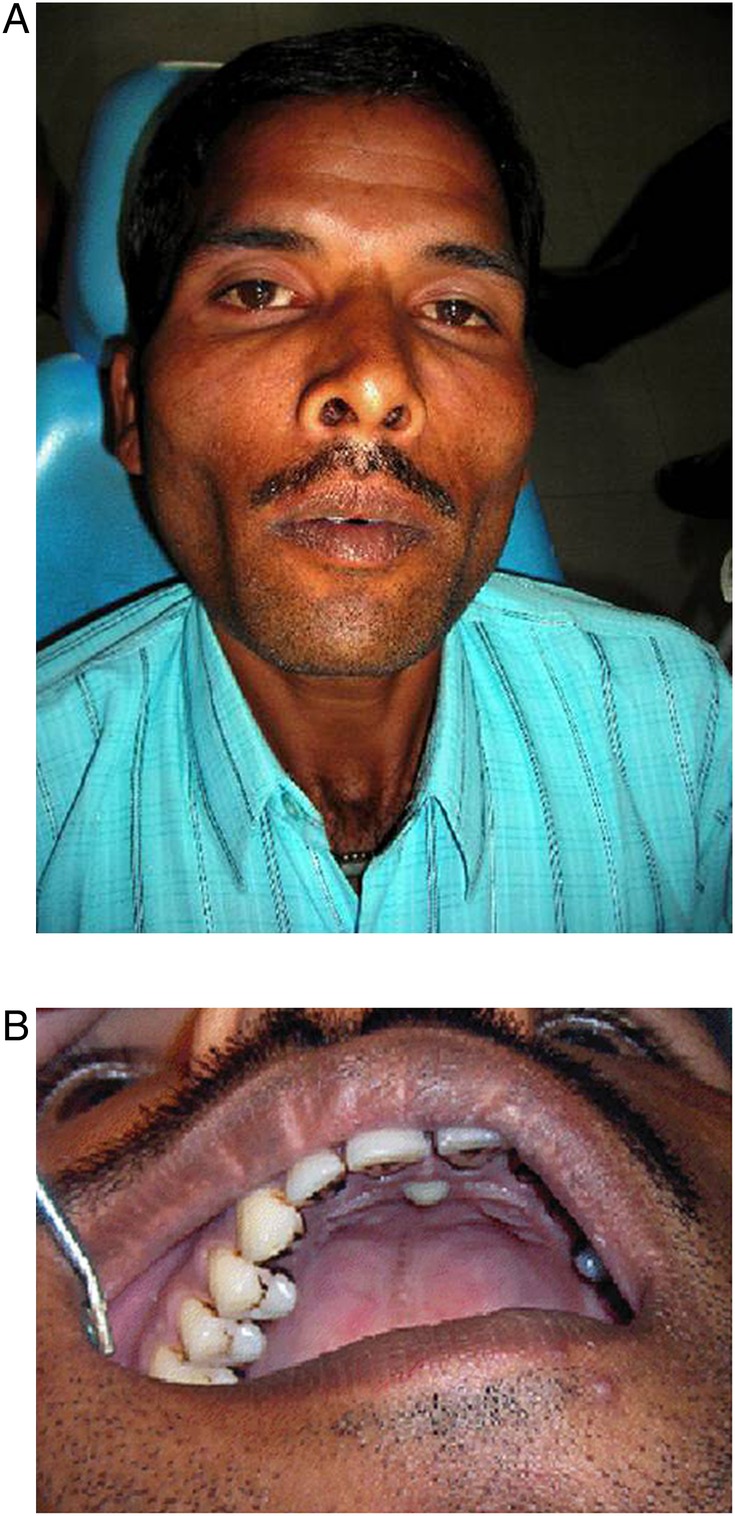
(A) Extraoral photograph of patient. (B) Intraoral clinical photograph.
Investigations
Intraoral periapical radiograph (figure 2) taken for 11, 21 shows a well-corticated radiolucency of size about 1 cm diameter in the midline and above the level of the apices of the teeth.
Figure 2.

Intraoral periapical x-ray
Occlusal radiograph (figure 3) shows the radiolucent area in midline being symmetrical bilaterally in anterior palate. A break in the cortical outline of the radiolucency can be appreciated on the left side in the anterior aspect near the midline. The internal structure of the radiolucency is not completely radiolucent.
Figure 3.

Occlusal x-ray.
Systemic history revealed that he was under DOTS (directly observed treatment, short-course) regimen for pulmonary tuberculosis for 2 months but no symptoms of disease were present.
Blood investigation showed a raised erythrocyte sedimentation rate and eosinophilia.
Microscopic study revealed a fibrous wall lined by thin, non-papillated, cuboidal-to-columnar epithelium. Scattered chronic inflammatory cells are seen in the fibrous wall along with some nerve bundles and blood vessels. A final diagnosis of nasopalatine canal cyst was reached based on clinical, radiographic and histopathological findings.
Differential diagnosis
The differential diagnosis is established with the following conditions:3 6 enlarged nasopalatine duct, central giant cell granuloma, central incisor periapical cyst, other maxillary cysts and osteitis with palatal fistula.
Treatment
Surgical enucleation was performed under local anaesthesia and tissue was sent for histopathological testing.
Discussion
Cysts in the midline of the palate and nasoalveolar or nasopalatine cysts are very uncommon. The cysts in this region are usually an extension of cysts from adjacent regions, which involve or cross the midline.7 The age distribution is broad, with most cases being discovered in the fourth through sixth decades. The incidence is three times higher in males.1–3
Trauma or bacterial infections have been mentioned as possible triggers, but there is very little evidence to support such hypotheses. Although aetiology of this lesion is still uncertain, the NPDC most likely represents a spontaneous cystic degeneration of remnants of the nasopalatine duct and some genetic determinants have been suggested.4 5 In this case the bacterial infection pre-existing in the patient, that is, tuberculosis could be hypothecated as a possible trigger of the lesion.
Most of these cysts are asymptomatic or cause minor symptoms that are tolerated for long periods. A small, well-defined swelling just posterior to the palatine papilla is the most frequent complaint. If the cyst is near the surface, the swelling usually is fluctuant and blue. The deeper nasopalatine duct cyst is covered by normal-appearing mucosa unless it is ulcerated from masticatory trauma.1–7
Expansion of cyst may penetrate the labial plate and produce a swelling below the maxillary labial frenum or to one side. The lesion also may bulge into the nasal cavity and distort the nasal septum. Pressure from the cyst on the adjacent nasopalatine nerves that occupy the same canal may cause a burning sensation or numbness over the palatal mucosa.1 6 8 9
In some cases cystic fluid may drain into the oral cavity through a sinus tract or a remnant of the nasopalatine duct. The patient usually detects the fluid and reports a salty taste.8 9 Most nasopalatine duct cysts are found in the nasopalatine foramen or canal. However, if this cyst extends posteriorly to involve the hard palate, it often is referred to as a median palatal cyst. If it expands anteriorly between the central incisors, destroying or expanding the labial plate of bone and causing the teeth to diverge, it sometimes is referred to as a median anterior maxillary cyst.
This cyst may not always be positioned symmetrically. The periphery usually is well-defined and corticated and is circular or oval in shape. The shadow of the nasal spine sometimes is superimposed on the cyst, giving it a heart shape.1 10 Most nasopalatine duct cysts are totally radiolucent. Most commonly this cyst causes the roots of the central incisors to diverge, and occasionally root resorption occurs. The floor of the nasal fossa may be displaced in a superior direction. The most common differential diagnosis is a large incisive foramen. A foramen larger than 6 mm may simulate the appearance of a cyst. Comparison with previous images may be useful, or aspiration may be attempted, or another image may be made in 6 months to 1 year to assess any change in size. However few cases of median palatine cysts have been reported which may accidentally be found to be present on routine radiographic examination.7 A total of 334 cases have been studied retrospectively to gather demographic, clinical and histological data. Symptoms were present in at least 70% of the cases.11 When symptomatic they present with a swelling on the palate either in midline or adjacent to it, however lying posterior to the incisive papilla. One feature common to this cyst is presence of vital teeth adjacent to the lesion.7
However, these can be confused with the primordial cyst arising from anterior supernumerary teeth, that is, Mesiodens.7 A radicular cyst or granuloma associated with a central incisor is similar in appearance to an asymmetric nasopalatine cyst. The presence or absence of the lamina dura and enlargement of the periodontal ligament space around the apex of the central incisor indicate an inflammatory lesion. A vitality test of the central incisor may be useful.1 5 6 A second periapical view taken at a different horizontal angulation should show an altered position of the image of a nasopalatine duct cyst, whereas a radicular cyst should remain centred about the apex of the central incisor. Nasopalatine duct cysts are treated by surgical enucleation. Recurrence and malignant transformations are rare.12
From the histological perspective, in a study of 22 cases3 the lesions presented exclusively squamous cell epithelium in 15 cases (68.18%), while the remaining 7 cases (31.82%) moreover also showed ciliary cylindrical epithelium. The presence of melanin was observed in one case. The cyst lumen usually contains an abundant inflammatory infiltrate with a great variety of polymorphonuclear leucocytes, secondary to chronic inflammation.5
Learning points.
Nasopalatine canal cysts must be distinguished from other maxillary anterior radiolucencies.
Vitality testing of teeth adjacent to or involved with a cyst-like lesion is mandatory.
Clinician should be aware of the features of this cyst as nearly 40% of the cases are totally asymptomatic and found only during routine clinical examination.
Footnotes
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.White SC, Pharoah MJ. Cysts of the jaws. In: Rudolph P, ed Oral radiology principles and interpretation. 5th edn. St. Louis, USA: Mosby, 2004:400–401 [Google Scholar]
- 2.Shear M, Speight PM. Nasopalatine duct cyst. In: Cysts of the oral and maxillofacial regions. 4th edn. Oxford, UK: Blackwell Munksgaard, 2007:108–113 [Google Scholar]
- 3.Francolí JE, Marqués NA, Aytés LB, et al. Nasopalatine duct cyst: report of 22 cases and review of the literature. Med Oral Patol Oral Cir Bucal 2008; 13:E438–43 [PubMed] [Google Scholar]
- 4.Hegde RJ, Shetty R. Nasopalatine duct cyst. J Indian Soc Pedod Prev Dent 2006;24:31–2 [PubMed] [Google Scholar]
- 5.Pawankumar K, Sholapurkar AA, Joshi V. Surgical management of nasopalatine duct cyst: case report. Rev Clín Pesq Odontol 2010;6:81–6 [Google Scholar]
- 6.Wood NK, Goaz PW. Differential diagnosis of oral and maxillofacial lesions. In: Wood NK and Goaz PW, eds Interradicular radiolucencies. 5th edn. St. Louis, USA: Mosby, 1997:303–305 [Google Scholar]
- 7.Joshi UK, Patil SK, Siddiqua A. Nasopalatine cyst: a rare entity. Int J Dent Clin 2010;2:34–6 [Google Scholar]
- 8.Neville BW, Damm DD, Allen CM, et al. Oral and maxillofacial pathology. In: Developmental defects of the oral and maxillofacial region. 2nd edn. Philadelphia, USA: Saunders, 2005:27–30 [Google Scholar]
- 9.Regezi JA, Sciubba JJ, Jordan RCK. Oral pathology clinical pathologic correlations. In: Rudolph P, ed Cysts of the jaws and neck. 4th edn. San Francisco, USA:Saunders, 2003:256–7 [Google Scholar]
- 10.Cicciù M, Grossi GB, Borgonovo A, et al. Rare bilateral nasopalatine duct cysts: a case report. Open Dent J 2010;4:8–12 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Swanson KS, Kaugars GE, Gunsolley JC. Nasopalatine duct cyst: an analysis of 334 cases. J Oral Maxillofac Surg 1991;49:268–71 [DOI] [PubMed] [Google Scholar]
- 12.Hoseini SV, Khiavi MM, Aghbali A, et al. Unilateral nasopalatine duct cyst, differential diagnosis and treatment plan: a case report. Shiraz Univ Dent J 2011;12:95–9 [Google Scholar]